![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
409 Cards in this Set
- Front
- Back
|
A 4-year-old boy presents with fever and a sore throat. Examination reveals tonsillitis and a furred tongue with enlarged papillae. There is a blanching punctate rash sparing the face dx |
scarlet fever |
|
|
A 3-year-old girl with a two day history of fever and malaise. Developed a pink maculopapular rash initially on the face before spreading. Suboccipital lymph nodes are also noted |
rubella |
|
|
A 4-year-old boy presents with fever, malaise and a 'slapped-cheek' appearance |
parvovirus b19 |
|
|
Which one of the following is responsible for causing scarlet fever? |
Group A haemolytic streptococci |
|
|
Which of the following conditions is inherited in an autosomal recessive fashion? |
homocystinuria |
|
|
Autosomal recessive diseases mnemonic abcdefgh spw |
a=albinism ,alpha 1 antitrypsin deficiency b=beta thalassemia c=cystic fibrosis,CGD,CAH d=deafness(SNHL),dubin johnson e=enzyme deficiencies(glycogen storage and lysosomal storage) f=friedrich's ataxia, fanconi anemia g=G6PD,galactosemia h=hemochromatosis, homocystinuria s=sickle cell disease p=phenylketonuria w=wilson's |
|
|
Mnemonic for autosomal dominant disorders is "VERy Powerful DOMINANT H(5)uman Families" |
V = Von willibrands disease/ Von hippel lindau E = Ehlers Danlos R = Retinoblastoma, Ramano-Ward syndrome P = Pseudo hypoparathyroidism, Peutz Jeghers syndrome D = Dystrophia myotonica (ie myotonic dystrophy) O = Osteogenesis imperfecta/Osler-weber-rendu M = Marfans syndrome, MEN, malignant hyperthermia I = Intermittent porphyria N = Neurofibramatosis (1&2) A = Achondroplasia, Adult polycystic kidney disease N = Noonans syndrome T = Tuberous sclerosis H = Huntington disease H = Hypertrophic obstructive cardiomyopathy H = Hereditary spherocytosis H = HNPCC H = Hereditary hemorrhagic telengiectasia F = FAP, familial hyperlipidemia/hypercholesteralmia |
|
|
how to remember AD, AR maybe learn the non AR ones as AR is most |
AR are enzyme deficiencies and tend to present earlier in life whereas AD are usually structural problems AD tends to later onset This is just a general rule, but it covers like 90% of stuff. most disease are AR |
|
|
Down syndrome features: complete "CHILD HAS PROBLEM!": |
Congenital heart disease/ Cataracts Hypotonia/ Hypothyroidism Incure 5th finger/ Increased gap between 1st and 2nd toe Leukemia risk x2/ Lung problem Duodenal atresia/ Delayed development Hirshsprung's disease/ Hearing loss Alzheimer's disease/ Alantoaxial instability Squint/ Short neck Protruding tongue/ Palm crease Round face/ Rolling eye (nystagmus) Occiput flat/ Oblique eye fissure Brushfield spot/ Brachycephaly Low nasal bridge/ Language problem Epicanthic fold/ Ear folded Mental retardation/ Myoclonus |
|
|
X-linked recessive mnemonic Be Wise Gold Has False Hope |
Brutons agama, Wiskott aldrich, G6pd, Ocular albinism, Lesch-nyhan, Duchenne, Hemophilia A n B, Fabrys, Hunters |
|
|
tuberous sclerosis key fxs ASH LEAF |
Ashleaf spots Shagreen patches Heart rhabdomyosarcoma Lung hamartoms epilepsy angiomyolipoma in kidney facial angiofibroma |
|
|
good huntington video |
http://www.baronerocks.com/mnemonics/mnemonics-genetics |
|
|
Attention Deficit Hyperactivity Disorder (ADHD) is characterised by |
extreme restlessness poor concentration uncontrolled activity impulsiveness |
|
|
A 2-week-old infant with a small chin, posterior displacement of the tongue and cleft palate |
Pierre-Robin syndrome |
|
|
Supravalvular aortic stenosis is found in a 3-year-old boy with learning difficulties |
William's syndrome |
|
|
A 9-week-old is noted to have a small chin and rocker-bottom feet |
Rocker-bottom feet may also be seen in Patau syndrome but when seen in combination with micrognathia Edward's syndrome is the most likely diagnosis. |
|
|
Patau syndrome (trisomy 13) |
Microcephalic, small eyes Cleft lip/palate Polydactyly Scalp lesions |
|
|
A 2-year-old boy is seen in the Emergency Department with watery diarrhoea for the past two day. What is the most likely causative agent? |
rotavirus (in UK) most common cause |
|
|
A 16-month-old girl is reviewed by her GP. She has a 3 day history of fever and coryzal symptoms. Overnight she has developed a harsh cough. On examination she has a temperature of 38ºC and inspiratory stridor is noticed although there are no signs of intercostal recession. What is the most likely diagnosis? |
croup |
|
|
Infantile colic typically occurs in infants less than 3 months old true/false |
true Infantile colic describes a relatively common and benign set of symptoms seen in young infants. It typically occurs in infants less than 3 months old and is characterised by bouts of excessive crying and pulling-up of the legs, often worse in the evening Infantile colic occurs in up to 20% of infants. The cause of infantile colic is unknown |
|
|
School exclusion is not advised for children with head lice true/false |
true head lice dx fine-toothed combing of wet or dry hair tx malathion, wet combing, dimeticone, isopropyl myristate and cyclomethicone |
|
|
The chance of a 35-year-old mother giving birth to a child with Down's syndrome is approximately: |
1 in 270 |
|
|
Each one of the following statements regarding autism is correct, except: |
The majority of children have normal or increased intelligence |
|
|
Autism All 3 of the following features must be present for a diagnosis to be made |
global impairment of language and communication impairment of social relationships ritualistic and compulsive phenomena other fxs = low iq Associated conditions Fragile X Rett's syndrome |
|

A 14-month-old boy is brought to surgery. Mum says he has been off his food for the past few days and is a bit 'niggly'. His temperature is 37.8degC. dx |
hand, foot and mouth disease caused by intestinal viruses clinical fxs mild systemic upset = sore throat, fever oral ulcers vesicles on palms and soles of feet mgmt hydration and analgesia reassurance go to school |
|
|
Organisms which may colonise CF patients |
Staphylococcus aureus Pseudomonas aeruginosa Burkholderia cepacia Aspergillus |
|
|
embryo |
.. |
|
|
branchial cleft and arch |

|
|
|
A 30-year-old G0P0 woman presents to the gynecologist with a chief complaint of infertility. Over the past year, her and her husband have been attempting to conceive a child without any success. Pelvic exam is unremarkable. A pelvic ultrasound is performed and is shown below |
The source of this woman’s infertility is most likely secondary to a abnormal development of which of the following? Paramesonephric ducts these fuse during 3rd trimester to form uterus and upper 1/3 of vagina |
|
|
A 15-year-old female is brought to the office by her mother because she has not yet had menses. According to patient, she first noticed breast changes roughly 3 years ago, with pubic hair development beginning shortly after. On physical examination, she has Tanner stage 4 breast and pubic development. Chromosome studies reveal a 46, XX karyotype. A pelvic ultrasound reveals the complete absence of a uterus and vagina. The presence of which of the following is most likely responsible for this abnormality? |
Mullerian inhibiting substance this inhibits formation of the uterus and upper 1/3 of the vagina |
|
|
A 9-year-old boy is brought to the pediatrician after his parents became concerned about a painless mass in his neck. Evaluation shows the mass to be cystic and located near the hyoid bone in the midline. It moves when the patient swallows or protrudes his tongue. What is the most likely cause of this mass? |
Failure of the thyroglossal duct to obliterate |
|
|
thyroid gland d/t |
forms from a diverticulum known as median thyroid anlagen located at the tongue duering week 3 gestation as gest. progresses = thyroid gland descends into the neck and fuses with the 4th and 5th branchial pouches (lateral thyroid anlagen) it keeps descending into the hyoid bone and the median enlage is turned into the thyroglossal duct week 5-8 t.duct obliterates and leaves remnant as the foramen cecum (near the tongue) and pyramidal lobe of the thyroid it t.duct doesnt obliterate = cyst |
|
|
A 1-year-old girl is brought in to the emergency room after she started crying uncontrollably and refused feeding. Physical examination shows a cyst near the left outer ear and swelling of the parotid gland on the same side. The physician becomes concerned about the abnormal development of a particular embryonic structure. Which embryonic structure is the physician most likely to be concerned about? |
1st branchial cleft abn. of this can lead to cyst, sinus or fistula near the outer ear and inflammation of the parotid gland |
|
|
learn the structures that arise from the branchial clefts and arches |
... |
|
|
A 31-year-old woman at 37 weeks gestation presents to the emergency department complaining that her water broke one hour ago. After eight hours of attempted labor with no cervical change, she is scheduled for Cesarean section. Apgar scores were 7 at one minute and 9 at five minutes, and there are no abnormal findings on physical examination. The placenta was delivered and on examination is found to have a large hematoma on the maternal side.Which of the following contributes to the maternal side of the placenta? |
decidua basalis |
|
|
A one-week-old infant presents with his mother to the pediatrician’s office with difficulty feeding. The infant gags and becomes cyanotic after each feeding. For the past one day, he has had difficulty breathing at rest. The prenatal period for this infant was complicated by polyhydramnios. Respiratory rate is elevated, and the other vital signs are within normal limits. Physical exam reveals normal head and face. Heart has regular rate and rhythm with no rubs, gallops, or murmurs. Crackles are heard at the bases of both lungs.Which of the following is the most likely developmental abnormality in this infant? |
Tracheoesophageal fistula |
|
|
A 13-year-old girl is brought to the office for evaluation of a painful swelling on the face near the right ear. She says that this started about a week ago and has become progressively more painful and swollen. She denies trauma to the area. Further workup reveals an infected first branchial cleft cyst. She is referred for surgical evaluation.Which below is the most likely complication of the surgery? |
difficulty smiling due to damage to facial nerve in surgery |
|
|
A 31-year-old male with a history of recurrent urinary tract infections presents to the emergency department with flank pain, urinary urgency and dysuria. His temperature is 39.6oC (103.2oF), pulse is 92 beats/min, respirations are 13 breaths/min and blood pressure is 131/84 mm Hg. |
Renal ultrasound shows kidneys fused at the inferior poles.The kidneys are most likely trapped under which artery? IMA |
|
|
A 27-year-old woman comes to the office for her initial obstetric appointment. She has a history of seizures and has been taking phenobarbital daily. She takes no other medications and does not take a multivitamin. Urine hCG is positive. Her last menstrual period was 20 weeks ago, and this date is confirmed by ultrasound. Given her risk factors the physician is concerned about a neural tube defect. Which of the following would be most likely to be elevated in the maternal serum if the fetus has a neural tube defect? |
alpha fetoprotein |
|
|
