![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
Personality |
- personality traits are enduring patterns of perceiving, relating to, and thinking about the environment and oneself. |
|
|
Theories of personality |
- humanist- self - psychodynamic: ego, super-ego, ID and psychosexual (Freud) - social cognitive theorists- personality X situation debate. - trait based theories (disposition) - Big 5 |
|
|
Big Five trait based Theory |
- openness to experience. Your receptiveness to new things, trying things ext. - agreeableness. The person tries to get along with others make compromise. - extraversion. The degree to which people like to be with others and interacting with others. - neuroticism. Fears about the way things will turn out. High anxiety. Etc. - contentiousness. Attention to detail responsibilities xcetera. • degree scale: 1 2 3 4 5. |
|
|
Interpersonal circumplex model |
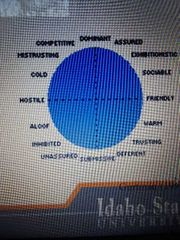
- personality described as a cross between two Dimensions dominance various submissions and friendly Earth hostile. - personality disorders result from extreme variations in the crossing of these dimensions. |
|
|
Personality continuum / medical student syndrome |
- range along Continuum is normal. ● medical student syndrome: - oftenly can relate to or noticed some of the symptoms in ourselves or our clients versus those who meet full criteria. |
|
|
Personality disorder |
• Faith must be inflexible, maladaptive, distressing, and comparing functioning for personality disorder diagnosis. - deviant from individuals culture. - persuasive across contexts by adolescence or early childhood. ( important that we don't give a diagnosis of this in early adolescence or childhood) - cannot diagnose PD under 18 until symptoms are present for at least a year. - cannot diagnose antisocial before 18. |
|
|
Objections to DSM-5 classification of personality disorders |
- disorders are based on categories list of symptoms rather than points along the continuum. Large degree of overlap of diagnostic criteria among different personality disorders. Low reliability for the diagnostic criteria. Classification of personality disorders is a circle atheoretical. Gender bias may be evident in the construction of personality disorders because some symptoms seem to represent extreme stereotypes of masculine or feminine Behavior. |
|
|
DSM-5 General personality disorder criteria |
• an enduring pattern of inner experiences and behavior that deviates markedly from the expectations of the individuals culture and two or more areas: - cognitive / interpreting and perceiving others. - effectivity / range, intensity, lability. - interpersonal functioning. - impulse control. - AND significant impairment. |
|
|
Personality disorders clusters there are three a b c |
• cluster A: odd or eccentric: - paranoid, schizoid, schizotypal - symptoms are similar to schizophrenia, including impairment or flat affect, odd thoughts and speech patterns, and paranoia. • cluster B: dramatic, emotional, erratic: - antisocial, borderline, narcissistic, histrionic - individuals with these PD's often described as prone to manipulation or impulsive, sometimes violent behaviors that show little regard to their own safety or the safety or needs of others. • cluster C: anxious or fearful: - avoidant, obsessive-compulsive, dependent - commonly concerned about being criticized or abandoned. |
|
|
Cluster A: paranoid personality disorder |
•symptoms: - excessive suspiciousness and hostility. - expression / gestures and critical / negative. - preoccupied with the Loyalty / trustworthiness of others. - hold grudges. • more likely to be male. • must present without hallucinations/ delusions. • treatment: offten does not seek treatment. especially not for distrust of others, developed Alliance, avoid direct confrontation, increases self efficacy. |
|
|
Cluster A schizoid personality disorder |
• symptoms: - Detachment and restricted range of emotions. - Movieland limited desire for intimacy, lacks close friends. - indifferent to approval or criticism. • uncommon that they seek clinical treatment. • prevalence rates 3.1 to 4.9% of general population. •3 to 1 male to female ratio in clinical samples. • treatments: focus on social skills training increase awareness of feelings. |
|
|
Cluster A: schizotypal PD |
• symptoms: - cognitive / for sexual disorientation/ eccentric Behavior that are not within cultural practices / norms. ( fantasy not psychosis) - ideas of reference: incorrect interpretations of casual incidents / events as having particular meeting for a person. ( if I see blue before I see red, it means I'm feeling sad) - magical thinking: the idea one can control events with thoughts ( cause Rain by watching Singing in the Rain. If I think nice thoughts about someone then he or she will like me). - unusual mannerisms (odd thinking or speech). - Austin uncomfortable in social interactions. - suspicious of others, lack close friends. • prevalence 6 to 4.6% general population. • 2 to 1 males diagnosed two females. • treatment: low levels of antipsychotic drugs, cognitive therapy address is bizarre thoughts (track in accuracy, help to reject an appropriate or odd beliefs, distinguish fantasy vs reality). • genetic link with schizophrenia (higher heritability and incidents in first-degree relatives of someone with schizophrenia) - similar cognitive deficits as seen in research with individuals with schizophrenia. |