A 5-day-old neonate is having difficulty with feeding. With every attempt, the baby coughs, regurgitates food, and becomes cyanotic. The patient excessively salivates and occasionally has coughing spasms. Birth history includes a history of maternal polyhydramnios. On physical exam, the patient has a distended abdomen.What is the most likely cause for this patient’s inability to feed? |
fistula formation |
|
|
polyhydramnios is associated with VATER |
Veterbral abn Anal atresia TrachealEso. fistula and Renal dis they present with cough, regurg and cyanosis after times of feeding if the have TE fistula |
|
|
A 7-year-old with a one day history of a painful right hip. Just about able to walk but painful. Looks flushed and has a temperature of 38.7ºC dx |
Septic arthritis/osteomyelitis |
|
|
An 8-month-old child is noted to have a discrepancy between the skin creases behind the right and left hips |
Development dysplasia of the hip |
|
|
An obese 13-year-old boy presents with a two week history of right sided knee pain associated with a stiff right hip. There is no history of trauma |
Slipped upper femoral epiphysis SUFE relates to SLOB (ie obese boy) |
|
|
causes of limping child |
A.Perthes disease B.Septic arthritis/osteomyelitis C.Development dysplasia of the hip D.Trauma E.Slipped upper femoral epiphysis F.Transient synovitis G.Juvenile idiopathic arthritis |
|
|
Transient synovitis |
Acute onset Usually accompanies viral infections, but the child is well or has a mild fever More common in boys, aged 2-12 years |
|
|
Septic arthritis/osteomyelitis |
Unwell child, high fever |
|
|
Juvenile idiopathic arthritis |
Limp may be painless |
|
|
Trauma |
History is usually diagnostic |
|
|
Development dysplasia of the hip |
Usually detected in neonates6 times more common in girls |
|
|
Perthes disease |
More common at 4-8 yearsDue to avascular necrosis of the femoral head |
|
|
Slipped upper femoral epiphysis |
10-15 years - Displacement of the femoral head epiphysis postero-inferiorly ITS THE SAME AS THE DIRECTION YOU PULL THE EAR IN KIDS to look at ear canal |
|
|
Cystic fibrosis is not a cause of hypotonia in infancy true/false |
true |
|
|
hypotonia |
Hypotonia, or floppiness, may be: 1) central in origin - DS, Prada Willi syndrome, hypothyroidism, cerebral palsy (before spasticity) or 2) related to nerve and muscle problems - spinal muscular atrophy, spina bifida, Guillain Barre syndrome, myasthenia gravis, muscular dystrophy, myotonic dystrophy or 3) due to acutely ill child (septicemia) or ischemic encephalopathy in newborns |
|
|
Which one of the following statements regarding scabies is false? |
Patients who complain of pruritus 4 weeks following treatment should be retreated It is normal for pruritus to persist for up to 4-6 weeks post eradication |
|
|
scabies is what type of hypersensitivity rxn |
Scabies causes a delayed type IV hypersensitivity reaction (to mites/eggs that the scabies mite lays in the stratum corneum 30 days after initial infxn) |
|
|
Which one of the following is a risk factor for developmental dysplasia of the hip? |
Oligohydramnios ddh dx = US mgmt 3-6 weeks old = reassurance 4-5 months = pavlik harness older children = surgery |
|
|
Risk factors for DDH |
female sex: 6 times greater risk breech presentation positive family history firstborn children oligohydramnios birth weight > 5 kg congenital calcaneovalgus foot deformity |
|
|
A 10-month-old boy is brought to surgery. Around 4 days ago he developed a fever after being irritable the previous day. The fever settled after around 3 days but following this he developed a rash, which prompted his mother to bring him to surgery. He is taking around 75% of his normal feeds, is producing wet nappies and has had two episodes of loose stools. On examination he is alert, temperature is 37.0ºC, chest is clear, ears/throat unremarkable. There are a number of blanching, rose pink macules present on his trunk. What is the most likely diagnosis? |
Roseola infantum (aka exanthem subitum occassionally sixth disease)- fever followed later by rash caused by herpes 6 virus incubation period = 5-15days usu. 6months to 2yo |
|
|
fxs of roseola infantum infxn |
high fever: lasting a few days, followed by amaculopapular rash febrile convulsions occur in around 10-15% diarrhoea and cough are also commonly seen |
|
|
Other possible consequences of HHV6 infection |
aseptic meningitis hepatitis |
|
|
hormone receptors including ER (E2 receptors) or PR (P4 receptors) |
a hormone receptor assay, a test that tells you whether or not the breast cancer cells have receptors for the hormones estrogen and progesterone. Hormone receptors are proteins — found in and on breast cells — that pick up hormone signals telling the cells to grow.A cancer is called estrogen-receptor-positive (or ER+) if it has receptors for estrogen. This suggests that the cancer cells, like normal breast cells, may receive signals from estrogen that could promote their growth. The cancer isprogesterone-receptor-positive (PR+) if it has progesterone receptors. Again, this means that the cancer cells may receive signals from progesterone that could promote their growth. Roughly two out of every three breast cancers test positive for hormone receptors.Testing for hormone receptors is important because the results help you and your doctor decide whether the cancer is likely to respond to hormonal therapy or other treatments. Hormonal therapy includes medications that either (1) lower the amount of estrogen in your body or (2) block estrogen from supporting the growth and function of breast cells. If the breast cancer cells have hormone receptors, then these medications could help to slow or even stop their growth. If the cancer is hormone-receptor-negative (no receptors are present), then hormonal therapy is unlikely to work. You and your doctor will then choose other kinds of treatment. |
|
|
herceptin |
is a targeted therapy for HER2 Positive Metastatic Breast Cancer and HER2 Positive Gastric Cancer |
|
|
A 45 year old woman presents with a 3cm breast lump. She undergoes a mammogram, biopsy and CT scan for staging. Investigations reveal this to be a single ER+ve, HER2-ve tumour, confined to the breast. What is the next stage of management? |
surgery 1st line for breast cancer if LT 4cm wide local excision (breast conserving surgery) favored tamoxifen is an option AFTER SURGERY as breast cancer is ER +ve |
|
|
tamoxifen |
E2 receptor antagonist (remember the breast cancer cells may have E2 and/or P4 receptors that may promote growth on hormone binding, thus blocking will stop growth) |
|
|
A 4-week-old child is brought to clinic with a red rash on her scalp associated with yellow flakes. What is the most likely diagnosis? |
Seborrhoeic dermatitis |
|
|
What is the most common identified trigger of anaphylaxis in children? |
food Anaphylaxis may be defined as a severe, life-threatening, generalised or systemic hypersensitivity reaction. and then drugs and then venom (eg wasp sting) |
|
|
A 2-month-old girl is brought in by her mother. She was breastfed for the first two weeks of life before being switched to formula. For the past six weeks she has experienced a number of problems including regurgitation, vomiting, diarrhoea and eczema. Despite these problems she has kept to the 50th centile for weight. Clinical examination is unremarkable other than some dry skin on her torso. What is the most likely diagnosis? |
Cow's milk protein intolerance The emergence of symptoms following the introduction of formula is very suggestive of cow's milk protein intolerance is an allergic rxn |
|
|
Withhold benzylpenicillin only in children and young people who have a clear history of anaphylaxis after a previous dose; a history of a rash following penicillin is not a contraindication. true/false |
true |
|
|
A 7-year-old child is brought to surgery by her father after he collected her from school. She was unwell in the morning with a fever and cough but has become gradually worse during the day. His father is panicked because he has noticed a red rash on her legs which doesn't blanch following the 'tumbler test'. The girl is now also complaining of a headache and cool hands and feet. On examination she has a petechial rash on her lower legs and is pyrexial with a temperature of 38.4ºC. Her father reports she is allergic to penicillin. On reviewing the records you note she developed a rash and vomiting after been given amoxicillin for otitis media 4 years ago. dx |
meningococcal septicaemia until proven otherwise get to hospital + give IM benzylpenicillin (remember hx of rash after penicillin is not a CI) |
|
|
A 4-year-old girl is reviewed by her GP due to poor control of asthma. She currently takes a regular steroid inhaler and a salbutamol inhaler as required. What is the next step in management? |
Trial of a leukotriene receptor antagonist |
|
|
Asthma in children: stepwise management BASED ON BTS = Children aged under 5 years |
Step 1 As-required reliever therapy: short-acting beta2-agonist Step 2 Regular preventer therapy: inhaled corticosteroids, 200-400mcg/day* Or, if inhaled corticosteroids cannot be used, a leukotriene receptor antagonist Step 3 Children aged 2-5 years: trial of a leukotriene receptor antagonist. If already taking leukotriene receptor antagonist reconsider inhaled corticosteroidsChildren aged under 2 years: refer to respiratory paediatrician Step 4 Refer to a respiratory paediatrician |
|
|
Asthma in children: stepwise management BASED ON BTS = Children aged over 5 years (similar to adult guidance) |
1 As-required reliever therapy: short-acting beta2-agonist 2 Regular preventer therapy: inhaled corticosteroids, 200-400mcg/day* 3 1. Add inhaled long-acting B2 agonist (LABA) 2. Assess control of asthma: - good response to LABA - continue LABA - benefit from LABA but control still inadequate: continue LABA and increase inhaled steroid dose to 400 mcg/day* (if not already on this dose) - no response to LABA: stop LABA and increase inhaled steroid to 400 mcg/ day.* If control still inadequate, institute trial of other therapies, leukotriene receptor antagonist or SR theophylline 4 Increase inhaled corticosteroids to high-dose, up to 800mcg/day* 5 Use daily steroid tablet at lowest dose providing controlMaintain inhaled corticosteroids at 800mcg/dayRefer to a paediatrician |
|
|
Sudden infant death syndrome |
is the commonest cause of death in the first year of life. It is most common at 3 months of age |
|
|
sudden infant death syndrome risk factors nb Following a cot death siblings should be screened for potential sepsis and inborn errors of metabolism |
prematurity parental smoking hyperthermia (e.g. over-wrapping) putting the baby to sleep prone male sex multiple births bottle feeding social classes IV and V maternal drug use incidence increases in winter |
|
|
You are discussing conception with two parents who both have achondroplasia. They ask you what the chances are that a child of theirs would be of normal height. What is the correct response? |
achondroplasia is a common cause of dwarfism its a autosomal dominant genetic disorder associated with short stature = abn. cartilage thus 25% chance of having a child of normal height nb 1 in 4 chance of an unaffected child 1 in 2 chance of an affected heterozygous child 1 in 4 chance of an affected homozygous child. With achondroplasia children unfortunately don't live past the first few months of life |
|
|
A 4-year-old boy is reviewed in the Paediatric Admissions Unit. He has had a fever for the past week. On examination he has red, sore lips and conjunctival injection. He also has swollen, red hands. Hb is decreased WBC increased Platelets increased CRP sig. increased dx |