|
|
Cluster B: antisocial PD |
• symptoms (3 +) A. Disregard for the violation of the rights of others. little remorse and different to effect of one's actions on others (occurring since age 15) - no respect for social norms. - deceit / manipulation. - poor impulse control. - irresponsibility. - irritability and aggressiveness. - Reckless disregard for safety of self or others. B. Age 18. C. Conduct disorder diagnosis by age 15. D. Behaviors not in context of schizophrenia or bipolar. • prevalence rate 2.3 to 3.3%. • more frequent in males. So occurs with substance use disorder. • associated with low SES and urban environment. - to what extent should we consider a person social and economic context in making this diagnosis. • lower levels of physiological arousal in response to stress. • treatment: do not generally seek treatment on their own. Some success using a lithium to decrease impulsivity. |
|
|
Cluster B: borderline personality disorder |
-need 5+ or more to be diagnosed. • pattern of in stable and intense interpersonal relationships. • frantic efforts to avoid real or imagined abandonment. Intolerance for being alone. • unstable self-image. Views the self as bad, question one's own existence. • impulsivity: self-harm, risk-taking - link between self-harm and dissociation: and recreate sense of self as real / present. - 69% to 75% resort to self-destructive behaviors ( self harm, drug abuse, bing eting or food restriction, and suicide attempts) • affect instability, dysphoric mood, feelings of emptiness, rage. • history of abuse, neglect, and loss of a parent is more common in people with BPD. • 75% of individuals with diagnosis or females. • 1.6 to 5.9% prevalence rate. • it's your turn to play this memory often show Improvement in first year of treatment after 10 years as many as half no longer meet criteria. ● treatment:DBT dialectical behavior therapy. Skills training in: -- affect regulation and impulse control. -- interpersonal skills. • interpersonal treatment/focus on skills and interpersonal processes. processes. |
|
|
Cluster B: histrionic PD |
• pervasive and excessive emotionality and attention-seeking. • sexually provocative / seductive. Exaggerated emotional presentation. • shallow and rapidly shifting emotions, highly suggestible. • dramatic speech presentation but little detail to support opinions exedra. • Behavior / symptoms cause distress? Cultural context? |
|
|
Cluster B: narcissistic PD |
• symptoms - grandiosity need for admiration. - self-importance / Superior verse Devaluation of others. - entitlement / special treatment. - lack of empathy and lack of recognition of others. - difficulty with criticism or perceived criticism. • demographics: - take age into account these features are common among adolescents. - prevalence rate 1 to 2.9% - 50 to 75% individuals with this diagnosis are male. |
|
|
Cluster C: avoidant PD |
• symptoms: - social inhibition fear of criticism or rejection drives choices in interpersonal relationships, assumes others will be disapproving / critical. - feeling of inadequacy. - hypersensitivity to negative emotion. - restrict lifestyle to avoid risk/new situations, potential for embarrassment. - problems and social and occupational functioning isolated but want acceptance. • awareness of culture, acculturation process. • equal prevalence for men and women. • overlaps with social phobia, generalized type. • overlap with dependent PD. |
|
|
Cluster C: dependant PD |
• symptoms: - pervasive and extensive need to be taken care of / leads to clinging behaviors and fears of separation. - allow / request others make major life decisions. - difficulty expressing disagreement because of a fear of losing others. - make excessive sacrifices rather than risk being alone. - difficulty taking initiative/ low self confidence. • diagnose only if an excess of cultural norms and age-appropriate norms. |
|
|
Cluster C: obsessive-compulsive PD |
• symptoms: - preoccupation with orderliness, perfectionism, and control. --- control via rules, procedures, list or schedules. - perfectionism causes impaired functioning and / or difficulty working with others. -- difficulty with time allotment/ focus on details rather than larger goals leads to inefficiency. - Devotion to work or tasks. - rigid about moral values. Tendency to be rigid. - attentive to "status" of other individuals. Respect authority Terry figures, devalue others. - discomfort with expression of affection. Difficulty paying compliments to others. • 2 times more likely in males. 1.6 to 7.7% prevalence rate. • co-occurrence with hoarding |