Kawasaki disease mainly seen in kids can cause coronary artery aneuryms clinical dx tx -aspirin -IVIg -ECHO - checking for coronary aneuryms nb Kawasaki disease is one of the few indications for the use of aspirin in children. Due to the risk of Reye's syndrome aspirin is normally contraindicated in children. |
|
|
A 6-year-old boy is reviewed in clinic due to nocturnal enuresis. His mother has tried using a star-chart but unfortunately this has not resulted in any significant improvement. Of the following options, what is the most appropriate initial management strategy? |
Enuresis alarm |
|
|
A 2-month-old baby girl is admitted to hospital with suspected meningitis. Her parents describe her becoming pyrexial and drowsy over the past 24 hours. On examination her temperature is 39.2ºC, heart rate is 160/min and respiratory rate is 50.min. Her anterior fontanelle is bulging. No petechial rash is seen. In addition to cefotaxime, what antibiotic should be given intravenously? |
Amoxicillin Meningitis in children LT 3 months: give IV amoxicillin in addition to cefotaxime to cover for Listeria |
|
|
MENINGITIS CI to LP (basically any signs of raised ICP) focal neurological signs papilloedema significant bulging of the fontanelle disseminated intravascular coagulation signs of cerebral herniation |
For patients with meningococcal septicaemia lumbar puncture is contraindicated - blood cultures and PCR for meningococcus should be obtained |
|
|
You see a worried mum with her 6 month old baby boy. She is concerned that his skull shape is not normal. His development and birth have been normal and there are no conditions in the family. On examination his head circumference is at the 40th centile with his height and weight at the 30th centile. His occiput is flattened on the left, his left ear mildly protruding forward and his left forehead more prominent than the right. No other abnormality is detected. What is the most appropriate management? |
Reassurance dx = plagiocephaly = parallelogram shaped head the incidence of plagiocephaly has increased due to sleeping on back nb other skull prob in kids = Craniosynostosis = premature fusion of skull bones |
|
|
The prodrome is characterised by fever, irritability and conjunctivitis dx |
measles |
|
|
May cause vesicles in the mouth and on the palms dx |
Coxsackie A16 causes Hand, foot and mouth disease Mild systemic upset: sore throat, fever Vesicles in the mouth and on the palms and soles of the feet |
|
|
May cause a crop of white spots on the inside of the mouth |
Measles |
|
|
Chickenpox |
Fever initially Itchy, rash starting on head/trunk before spreading. Initially macular then papular then vesicular Systemic upset is usually mild |
|
|
Measles |
Prodrome: irritable, conjunctivitis, fever Koplik spots: white spots ('grain of salt') on buccal mucosa Rash: starts behind ears then to whole body, discrete maculopapular rash becoming blotchy & confluent |
|
|
Mumps |
Fever, malaise, muscular pain Parotitis ('earache', 'pain on eating'): unilateral initially then becomes bilateral in 70% |
|
|
Rubella |
Rash: pink maculopapular, initially on face before spreading to whole body, usually fades by the 3-5 day Lymphadenopathy: suboccipital and postauricular |
|
|
Erythema infectiosum |
Also known as fifth disease or 'slapped-cheek syndrome' Caused by parvovirus B19 Lethargy, fever, headache 'Slapped-cheek' rash spreading to proximal arms and extensor surfaces |
|
|
Scarlet fever |
Reaction to erythrogenic toxins produced by Group A haemolytic streptococci Fever, malaise, tonsillitis 'Strawberry' tongue Rash - fine punctate erythema sparing face |
|
|
Which one of the following statements regarding cerebral palsy is incorrect? |
Less than 5% of children will have epilepsy Children with cerebral palsy often have associated non-motor problems such as: learning difficulties (60%) epilepsy (30%) squints (30%) hearing impairment (20%) |
|
|
causes of cerebral palsy (APE) |
Antenatal = cerebral malfomxn and TORCH Postnatal = IVentricular bleeding, meningitis, head trauma Endonatal (ie intrapartum) = birth asphyxia/trauma |
|
|
cerebral palsy |
It is the most common cause of major motor impairment in children |
|
|
classification of cerebral palsy = MADS |
Mixed Ataxic Dyskinetic Spastic (70%) = hemiplegia, diplegia or quadriplegia |
|
|
A mother brings her 8-month-old infant to the GP due to the development of a nappy rash. On examination an erythematous rash with flexural sparing is seen. What is the most likely cause? |
Irritant dermatitis is the most common cause of nappy rash - due to irritant effect of urinary ammonia and faeces creases/flexures are usu. spared |
|
|
causes of nappy/napkin rash |
irritant dermatitis (most common) candida dermatitis seborrhoeic dermatitis psoriasis atopic eczema |
|
|
fxs of nappy/napkin rash caused by irritant dermatitis |
due to irritant effect of urinary ammonia and faeces Creases are characteristically spared |
|
|
fxs of nappy/napkin rash caused by candida dermatitis |
erythematous rash which involve the flexures and has characteristic satellite lesions |
|
|
fxs of nappy/napkin rash caused by Seborrhoeic dermatitis |
Erythematous rash with flakes. May be coexistent scalp rash |
|
|
fxs of nappy/napkin rash caused by psoriasis |
A less common cause characterised by an erythematous scaly rash also present elsewhere on the skin |
|
|
fxs of nappy/napkin rash caused by |
Other areas of the skin will also be affected |
|

A 1-year-old girl is investigated for recurrent urinary tract infections. A micturating cystourethrogram is ordered: What does this image demonstrate? |
Vesicoureteric reflux gross dilatation of the ureter, pelvis and calyces with ureteral tortuosity. A DMSA scan is needed to identify renal scarring. |
|
|
Vesicoureteric reflux (VUR) definition |
abnormal backflow of urine from the bladder into the ureter and kidney |
|
|
VUR pathophys |
ureters are displaced laterally, entering the bladder in a more perpendicular fashion than at an angle therefore shortened intramural course of ureter vesicoureteric junction cannot therefore function adequately |
|
|
grading of VUR |
I Reflux into the ureter only, no dilatation II Reflux into the renal pelvis on micturition, no dilatation III Mild/moderate dilatation of the ureter, renal pelvis and calyces IV Dilation of the renal pelvis and calyces with moderate ureteral tortuosity V Gross dilatation of the ureter, pelvis and calyces with ureteral tortuosity |
|
|
InV for VUR |
VUR is normally diagnosed following a micturating cystourethrogram a DMSA scan may also be performed to look for renal scarring |
|
|
A 3-year-old child is diagnosed with whooping cough. What is the most appropriate antibiotic therapy? |
oral erythromycin (or azithromycin) |
|
|
dx of pertusis (whooping cough) |
per nasal swab culture for Bordetella pertussis - may take several days or weeks to come back PCR and serology are now increasingly used as their availability becomes more widespread |
|
|
complications of pertussis (whooping cough) |
subconjunctival haemorrhage pneumonia bronchiectasis seizures |
|
|
Bronchiolitis most common cause |
RSV in 75-80% of cases |
|
|
bronciolitis fxs |
coryzal sxs dry cough increased SOB wheezing, fine inspiratory crackles feeding difficulties + SOB |
|
|
bronchiolitis signs suggestd criteria for referral to hospital |
poor feeding (< 50% normal) lethargy apnoea respiratory rate > 70/min nasal flaring or grunting severe chest wall recession cyanosis oxygen saturation < 94% uncertainty regarding diagnosis |
|
|
bronchiolitis InV |
immunofluorescence of nasopharyngeal secretions may show RSV |
|
|
Management is largely supportive |
humidified oxygen is given via a head box for bronchiolitis |
|
|
A 6-year-old boy is noted to have pectus excavatum and pulmonary stenosis during a cardiorespiratory exam. What is the most likely diagnosis? |
Noonan syndrome |
|
|
A mother brings her 2-week-old baby girl into the surgery for review. She has noted a bright red, well-circumscribed and lobulated lesion developing on her right temple. This wasn't noted at birth but is now 5 mm in diameter. What is the most appropriate management? |
Reassure the mother that most lesions spontaneously regress (if tx needed then use systemic steroids) This baby has a strawberry naevus (capillary haemangioma). Treatment is only usually required if the lesion is causing a mechanical problem or bleeding. They appear as erythematous, raised and multilobed tumours. |
|
|
Cavernous haemangioma is a deep capillary haemangioma true/false |
true strawberry naevus is a superficial capillary hemangioma |
|
|
A 2-year-old boy is brought to the surgery by his mother with earache and pyrexia. On examination of the precordium a murmur is heard. Which one of the following characteristics is not consistent with an innocent murmur? |
Diastolic murmur |
|
|
fxs of innocent murmurs |
Short buzzing murmur in the aortic area Soft-blowing murmur in the pulmonary area Varies with posture Continuous blowing noise heard just below the clavicles |
|
|
fxs of innocent (ejection) murmurs |
soft-blowing murmur in the pulmonary area or short buzzing murmur in the aortic area may vary with posture localised with no radiation no diastolic component no thrill no added sounds (e.g. clicks) asymptomatic child no other abnormality |
|
|
innocent murmurs heard in children include |
ejection murmurs = due to turb. flow at outflow tracts venous hums = due to turb. flow in great veins returning to heart = continuous blowing noise heard just below clavicles Still's murmur = low pitched sound heard at lower left sternal edge |
|
|
Which one of the following types of glomerulonephritis is most characteristically associated with streptococcal infection in children? |
Diffuse proliferative glomerulonephritis classical post-streptococcal glomerulonephritis in child presents as nephritic syndrome / acute kidney injury most common form of renal disease in SLE |
|
|
Membranous glomerulonephritis |
presentation: proteinuria / nephrotic syndrome / chronic kidney disease cause: infections, rheumatoid drugs, malignancy 1/3 resolve, 1/3 respond to cytotoxics, 1/3 develop chronic kidney disease |
|
|
IgA nephropathy - aka Berger's disease, mesangioproliferative GN |
typically young adult with haematuria following an URTI |
|
|
Diffuse proliferative glomerulonephritis DPG - the dog pound are strep. (strepped) with infxn |
classical post-streptococcal glomerulonephritis in child presents as nephritic syndrome / acute kidney injury most common form of renal disease in SLE |
|
|
Minimal change disease |
most common cause of GN in children typically a child with nephrotic syndrome (accounts for 80%) causes: Hodgkin's, NSAIDs good response to steroids |
|
|
Focal segmental glomerulosclerosis |
may be idiopathic or secondary to HIV, heroin presentation: proteinuria / nephrotic syndrome / chronic kidney disease |
|
|
Rapidly progressive glomerulonephritis - aka crescentic glomerulonephritis |
rapid onset, often presenting as acute kidney injury causes include Goodpasture's, ANCA positive vasculitis |
|
|
Mesangiocapillary glomerulonephritis (membranoproliferative GN) |
type 1: cryoglobulinaemia, hepatitis C type 2: partial lipodystrophy |
|
|
In hand, foot and mouth disease oral lesion usually occur before palm and sole lesions true/false |
true |
|
|
hand, foot and mouth disease |
May be caused by enterovirus 71 Typically occurs in outbreaks
Children do not need to be excluded from school Mild systemic upset is common |
|
|
Which one of the following drugs is contra-indicated whilst breast feeding? |
lithium |
|
|
The following drugs can be given to mothers who are breast feeding: |
antibiotics: penicillins, cephalosporins, trimethoprim endocrine: glucocorticoids (avoid high doses), levothyroxine* epilepsy: sodium valproate, carbamazepine asthma: salbutamol, theophyllines psychiatric drugs: tricyclic antidepressants, antipsychotics** hypertension: beta-blockers, hydralazine, methyldopa anticoagulants: warfarin, heparin digoxin |
|
|
The following drugs should be avoided in pregnancy: |
antibiotics: ciprofloxacin, tetracycline, chloramphenicol, sulphonamides psychiatric drugs: lithium, benzodiazepines aspirin carbimazole sulphonylureas cytotoxic drugs amiodarone |
|
|
A 5-year-old boy is diagnosed as having absence seizures. What is the chance he will be seizure free by the age of 16-years-old? |
Absence seizures - good prognosis: 90-95% become seizure free in adolescence |
|
|
Cleft lip and palate |
affect around 1 in every 1,000 babies pathophys: polygenic inheritance maternal antiepileptic use increases risk cleft lip results from failure of the fronto-nasal and maxillary processes to fuse cleft palate results from failure of the palatine processes and the nasal septum to fuse Problems feeding: orthodontic devices may be helpful speech: with speech therapy 75% of children develop normal speech increased risk of otitis media for cleft palate babies |
|
|
Cleft lip and palate mgmt |
cleft lip is repaired earlier than cleft palate, with practices varying from repair in the first week of life to three months cleft palates are typically repaired between 6-12 months of age |
|
|
Live attenuated vaccines MOOBY (is LIVE) CI to live vaccines = preg and immunosuppresion |
MMR Oral polio Oral typhoid BCG Yellow fever |
|
|
Inactivated vaccines (RIFLE) |
Rabies InFLuEnza (intramuscular) |
|
|
Detoxified exotoxins vaccines |
tetanus |
|
|
Extracts of the organism/virus (sometimes termed fragment vaccine) DPHM |
diphtheria pertussis ('acellular' vaccine) hepatitis B meningococcus, pneumococcus, haemophilus |
|
|
Not contraindications to immunisation |
asthma or eczema history of seizures (if associated with fever then advice should be given regarding antipyretics) breastfed child previous history of natural pertussis, measles, mumps or rubella infection history of neonatal jaundice family history of autism neurological conditions such as Down's or cerebral palsy low birth weight or prematurity patients on replacement steroids e.g. (CAH) |
|
|
mid parental height calculation FOR BOYS (ie make mums height similar height to dad) |
For boys (both give same answer): [DADS height cm + (MUMS height cm + 5 inches or 13 cm)] / 2 OR ((DADs height cm + MUMS height cm)/2) + 7 |
|
|
mid parental height calculation FOR GIRLS (ie make dads height similar to mums) |
For girls(both give same answer): [MUMs height cm + (DADs height cm – 5 inches or 13 cm)] / 2 OR ((DADs height cm + MUMS height cm)/2) - 7 |
|
|
The most common causes of hearing problems in children are listed below |
Conductive HL secretory otitis media Down's syndrome (+/- snhl) Sensorineural HL hereditary - Usher syndrome, Pendred syndrome, Jervell-Lange-Nielson syndrome, Wardenburg syndrome congenital infection e.g. rubella acquired - meningitis, head injury cerebral palsy perinatal insult |
|
|
A 3-year-old girl is taken to the GP due to a rash on her upper arm. On examination multiple raised lesions of about 2 mm in diameter are seen. On close inspection a central dimple is present in the majority of lesions. What is the likely diagnosis? |
Molluscum contagiosum (is a virus) |
|
|
At what age do the majority of children achieve day and night time urinary continence? |
3-4yo |
|
|
A 23-year-old female with Down's syndrome is reviewed in clinic. Which one of the following features is least associated with her condition? |
infertility As this patient is female she is likely to be subfertile rather than infertile |
|
|
Down syndrome: features |
face: upslanting palpebral fissures, epicanthic folds, Brushfield spots in iris, protruding tongue, small ears, round/flat face flat occiput single palmar crease, pronounced 'sandal gap' between big and first toe hypotonia congenital heart defects (40-50%, see below) duodenal atresia Hirschsprung's disease |
|
|
Cardiac complications of DS |
multiple cardiac problems may be present endocardial cushion defect (c. 40%, also known as atrioventricular septal canal defects) ventricular septal defect (c. 30%) secundum atrial septal defect (c. 10%) tetralogy of Fallot (c. 5%) isolated patent ductus arteriosus (c. 5%) |
|
|
Later complications of DS |
subfertility: males are almost always infertile due to impaired spermatogenesis. Females are usually subfertile, and have an increased incidence of problems with pregnancy and labour learning difficulties short stature repeated respiratory infections (+hearing impairment from glue ear) acute lymphoblastic leukaemia hypothyroidism Alzheimer's atlantoaxial instability |
|
|
Talk in short sentences (e.g. 3-5 words) |
3 years |
|
|
Vocabulary of 2-6 words |
12-15 months |
|
|
Responds to their own name |
12-15 months |
|
|
Cause of obesity in children |
growth hormone deficiency hypothyroidism Down's syndrome Cushing's syndrome Prader-Willi syndrome |
|
|
Acne is actually more common in females after the age of 25 years |
true |
|
|
pathophys of acne vulgaris |
follicular epidermal hyperproliferation resulting in the formation of a keratin plug. This in turn causes obstruction of the pilosebaceous follicle. Activity of sebaceous glands may be controlled by androgen, although levels are often normal in patients with acne colonisation by the anaerobic bacterium Propionibacterium acnes inflammation |
|
|
A mother brings her 9-month-old child to surgery. She is concerned he is not developing normally and is 'falling behind' the children of her friends. Whilst observing the child you notice he sits without support but makes little effort to move around the room. He has a crude pincer grip, appears shy when you try to interact and says 'mama' but little else. What is the most accurate description of his development? |
normal d/t |
|
|
A mother brings her 18-month-old daughter for review following a recent admission after a febrile convulsion. Which one of the following statements regarding febrile convulsions is not correct? |
Giving antipyretics promptly can reduce the chance of further seizures Antipyretics do not prevent febrile convulsions |
|
|
Which one of the following drugs is contra-indicated whilst breast feeding? |
Lymecycline |
|
|
The parents of a 3-year-old boy with cystic fibrosis ask for advice. They are considering having more children. What is the chance that their next child will be a carrier of the cystic fibrosis gene? |
50% As cystic fibrosis is an autosomal recessive condition there is a 50% chance that their next child will be a carrier of cystic fibrosis (i.e. be heterozygous for the genetic defect) and a 25% chance that the child will actually have the disease (be homozygous). |
|
|
Organisms which may colonise CF patients |
Staphylococcus aureus Pseudomonas aeruginosa Burkholderia cepacia* Aspergillus |
|
|
Which one of the following best describes the emergency treatment of a child with severe croup? |
Oxygen + nebulised adrenaline Oral dexamethasone should also be given if the child is able to take it. |
|
|
What is the average age that the first signs of puberty appear in girls? |
11.5 years |
|
|
Normal changes in puberty |
gynaecomastia may develop in boysasymmetrical breast growth may occur in girlsdiffuse enlargement of the thyroid gland may be seen |
|
|
Malesfirst sign is testicular growth at around 12 years of age (range = 10-15 years) |
true |
|
|
Femalesfirst sign is breast development at around 11.5 years of age (range = 9-13 years) |
true |
|
|
male puberty |
first sign is testicular growth at around 12 years of age (range = 10-15 years) testicular volume > 4 ml indicates onset of puberty maximum height spurt at 14 |
|
|
female puberty |
first sign is breast development at around 11.5 years of age (range = 9-13 years) height spurt reaches its maximum early in puberty (at 12) , before menarche menarche at 13 (11-15) there is an increase of only about 4% of height following menarche |
|
|
A 15-year-old girl presents with a palpable purpuric rash over her lower limbs accompanied by polyarthralgia following a recent sore throat. What is the most likely diagnosis? |
Henoch-Schonlein purpura Henoch-Schonlein purpura (HSP) is an IgA mediated small vessel vasculitis. There is a degree of overlap with IgA nephropathy (Berger's disease). HSP is usually seen in children following an infection. |
|
|
Henoch-Schonlein purpura fxs |
palpable purpuric rash (with localized oedema) over buttocks and extensor surfaces of arms and legs abdominal pain polyarthritis features of IgA nephropathy may occur e.g. haematuria, renal failure |
|
|
tx for Henoch-Schonlein purpura |
analgesia for arthralgia treatment of nephropathy is generally supportive. There is inconsistent evidence for the use of steroids and immunosuppressants |
|
|
prognosis ofHenoch-Schonlein purpura |
usually excellent, HSP is a self-limiting condition, especially in children without renal involvement around 1/3rd of patients have a relapse |
|

dx |
Henoch-Schonlein purpura |
|

dx |
Henoch-Schonlein purpura |
|

dx |
Henoch-Schonlein purpura |
|
|
A 4-week-old baby girl is diagnosed as having developmental dysplasia of the left hip following an ultrasound examination. Clinical examination of the hip was abnormal at birth. What treatment is she most likely to be given? |
Pavlik harness |
|
|
At what age would the average child start to say 'mama' and 'dada'? |
9-10 months |
|
|
The table below summarises the major speech and hearing developmental milestones |
3 months Quietens to parents voice Turns towards sound Squeals 6 months Double syllables 'adah', 'erleh' 9 months Says 'mama' and 'dada' Understands 'no' 12 months Knows and responds to own name 12-15 months Knows about 2-6 words (Refer at 18 months) Understands simple commands - 'give it to mummy' 2 years Combine two words Points to parts of the body 2½ years Vocabulary of 200 words 3 years Talks in short sentences (e.g. 3-5 words) Asks 'what' and 'who' questions Identifies colours Counts to 10 (little appreciation of numbers though) 4 years Asks 'why', 'when' and 'how' questions |
|
|
The chance of a 40-year-old mother giving birth to a child with Down's syndrome is approximately: |
1 in 100 |
|
|
A mother asks for information following a recent admission of her 2-year-old son with a febrile convulsion. What is the chance of her son having a further febrile convulsion? |
30% |
|
|
Which one of the following statements regarding Reye's syndrome is incorrect? |
Plasma exchange should be started as soon as possible |
|
|
Reye's syndrome |
Management of Reye's sydnrome is largely supportive. mortality rate of 15-25%. |
|
|
Reye's syndrome def |
severe, progressive encephalopathy affecting children that is accompanied by fatty infiltration of the liver, kidneys and pancreas |
|
|
Reye's syndrome fxs |
The peak incidence is 2 years of age, features include: may be history of preceding viral illness encephalopathy: confusion, seizures, cerebral oedema, coma fatty infiltration of the liver, kidneys and pancreas hypoglycaemia |
|

An 11-year-old girl presents with a productive cough and fever. A chest x-ray is taken: main finding on the XR? |
Left lingual consolidation |
|

A 10-year-old girl is admitted with shortness-of-breath and fatigue. A chest x-ray is performed on admission: Based on the x-ray findings, what is the most likely diagnosis? |
heart failure The x-ray shows dilated cardiomyopathy and features of pulmonary oedema including fluid in the horizontal fissure. |
|
|
Which one of the following is least likely to cause snoring in children? |
Kallman's syndrome Kallman's syndrome is a cause of delayed puberty secondary to hypogonadotrophic hypogonadism. It is not associated with snoring |
|
|
Snoring in children Causes |
obesity nasal problems: polyps, deviated septum, hypertrophic nasal turbinates recurrent tonsillitis Down's syndrome hypothyroidism |
|
|
Roseola - school exclusion? |
no |
|
|
whooping cough - |
5 days from commencing antibiotics should go back to school |
|
|
diarrhoea and vomitting |
go back to school when sxs have settled for 48hrs |
|
|
For which one of the following indications is carbamazepine least likely to be a useful management option? |
absent seizures Carbamazepine is generally ineffective in absence seizures |
|
|
Carbamazepine |
chemical structure similar to TCAS 1st line for partial seizures other indications: neuropathic pain (trigeminal neuralgia, diabetic neuropathy) bipolar disorder moa Na channel blocker = DOWN excitabiity Adverse effects P450 enzyme inducer dizziness and ataxia drowsiness headache visual disturbances (especially diplopia) Steven-Johnson syndrome leucopenia and agranulocytosis syndrome of inappropriate ADH secretion |
|
|
Which one of the following drugs is contra-indicated whilst breast feeding? |
Amiodarone |
|
|
A 9-year-old boy who has recently arrived from India presents with fever. On examination a grey coating is seen surrounding the tonsils and there is extensive cervical lymphadenopathy. What is the most likely diagnosis? |
Diphtheria caused by the Gram positive bacterium Corynebacterium diphtheriae |
|
|
Diphtheria pathophys |
releases an exotoxin encoded by a β-prophage exotoxin inhibits protein synthesis by catalyzing ADP-ribosylation of elongation factor EF-2 Diphtheria toxin commonly causes a 'diphtheric membrane' on tonsils caused by necrotic mucosal cells. Systemic distribution may produce necrosis of myocardial, neural and renal tissue |
|
|
diptheria possible presentations |
recent visitors to Eastern Europe/Russia/Asia sore throat with a 'diphtheric membrane' - see above bulky cervical lymphadenopathy neuritis e.g. cranial nerves heart block |
|
|
A 2-year-old boy presents with a harsh cough and pyrexia. His symptoms worsened overnight and on examination stridor is noted. Which one of the following interventions may improve his symptoms? |
Oral dexamethasone px has CROUP Croup is a form of upper respiratory tract infection seen in infants and toddlers. It is characterised by stridor which is caused by a combination of laryngeal oedema and secretions. Parainfluenza viruses account for the majority of cases. |
|
|
croup is mostly caused by |
parainfluenza virus fxs stridor barking cough (worse at night) fever coryzal symptoms |
|
|
Hypospadias is a |
congenital abnormality of the penis which occurs in approximately 3/1,000 male infants |
|
|
Hypospadias is characterised by |
a ventral urethral meatus a hooded prepuce chordee (ventral curvature of the penis) in more severe forms tx Corrective surgery is performed before 2 years of age. It is essential that the child is not circumcised prior to the surgery as the foreskin may be used in the corrective procedure |
|
|
Which one of the following statements concerning hypospadias is incorrect? |
Dorsal curvature of the penis is seen in more severe forms IT SHOULD VENTRAL CURVATURE |
|
|
A 4-year-old boy is brought in to surgery by his mother. He has reportedly been drowsy and pyrexial for the past 2 hours. Whilst waiting to be seen he becomes unresponsive. One of your GP colleagues performs an urgent assessment whilst the practice nurse calls 999. He is making no respiratory effort so 5 rescue breaths are given. As you arrive your colleague cannot detect a brachial or carotid pulse. What is the most appropriate course of action? |
Start chest compressions/ventilations at a ratio of 15:2 |
|
|
Paediatric basic life support STEPS |
unresponsive? shout for help open airway look, listen, feel for breathing give 5 rescue breaths check for signs of circulation 15 chest compressions:2 rescue breaths |
|
|
DEFINE meconium ileus |
Meconium ileus is a bowel obstruction that occurs when the meconiumin your child's intestine is even thicker and stickier than normalmeconium, creating a blockage in a part of the small intestine called theileum. Most infants with meconium ileus have a disease called cystic fibrosis. |
|
|
A newborn female baby is diagnosed with cystic fibrosis following an episode of meconium ileus shortly after birth. Which one of the following is least likely to occur as a consequence of her underlying diagnosis? |
Arthropathy is not a common feature of cystic fibrosis |
|
|
Cystic fibrosis: features |
Delayed puberty Nasal polyps Diabetes mellitus Rectal prolapse |
|
|
CF presenting fxs |
neonatal period (around 20%): meconium ileus, less commonly prolonged jaundice recurrent chest infections (40%) malabsorption (30%): steatorrhoea, failure to thrive other features (10%): liver disease |
|
|
Other features of cystic fibrosis |
short stature diabetes mellitus delayed puberty rectal prolapse (due to bulky stools) nasal polyps male infertility, female subfertility |
|
|
CF effects on fertility for male and female |
male = infertility female = subfertility |
|
|
At what age would the average child acquire the ability to build a tower of three blocks? |
18 months |
|
|
Which one of the following features is associated with rickets? |
Genu varum (bow legs) Genu valgum (knock knees) Reduced serum calcium
Harrison's sulcus |
|
|
rickets fxs |
in toddlers - genu varum (bow legs), in older children - genu valgum (knock knees) 'rickety rosary' - swelling at the costochondral junction kyphoscoliosis craniotabes - soft skull bones in early life Harrison's sulcus reduced serum calcium - symptoms may results from hypocalcaemiaraised alkaline phosphatase |
|
|
mgmt of rickets |
oral vitamin D |
|
|
predisposing factors to rickets |
mainly vitamin D deficiency dietary deficiency of calcium, for example in developing countries prolonged breast feedingun supplemented cow's milk formula lack of sunlight |
|

A 12-year-old girl presents with a two-day history of an itchy rash over her whole body associated with a low-grade pyrexia: Which one of the following complications is least likely to occur? |
Dilated cardiomyopathy px has chickenpox |
|
|
A 12-year-old girl presents with a two-day history of an itchy rash over her whole body associated with a low-grade pyrexia: what are some complications |
Disseminated haemorrhagic chickenpox Secondary bacterial infection Encephalitis
Pneumonia |
|
|
Chickenpox is highly infectious |
spread via the respiratory route can be caught from someone with shingles infectivity = 4 days before rash, until 5 days after the rash first appeared* incubation period = 10-21 days |
|
|
chicken pox vs shingles |
Chickenpox is caused by primary infection with varicella zoster virus. Shingles is reactivation of dormant virus in dorsal root ganglion |
|
|
mgmt of chicken pox |
supportive - keep cool, trim nails - calamine lotion - school exclusion - if immunocompromised px = give IVIG of VZ |
|
|
A COMMON COMPLICATION OF CHICKENPOX is |
secondary bacterial infection of the lesions. Rare complications include: pneumonia encephalitis (cerebellar involvement may be seen) disseminated haemorrhagic chickenpox arthritis, nephritis and pancreatitis may very rarely be seen |
|
|
A mother brings her 3-year-old boy who is known to have Down's syndrome to surgery, as she is concerned about his vision. Which one of the following eye problems is least associated with Down's syndrome? |
Retinal detachment |
|
|
Down's syndrome: vision and hearing problems |
Vision refractive errors are more common strabismus: seen in around 20-40% cataracts: congenital and acquired are both more common recurrent blepharitis glaucoma Hearing otitis media and glue ear are very common resulting in hearing problems |
|
|
At what age would the average child acquire the ability to sit without support? |
7-8 months |
|
|
Which one of the following statements regarding the MMR vaccine is incorrect? |
Children who received another live vaccine 2 weeks ago can safely have MMR |
|
|
Contraindications to MMR |
severe immunosuppression allergy to neomycin children who have received another live vaccine by injection within 4 weeks pregnancy should be avoided for at least 1 month following vaccination immunoglobulin therapy within the past 3 months (there may be no immune response to the measles vaccine if antibodies are present) |
|
|
Adverse effects of MMR |
malaise, fever and rash may occur after the first dose of MMR. This typically occurs after 5-10 days and lasts around 2-3 days |
|
|
usmle embryo |
usmle embryo |
|
|
A 3-year-old girl is brought in for an evaluation after she has been having recurrent infection. Further evaluation shows failure to thrive, delayed speech development, low-set ears and poor muscle tone. Genetic analysis shows 22q11 deletion. Which embryonic abnormalities are most likely responsible for these clinical manifestations? |
Abnormal development of the 3rd and 4th branchial pouches |
|
|
DiGeorge syndrome FXS |
Salient features can be summarized using the mnemonic CATCH-22 to describe DiGeorge syndrome, with the 22 to remind one the chromosomal abnormality is found on the 22 chromosome Cardiac abnormality (especially tetralogy of Fallot) Abnormal facies Thymic aplasia Cleft palate Hypocalcemia/Hypoparathyroidism 22 CHROMOSOME |
|
|
BRACHIAL CLEFTS MNEMONIC |
1st Arch: a Massive list of M’s Nerve: Maxillary and Mandibular nerves Artery: Maxillary artery Cartilage: Meckel’s Cartilage - Mandible + spheno Mandibular ligament - Malleus + Incus Muscles: MAT x 2- Muscles of Mastication - Mylohyoid - Anterior belly of digastric- Anterior 2/3 of tongue- Tensor veli palatini- Tensor tympaniPS: for every one you get right reward yourself with an M&M :D2nd arch: SecondNerve: Seventh nerve (facial nerve)Artery: Stapedial artery and hyoid arteryCartilage: - Stapes- Styloid- Stylohyoid ligament- leSSer horn of hyoidMuscles: - Muscles of facial expression (Smiling)- Stapedius- Stylohyoid- poSSSterior belly of digastric3rd arch: think Glossopharyngeal nerveNerve: - Glossopharyngeal nerveCartilage: - Greater horn of hyoidMuscle: - Stylopharyngeus4th Arch: Swallowing + The exceptions to the 6th arch belowNerve: Superior Laryngeal (branch of vagus) Cartilage: - Thyroid cartilageMuscles: - Pharyngeal constrictors- Levator veli palatini- Cricothyroid6th Arch: Speaking (Laryngeal)Nerve: Recurrent laryngeal (branch of vagus)Cartilage: All laryngeal cartilages except thyroid cartilageMuscles: All instrinsic laryngeal muscles except cricothyroid |
|
|
A 28-year-old, G2P1 woman gives birth to a female neonate with no obvious abnormalities. The infant's temperature is 36.8ºC (98.2ºF), heart rate is 155 beats/minute, respiratory rate is 50 breaths/minute, and 1 and 5 minute Apgar scores are 7 and 8, respectively. The infant has a strong cry and appears pink. A cardiac murmur is heard, which is available as an Exhibit (button at bottom of screen). The remainder of the exam is normal.
Giving what will get rid of the murmur |
Indomethicin
PG keeps ductus arteriosus open, indo. Is a nsaid, which blocks cox thus reduce PG = help close patent ductus arteriosus |
|
|
A 3-year-old child is brought to surgery as her mother has noticed that she is 'cross-eyed'. The corneal light reflection test confirms this. What is the most appropriate management? |
Refer children with a squint immediately to ophthalmology |
|
|
squint aka |
strabismus characterised bymisalignment of the visual axes. Squints may be divided into: 1) concomitant (common) and 2) paralytic (rare) 1) concomitant = - Due to imbalance in extraocular muscles - Convergent is more common than divergent 2) paralytic = - due to paralysis of extraocular muscles |
|
|
how do you detect a squint |
by the corneal light reflection test - holding a light source 30cm from the child's face to see if the light reflects symmetrically on the pupils |
|
|
mgmt of strabismus aka squint |
eye patches may help prevent amblyopia referral to secondary care is appropriate nb amblyopia = impaired or dim vision without obvious defect or change in the eye |
|
|
A 2-year-old child with a history of atopic eczema is brought to the local GP surgery. Her eczema is usually well controlled with emollients but her parents are concerned as the facial eczema has got significantly worse overnight. She now has painful clustered blisters on both cheeks, around her mouth on her neck. Her temperature is 37.9ºC. What is the most appropriate management? |
Eczema herpeticum is a serious condition that requires IV antivirals |
|
|
Eczema herpeticum describes |
a severe primary infection of the skin by herpes simplex virus 1 or 2. It is more commonly seen in children with atopic eczema. As it is potentially life threatening children should be admitted for IV aciclovir |
|
|
A boy is noted to have a webbed neck and pectus excavatum |
Noonan sydrome nb Turners and Noonan both have webbed neck (short neck) |
|
|
An infant is found to have small eyes and polydactyly |
Patau syndrome |
|
|
A 7-year-old boy with learning difficulties and macrocephaly |
Fragile X |
|
|
What is the most useful investigation to screen for the complications of Kawasaki disease? |
Echocardiogram NOT coronary angiogram |
|
|
Precocious puberty in females may be defined as the development of secondary sexual characteristics before: |
8 years of age for females (males before 9yo) |
|
|
Which one of the following vaccinations should be avoided in patients who are HIV positive? |
BCG NB MO(p)O(t)BY try MOOBY smoking POT LIVE |
|
|
Hops on one leg |
4 years |
|
|
Pulls to standing |
8-10 months |
|
|
Squats to pick up ball |
18 months |
|
|
Management if suspected meningococcal septicaemia |
give intramuscular or intravenous benzylpenicillin unless there is a history of anaphylaxis and admit |
|
|
specific signs for meningococcal septicaemia |
remember that sxs of meningitis will be non specific more specific sxs/signs: Non-blanching rash, altered mental state, capillary refill time more than 2 seconds, unusual skin colour, shock, hypotension, leg pain, cold hands/feet |
|
|
What is the most common presenting feature of Wilms tumour? |
Abdominal mass |
|
|
Wilms tumor |
Wilms' nephroblastoma is one of the most common childhood malignancies usu. LT 5yo |
|
|
fxs of wilms tumor |
abdominal mass (most common presenting feature) painless haematuria flank pain other features: anorexia, feverunilateral in 95% of cases metastases are found in 20% of patients (most commonly lung) |
|
|
wilms tumor mgmt |
nephrectomy chemotherapy radiotherapy if advanced disease prognosis: good, 80% cure rate |
|
|
Which one of the following is least recognised as a side-effect of carbamazepine? |
Hirsutism |
|
|
Which one of the following statements regarding the vaccine used to routinely immunise children against influenza is correct? |
It is a live vaccine (MOOBYI/MOOIBY) |
|
|
A new NHS influenza vaccination programme for children was announced in 2013. There are three key things to remember about the children's vaccine: |
it is given intranasally the first dose is given at 2-3 years, then annually after that it is a live vaccine (cf. injectable vaccine below) |
|
|
Mnemonics: Horner's Syndrome PAMELa (anderson) shes horny ie horners |
Ptosis Anhydrosis Miosis Enophthalmos Loss of ciliospinary reflex |
|
|
Mnemonics: MODIFIED JONES CRITERIA Rheumatic Fever - MAJOR CRITERIA |
MAJOR CRITERIA - JONES/CASES C- Carditis A- Arthritis (not Arthralgias i.e polyarthritis) S- Syndhem's Chorea E- Erythema Marginatum (not nodosum) S- Subcutaneous Nodules |
|
|
Mnemonics: MODIFIED JONES CRITERIA Rheumatic Fever - MINOR CRITERIA |
"PEACH-Fever" P- Prolonged PR interval E- ESR raised A- Arthralgias (not arthritis), Acute phase reactants : leukocytosis, elevated sedimentation rate, and C -reactive protein C- C-reactive protein increased H- History of previous rheumatic fever, rheumatic heart disease & Fever |
|
|
AD & AR disorders |
Autosomal recessive conditions are 'metabolic' - exceptions: inherited ataxias Autosomal dominant conditions are 'structural' - exceptions: Gilbert's, hyperlipidaemia type II |
|
|
The following conditions are autosomal dominant: |
Achondroplasia Acute intermittent porphyria Adult polycystic disease Antithrombin III deficiency Ehlers-Danlos syndrome Familial adenomatous polyposis Hereditary haemorrhagic telangiectasia Hereditary spherocytosis Hereditary non-polyposis colorectal carcinoma Huntington's disease Hyperlipidaemia type II Hypokalaemic periodic paralysis Malignant hyperthermia Marfan's syndromes Myotonic dystrophy Neurofibromatosis Noonan syndrome Osteogenesis imperfecta Peutz-Jeghers syndrome Retinoblastoma Romano-Ward syndrome Tuberose sclerosis Von Hippel-Lindau syndrome Von Willebrand's disease (type 1 and 2 but 3 is AR) |
|
|
A 14-year-old male being investigated for iron-deficiency anaemia is found to have numerous polyps in his jejunum. On examination he is also noted to have pigmented lesions on his palms and soles. What is the likely diagnosis? |
Peutz-Jeghers syndrome |
|
|
Peutz-Jeghers syndrome |
autosomal dominant condition characterised by numerous hamartomatous polyps in the gastrointestinal tracT also associated with pigmented freckles on the lips, face, palms and soles. Around 50% of patients will have died from a gastrointestinal tract cancer by the age of 60 years |
|
|
Peutz-Jeghers syndrome FXS |
hamartomatous polyps in GI tract (mainly small bowel) pigmented lesions on lips, oral mucosa, face, palms and soles intestinal obstruction e.g. intussusception gastrointestinal bleeding |
|
|
Peutz-Jeghers syndrome MGMT |
conservative unless complications develop |
|
|
Short stature may be caused by: |
normal variant (often familial) constitutional delay of growth and puberty chronic illness e.g. cystic fibrosis, inflammatory bowel disease endocrine: growth hormone deficiency , hypothyroidism, steroid excess syndromes: Turner's, Down's, Prader-Willi skeletal dysplasias e.g. achondroplasia |
|
|
achondroplasia |
genetic disorder in bone d/t in the arms and legs - affects more the proximal arm and leg causing short stature, hypotonia, can be cervical/lumbar stenosis head and thus learning normal because bone d/t in skull different from those in the extremities mgmt -GH -surgical lengthening of lower extremities |
|
|
The Newborn Metabolic Screening Programme screens newborn babies for 28 metabolic disorders in NZ: |
amino acid disorders (14 disorders, including PKU and MSUD) fatty acid oxidation disorders (9 disorders e.g. MCAD) others: - Congenital hypothyroidism (CH) - Cystic fibrosis (CF) - Congenital adrenal hyperplasia (CAH) - Galactosaemia - Biotinidase deficiency. |
|
|
Which one of the following neonatal complications is least commonly seen in diabetic pregnancies? |
Microsomia Diabetes predisposes to macrosomia rather than microsomia |
|
|
Pregnancy: diabetes - complications 2 TYPES 1) maternal complications 2) neonatal complications |
maternal complications: polyhydramnios (25%) preterm labour (15%) |
|
|
Pregnancy: diabetes - complications 2 TYPES 1) maternal complications 2) neonatal complications |
macrosomia (although diabetes may also cause small for gestational age babies) hypoglycaemia (secondary to beta cell hyperplasia) respiratory distress syndrome: surfactant production is delayed polycythaemia: therefore more neonatal jaundice malformation rates increase 3-4 fold e.g. sacral agenesis, CNS and CVS malformations (hypertrophic cardiomyopathy) stillbirth hypomagnesaemia hypocalcaemia shoulder dystocia (may cause Erb's palsy) |
|
|
A 14-month-old girl is diagnosed as having roseola infantum. What is the most common complication of this disease? |
Febrile convulsions in 10-15% roseola infantum aka exanthem subitum OR 6th disease because its caused by HERPES 6 starts out as fever, then that goes and then you get rash and then febrile convulsions |
|
|
Which one of the following is least associated with constipation in children? |
Addison's disease |
|
|
You are doing the six week check on a baby girl. Which one of the following best describes the Barlow test for developmental dysplasia of the hip? |
Attempts to dislocate an articulated femoral head |
|
|
Barlow and ortalani test |
barlow test to dislocated articulated femoral head - hip and knee flexed at 90o and then adducting hips, and then apply pressure on the knee to push f. head backwards = f. head pushed out, and you can palpate the dislocated head ortalani test to relocated it (ie dislocated femoral head) used to confirm findings of B. test, to see if hip actually dislocated, by relocating it, hip and knee flexed at 90o, then abdxn of hip and push the thigh forward/anteriorly to relocate f. head, +ve test if a palable audible clunk heard when hip is reduced (ie put back into the socket) B comes before O Barlow = time to go OUT to the BAR ie femoral head out of socket Ortolani = we need to go back home ie put femoral head back into the socket |
|
|
Barlow and ortolani test |
B test - hip started out as reduced (ie in its socket) - test will dislocate hip ortolani test - hip started out dislocated - test will reduce the hip both tests are used for screening in newborns |
|
|
DDH is examined using |
barlow and ortalani test US confirms dx |
|
|
ddx risk factors |
female sex: 6 times greater risk breech presentation positive family history firstborn children oligohydramnios birth weight > 5 kg congenital calcaneovalgus foot deformity |
|
|
ddh mgmt |
most spontaneous stabilise by 3-6 weeks of age pavlik harness in children younger than 4-5 months older kids may req. surg. |
|
|
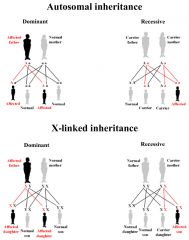
autosomal inheritance |
Inheriting a disease, condition, or trait depends on the type of chromosome affected (autosomal or sex chromosome). It also depends on whether the trait is dominant or recessive. A single abnormal gene on one of the first 22 nonsex (autosomal) chromosomes from either parent can cause an autosomal disorder. |
|
|
autosomal inheritance |
|
|
|
A 30-year-old woman presents for the 6 week check of her son who was diagnosed with Down's syndrome shortly after birth. A letter from genetics has confirmed non-disjunction as the cause of the trisomy. She asks you about future pregnancies. What is the chance that her next child will also have Down's syndrome? |
1 in 100 |
|
|
Which one of the following drugs is not contra-indicated whilst breast feeding? |
Ceftriaxone |
|
|
You are asked to by the Primary Care Trust to design a program to improve the health of infants in the local community. What is the most common cause of death of infants greater than one month but less than one year old? |
Sudden infant death syndrome |
|
|
A 12-year-old female from Bulgaria presents to the surgery. She reports being unwell for the past 2 weeks. Initially she had a sore throat but she is now experiencing joint pains intermittently in her knees, hips and ankles. On examination there are some pink, ring shaped lesions on the trunk and occasional jerking movements of the face and hands. What is the most likely diagnosis? |
Rheumatic fever |
|
|
measles made easy remember its an RNA virus |
4 D's and 4 C's 4 D's = 4 day fevers 4 C's = cough, coryza, conjunctivitis, coplik spots nb its actually Koplik spots but who cares (its pathognomonic (diagnostic) for measles - this is not the generalised red (maculopapular) measles rash |
|
|
pathognomonic def |
diagnostic |
|
|
Which one of the following is least recognised as a complication of measles infection? |
infertility these ones are complications of measles infxn: Keratoconjunctivitis Encephalitis Subacute sclerosing panencephalitis Pneumonia |
|
|
measles prodrome |
irritable, conjunctivitis, fever |
|
|
measles: koplik spots |
K. spots (occurs before the generalised rash) - white spots ('grain of salt') on buccal mucosa Generalised rash - starts behind ears then to whole body, discrete maculopapular rash becoming blotchy & confluent |
|
|
measles complications |
encephalitis: typically occurs 1-2 weeks following the onset of the illness) subacute sclerosing panencephalitis: very rare, may present 5-10 years following the illness febrile convulsions giant cell pneumonia keratoconjunctivitis, corneal ulceration diarrhoea increased incidence of appendicitis myocarditis |
|
|
mgmt of unimmunised kid who gets measles |
give MMR vaccine within 72hrs |
|
|
You are reviewing a 9-month-old child with suspected bronchiolitis. Which one of the following features should make you consider other possible diagnoses? |
high fever bronchiolitis is usu. has low grade fever |
|
|
A newborn baby is noted to have low-set ears, rocker bottom feet and overlapping of her fingers. What is the most likely diagnosis? |
Edward's syndrome |
|
|
fragile X syndrome |
X men are dumb and very emotional night crawler has low set ears, rocker bottom feet and overlapping fingers |
|
|
An 8-year-old boy who is known to have asthma is reviewed. His current treatment is a salbutamol inhaler as required and beclometasone inhaler 200mcg bd. Despite this he regular requires salbutamol for exacerbations and suffers with a night time cough. What is the most appropriate next step in management? |
Trial of a long-acting beta2-agonist |
|
|
Which one of the following congenital infections is most characteristically associated with sensorineural deafness? |
rubella Congenital rubella sensorineural deafness congenital cataracts |
|
|
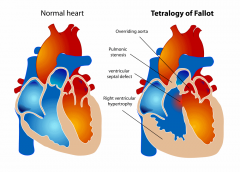
tetrology of fallot |
|
|
|
Which one of the following is not associated with the development of obesity in children? |
male sex |
|
|
What is the most common cause of hypertension in children? |
2o HTN due to Renal parenchymal disease (80%) |
|
|
You are asked to teach a 14-year-old boy how to use his metered dose salbutamol inhaler. After removing the cap and shaking, what is the next step? |
Breathe out gently |
|
|
Inhaler technique for MDI |
1. Remove cap and shake 2. Breathe out gently 3. Put mouthpiece in mouth and as you begin to breathe in, which should be slow and deep, press canister down and continue to inhale steadily and deeply 4. Hold breath for 10 seconds, or as long as is comfortable 5. For a second dose wait for approximately 30 seconds before repeating steps 1-4. Only use the device for the number of doses on the label, then start a new inhaler. |
|
|
Which one of the following is a cause of cyanotic congenital heart disease? |
Transposition of the great arteries |
|
|
Congenital heart disease: 2 types |
Acyanotic and Cyanotic |
|
|
Congenital heart disease most common causes of acyanotic heart disease |
ventricular septal defects (VSD) - most common, accounts for 30% atrial septal defect (ASD) patent ductus arteriosus (PDA) coarctation of the aortaaortic valve stenosis |
|
|
Congenital heart disease Cyanotic - most common causes |
tetralogy of Fallot transposition of the great arteries (TGA) tricuspid atresia pulmonary valve stenosis |
|
|
Bronchiolitis: investigations |
Look for RSV can be done rapidly using a fluorescent antibody test on nasopharyngeal secretions |
|
|
Bronchiolitis is a condition characterised by |
acute bronchiolar inflammation. Respiratory syncytial virus (RSV) is the pathogen in 75-80% of cases |
|
|
Bronchiolitis: management |
is supportive: 02 fluids + feed NG/IV +/- ventilation if due to bact. infxn = tx |
|
|
Admission criteria for bronchiolitis |
feeding difficulties RR > 50/min episodes of apnoea |
|
|
What is the investigation of choice to look for renal scarring in a child with vesicoureteric reflux? |
DMSA nb VUR is normally diagnosed following a micturating cystourethrograma DMSA scan may also be performed to look for renal scarring |
|
|
Which one of the following congenital infections is most characteristically associated with chorioretinitis? |
Toxoplasma gondii Congenital toxoplasmosis cerebral calcification chorioretinitis |
|
|
Benign rolandic epilepsy or benign childhood epilepsy with centrotemporal spikes |
most common epilepsy syndrome in childhood most children will outgrow the syndrome hence benign dx = eeg (EEG often shows centro-temporal spikes) tx usu. non but can use antiepileptics |
|
|
The cardinal features of rolandic epilepsy are infrequent, often single, focal seizures consisting of: |
a. unilateral facial sensorimotor symptoms (30% of patients) b. oropharyngolaryngeal manifestations (53% of patients) c. speech arrest (40% of patients), and d. hypersalivation (30% of patients) |
|
|
The cardinal features of rolandic epilepsy are infrequent, often single, focal seizures consisting of: |
face mouth and throat speech UP saliva others partial/focal seizures seizures occur at night usu. good prog. |
|
|
You review a 7-year-old girl who has cerebral palsy. She is having ongoing problems with spasticity in her legs which is causing pain and contractures. On speaking to her mother you ascertain that she is having regular physiotherapy, using the appropriate orthoses and has tried oral diazepam in the past. Which one of the following treatments may she be offered to try and improve her symptoms? |
Baclofen nb tx for spasticity include oral diazepam, oral and intrathecal baclofen, botulinum toxin type A, orthopaedic surgery and selective dorsal rhizotomy anticonvulsants, analgesia as required |
|
|
A 10-year-old boy who is known to have asthma is reviewed. He currently uses salbutamol prn, beclometasone 100mcg bd and recently had a trial of salmeterol 50mcg bd. Unfortunately he has noticed no benefit from adding salmeterol. What is the most appropriate next step in management? |
Stop salmeterol + increase beclometasone to 200mcg bd |
|
|
A 6-year-old boy is diagnosed as having nephrotic syndrome. A presumptive diagnosis of minimal change glomerulonephritis is made. What is the most appropriate treatment? |
Prednisolone A renal biopsy is only indicated if response to steroids is poor cyclophosphamide is the next step for steroid resistant cases |
|
|
Minimal change disease |
nearly always presents as nephrotic syndrome, accounting for 75% of cases in children and 25% in adults majority of cases are idiopathic around 10-20% a cause is found:drugs: NSAIDs, rifampicin Hodgkin's lymphoma, thymoma infectious mononucleosis |
|
|
Minimal change disease pathophys |
T-cell and cytokine mediated damage to the glomerular basement membrane → polyanion loss the resultant reduction of electrostatic charge → increased glomerular permeability to serum albumin |
|
|
Minimal change disease Prognosis is overall good, although relapse is common. Roughly: |
1/3 have just one episode 1/3 have infrequent relapses 1/3 have frequent relapses which stop before adulthood |
|
|
A baby is born by elective Caesarean section at 38 weeks performed due to pregnancy-induced hypertension. At one hour the female baby is noted to be grunting with mild intercostal recession. Oxygen saturations are 95-96% on air. What is the most likely cause of her respiratory distress? |
Transient tachypnoea of the newborn is the commonest cause of respiratory distress in the newborn period. It is caused by delayed resorption of fluid in the lungs |
|
|
Transient tachypnoea of the newborn |
difficulty breathing due to delayed resorption of fluid in the lungs more common following Caesarean sections, possibly due to the lung fluid not being 'squeezed out' during the passage through the birth canal |
|
|
CXR findings for Transient tachypnoea of the newborn |
may show hyperinflation of the lungs and fluid in the horizontal fissure |
|
|
Transient tachypnoea of the newborn mgmt |
Supplementary oxygen may be required to maintain oxygen saturations. Transient tachypnoea of the newborn usually settles within 1-2 days |
|
|
Which one of the following is a contraindication to receiving the pneumococcal vaccine? |
Current febrile illness |
|
|
Which one of the following vaccines uses an inactivated preparation of the organism or virus? |
Influenza (intramuscular) |
|
|
live attenuated vaccines |
MOOOIBY Live MMR Oral - Typhoid, Polio, Rotavirus I = INfluenza (IntraNasally) BCG Yellow fever |
|
|
Inactivated vaccines = RABItZ |
RABies InfluenZa (IM) |
|
|
What is the most appropriate way to confirm a diagnosis of pertussis? |
Per nasal swab |
|
|
Which one of the following is not part of the Apgar score for assessing the newborn? |
Capillary refill time apgar includes: Colour Respiratory effort Tone Heart rate and reflex iritability |
|
|
craniosyntosis |
when the growth plates of the skull fuse and don't allow the brain to grow |
|
|
A 11-week-old boy is reviewed in surgery. As part of a general assessment his head circumference is noted to be between the 0.4th and 2nd centile. Which one of the following would not explain this finding? |
Fragile X syndrome Whilst not a classic cause of macrocephaly, children with Fragile X syndrome tend to have a head larger than normal |
|
|
Microcephaly may be defined as |
occipital-frontal circumference < 2nd centile |
|
|
Microcephaly causes |
normal variation e.g. small child with small head familial e.g. parents with small head congenital infection perinatal brain injury e.g. hypoxic ischaemic encephalopathy fetal alcohol syndrome syndromes: Patau craniosynostosis |
|
|
A mother brings her son in to surgery as she suspects he has a squint. She thinks his right eye is 'turned inwards'. You perform a cover test to gather further information. Which one of the following findings would be consistent with a right esotropia? |
On covering the left eye the right eye moves laterally to take up fixation |
|
|
Squints may be classified as to where the eye deviates toward |
the nose: esotropia temporally: exotropia superiorly: hypertropia inferiorly: hypotropia |
|
|
Which one of the following statements regarding bronchiolitis is true? |
Peak incidence is 3-6 months of age |
|
|
A 4-year-old boy is noted to have macrocephaly and learning difficulties. What is the most likely diagnosis? |
Fragile X |
|
|
head lice |
Head lice (also known as pediculosis capitis or 'nits') is a common condition in children caused by the parasitic insect Pediculus capitis, which lives on and among the hair of the scalp of humans |
|
|
Which one of the following is not a recommended management option for head lice? |
Benzyl benzoate |
|
|
Which of the following is recommended management option for head lice? |
Isopropyl myristate and cyclomethicone Wet combing Dimeticone Malathion nb insecticides e.g. malathion, permethrin, phenothrin |
|
|
dx of head lice |
fine toothed combing of wet/dry hair to find live lice |
|
|
head lice |
its an insect so you can tx with insecticides e.g. Malathion Permethrin Phenothrin |
|
|
What is the most likely outcome following the diagnosis of minimal change nephropathy in a 10-year-old male? |
Full recovery but with later recurrent episode |
|
|
When assessing an 18-month-old child with diarrhoea and vomiting which one of the following signs is most likely to indicate shock? |
Prolonged capillary refill time |
|
|
An 8-year-old boy is reviewed in the Enuresis clinic. He is still wetting the bed at night despite using an enuresis alarm for the past three months. There are no problems with micturition during the daytime and he passes one soft stool everyday. Which one of the following treatments is most likely to be offered? |
Desmopressin |
|
|
Enuresis may be defined as the |
'involuntary discharge of urine by day or night or both, in a child aged 5 years or older, in the absence of congenital or acquired defects of the nervous system or urinary tract' |
|
|
A 14-year-old attends surgery. She was diagnosed with having migraines three years ago and requests advice about options for treating an acute attack. Which one of the following medications is it least suitable to recommend? |
Aspirin Avoid aspirin in children < 16 years as risk of Reye's syndrome nb Codeine would also be a poor choice as it has limited benefit in migraine. |
|
|
Migraine: management |
general rule 5-HT receptor agonists are used in the acute treatment of migraine whilst 5-HT receptor antagonists are used in prophylaxis |
|
|
acute tx for migraine 1st line |
oral triptan + NSAID/paracetamol |
|
|
What percentage of male term infants are found to have an undescended testicle on newborn examination? |
2-4% nb but is much more common if the baby is preterm. Around 25% of cases are bilateral |
|
|
Complications of undescended testis |
infertility torsion testicular cancer (MOST IMPORTANT) psychological |
|
|
MGMT OF UNDESCENDED TESTIS |
orchidopexy: referral should be considered from around 6 months of age. Surgical practices vary although the majority of procedures are performed at around 1 year of age |
|
|
You are reviewing a 11-month-old baby with a viral upper respiratory tract infection. She is clinically well but at the end of the consultation her mother asks you about her development. You notice that she points and babbles 'mama' and 'dada' but has no other words. She is shy and cries when you try to examine her. There is an early pincer grip and she can roll from front to back but she cannot yet sit without support. How would you describe her development? |
Isolated delay in gross motor skills |
|
|
A newborn infant is noted to have posterior displacement of the tongue and a clef palate. What is the most likely diagnosis? |
Pierre-Robin syndrome |
|
|
A 9-year-old girl is brought to surgery due to persistent leg pains. Which one of the following would not be consistent with a diagnosis of 'growing pains'? |
Present upon waking in the morning |
|
|
A 9-year-old boy is brought to surgery as his asthma has been getting worse over the past 2 days. His mother is concerned that his breathing is getting worse and not responding to inhaled salbutamol as normal. Given the overall clinical context, which one of the following is most consistent with a life-threatening asthma attack in this particular patient? |
Quiet breath sounds on auscultation NB SpO2 < 92%PEF < 33% best or predicted Silent chest Poor respiratory effort Altered consciousness Cyanosis |
|
|
Asthma in children: assessment of acute attacks |
BASED on age 1) b/w 2-5yo 2) GT 5 and they split into moderate, severe and life threatening attack |
|
|
Which one of the following conditions is not associated with obesity in children? |
GH excess |
|
|
is DS associated with obesity |
YES |
|
|
What is the average age that puberty starts in boys? |
12 YO |
|
|
A 3-year-old boy from a Turkish family is referred to the local paediatric unit due to recurrent lethargy and pallor. His parents report no other symptoms such as fever, pain or poor feeding. He had been treated with a course of ciprofloxacin for otitis externa two weeks ago. Admission bloods show: |
Glucose-6-phoshate dehydrogenase deficiency Ciprofloxacin is a common cause of haemolysis in patients with glucose-6-phoshate dehydrogenase deficiency |
|
|
Glucose-6-phosphate dehydrogenase (G6PD) deficiency |
is the commonest red blood cell enzyme defect It is more common in people from the Mediterranean and Africa and is inherited in a X-linked recessive fashion Many drugs can precipitate a crisis as well as infections and broad (fava) beans |
|
|
Glucose-6-phosphate dehydrogenase (G6PD) deficiency PATHOPHYS |
↓ G6PD → ↓ glutathione → increased red cell susceptibility to oxidative stress |
|
|
Glucose-6-phosphate dehydrogenase (G6PD) fxs |
neonatal jaundice is often seen intravascular haemolysis gallstones are common splenomegaly may be present Heinz bodies on blood films |
|
|
Glucose-6-phosphate dehydrogenase (G6PD) dx |
enzyme assay |
|
|
G6PD deficiency Some drugs causing haemolysis |
anti-malarials: primaquine ciprofloxacin sulph- group drugs: sulphonamides, sulphasalazine, sulfonylureas |
|
|
G6PD deficiency Some drugs thought to be safe |
penicillins cephalosporins macrolides tetracyclines trimethoprim |
|
|
G6PD deficiency is similar to |
hereditary spherocytosis |
|
|
Comparing G6PD deficiency to hereditary spherocytosis |
Gender G6PD deficiency M (X linked recessive) Hereditary spherocytosis M=F (AD) |
|
|
Comparing G6PD deficiency to hereditary spherocytosis |
BLOOD FILM different G6= heinz bodies HS = spherocytes DIAGNOSTIC TEST G6 = measure enz. activity of G6 HS = osmotic fragibility test |
|
|
Which one of the following statements regarding absence seizures is incorrect? |
Seizures may be provoked by a child holding their breath nb Seizures are characteristically provoked by hyperventilation |
|
|
Which of the following statements regarding absence seizures is correct? |
Typical age of onset of 3-10 years old Sodium valproate and ethosuximide are first-line treatments There is a good prognosis The EEG characteristically shows a bilateral, symmetrical 3Hz spike and wave pattern |
|
|
first-line treatment for absent seizures |
sodium valproate and ethosuximide are first-line treatment good prognosis - 90-95% become seizure free in adolescence |
|
|
Which one of the following is least associated with fetal varicella syndrome FVS? |
Sensorineural deafness |
|
|
features of FVS include |
skin scarring, eye defects (microphthalmia), limb hypoplasia, microcephaly and learning disabilities |
|
|
Risk factors FOR GLUE EAR |
male sex siblings with glue ear higher incidence in Winter and Spring bottle feeding day care attendance parental smoking |
|
|
GLUE EAR TX AKA OTITIS MEDIA WITH EFFUSION |
GROMMET ADENOIDECTOMY |
|
|
Which one of the following statements regarding chickenpox in children is incorrect? |
Children are infectious once rash begins until all lesions have scabbed over |
|
|
Which of the following statements regarding chickenpox in children is correct? |
Systemic upset is usually mild Incubation period is 10-21 days Can be caught from someone with shingles Spread by the respiratory route |
|

A 9-month-old girl is generally unwell with a low-grade pyrexia, oral ulcers and the following appearance of her feet: Which one of the following is most likely to be responsible for this presentation? |
Coxsackie A16 THIS IS HAND, FOOT AND MOUTH DIS. |
|
|
Hand, foot and mouth disease |
It is caused by the intestinal viruses of the Picornaviridae family (most commonly coxsackie A16 and enterovirus 71). It is very contagious and typically occurs in outbreaks at nursery COCK/SACK can be stimulated by HAND, FOOT OR MOUTH |
|
|
Hand, foot and mouth disease |
mild systemic upset: sore throat, fever oral ulcers followed later by vesicles on the palms and soles of the feet |
|
|
Hand, foot and mouth disease |
COCK/SACK can be stimulated by HAND, FOOT OR MOUTH you can put cock into intestine via anus, and when it goes into the mouth it can cause sore throat and fever and oral ulcers grabbing it with you hands/feet with give you vesicles on those areas |
|
|
Which one of the following is the most likely result if a fetus is homozygous for alpha-thalassaemia? |
Hydrops fetalis nb Alpha-thalassaemia is due to a deficiency of alpha chains in haemoglobin |
|
|
alpha thalassaemia |
Alpha-thalassaemia is due to a deficiency of alpha chains in haemoglobin 2 separate alpha-globulin genes are located on each chromosome 16 Clinical severity depends on the number of alpha chains present (normal = 4 alpha chains) If 1 or 2 alpha chains are absent then the blood picture would be hypochromic and microcytic, but the Hb level would be typically normal Loss of 3 alpha chains results in a hypochromic microcytic anaemia with splenomegaly. This is known as Hb H disease If all 4 alpha chains absent (i.e. homozygote) then death in utero (hydrops fetalis, Bart's hydrops) |
|
|
Which one of the following is associated with tall stature? |
Homocystinuria |
|
|
Causes of tall stature |
constitutional excessive growth hormone (pituitary gigantism) hyperthyroidism Marfan syndrome homocystinuria Klinefelter's syndrome |
|
|
The parents of a 9-year-old child come for advice regarding malaria prophylaxis. They are of Indian origin and are due to go back to their own country for a wedding. Which one of the following is contraindicated? |
Doxycycline |
|
|
The mother of a 4-year-old boy comes to surgery as she is concerned he is still wetting the bed at night. This is in contrast to his older brother who was dry at night by the age of 3 years. She is wondering if there is any treatment you can offer. What is the most appropriate management? |
Reassurance and advice on fluid intake, diet and toileting behaviour |
|
|
NICE MGMT for nocturnal enuresis |
1) stop causes/triggers 2) advise on fluid intake, diet and toilet behav. 3) reward system 4a) enuresis alarm if LT 7yo OR 4b) desmopressin first line if over 7 yo |
|
|
cataract causes |
Cataracts: causes CATARAct: Congenital Aging Toxicity (steroids, etc), TORCH Accidents Radiation Abnormal metabolism (diabetes mellitus, Wilson's) |
|
|
A 44-year-old Bangladeshi man with a history of mitral stenosis and atrial fibrillation is diagnosed with tuberculosis. He is commenced on anti-tuberculosis therapy. Three weeks after starting treatment his INR has increased to 5.6. Which one of the following medications is most likely to be responsible for this increase? |
Isoniazid inhibits the P450 system |
|
|
A raised INR is a result of |
inhibited liver enzymes and so a decreased INR is due to inducers |
|
|
P450 enzyme system Induction usually requires prolonged exposure to the inducing drug, as opposed to P450 inhibitors, where effects are often seen rapidly |
Inducers of the P450 system include antiepileptics: phenytoin, carbamazepine barbiturates: phenobarbitone rifampicin St John's Wort chronic alcohol intake griseofulvin smoking (affects CYP1A2, reason why smokers require more aminophylline) |
|
|
Inhibitors of the P450 system include |
antibiotics: ciprofloxacin, erythromycin isoniazid cimetidine, omeprazole amiodarone allopurinol imidazoles: ketoconazole, fluconazole SSRIs: fluoxetine, sertraline ritonavir sodium valproate acute alcohol intake quinupristin |
|
|
A 62-year-old man with a history of type 2 diabetes mellitus and ischaemic heart disease presents to his GP with erectile dysfunction. Which one of the following medications would contraindicate the prescription of sildenafil? |
Isosorbide mononitrate Viagra? - contraindicated by nitrates and nicorandil |
|
|
Which part of bowel affected in hirscgsprungs |
Large bowel and rectum |
|
|
Causes of visual problems in children |
congenital: infection, cataracts prematurity - retinopathy of prematurity cerebral palsy optic atrophy e.g. hydrocephalus, optic nerve hypoplasia albinism |
|
|
Treatment for acne depends on the patient's age and sex, the extent and the severity of the acne, how long it has been present, and response to previous treatments. |
Treatment for mild acne includes topical anti-acne preparations, lasers and lights
Treatment for moderate acne adds acne antibiotics such as tetracyclines and/or antiandrogens such as birth control pill
Treatment for severe acne may require a course of oral isotretinoin. |
|
|
Acne may be classified into mild, moderate or severe: |
mild: open and closed comedones with or without sparse inflammatory lesions moderate acne: widespread non-inflammatory lesions and numerous papules and pustules severe acne: extensive inflammatory lesions, which may include nodules, pitting, and scarring |
|
|
Treatment for acne depends on the patient's age and sex, the extent and the severity of the acne, how long it has been present, and response to previous treatments. |
Treatment for mild acne includes topical anti-acne preparations, lasers and lights
Treatment for moderate acne adds acne antibiotics such as tetracyclines and/or antiandrogens such as birth control pill
Treatment for severe acne may require a course of oral isotretinoin. |
|
|
Acne may be classified into mild, moderate or severe: |
mild: open and closed comedones with or without sparse inflammatory lesions moderate acne: widespread non-inflammatory lesions and numerous papules and pustules severe acne: extensive inflammatory lesions, which may include nodules, pitting, and scarring |
|
|
A simple step-up management scheme often used in the treatment of acne is as follows: |
single topical therapy (topical retinoids, benzyl peroxide) topical combination therapy (topical antibiotic, benzoyl peroxide, topical retinoid)
oral antibiotics: e.g. Oxytetracycline, doxycycline. Improvement may not be seen for 3-4 months. Minocycline is now considered less appropriate due to the possibility of irreversible pigmentation. Gram negative folliculitis may occur as a complication of long-term antibiotic use - high-dose oral trimethoprim is effective if this occurs
oral isotretinoin: only under specialist supervision |
|
|
Fragile x fxs in male |
learning difficulties large low set ears, long thin face, high arched palate macroorchidism hypotonia autism is more common mitral valve prolapse |
|
|
At what age would the average child acquire the ability to crawl? |
9 months |
|
|
A 4-year-old boy is admitted after developing a haemarthrosis in his right knee whilst playing in the garden. The following blood results are obtained:
Platelets 220 * 109/l = norm
PT 12 secs = norm APTT 78 secs = sig. UP
Factor VIIIc activity Normal
What is the most likely diagnosis? |
Haemophilia B
A grossly elevated APTT may be caused by heparin therapy, haemophilia or antiphospholipid syndrome.
A normal factor VIIIc activity points to a diagnosis of haemophilia B (lack of factor IX). Antiphospholipid syndrome is a prothrombotic condition |