![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
327 Cards in this Set
- Front
- Back
|
What are the two developmental screens most commonly used by pediatricians? |
|
|
|
Developmental Delay |
performance in a certain developmental area lags significantly compared with average attainment in a given skill area |
|
|
Developmental Quotient |
development age/chronological age x 100 -- this gives an idea of the child's developmental status |
|
|
Developmental dissociation |
When there is a substantial difference in the rates of development between two skill areas |
|
|
What is the best indicator of future intellectual potential? |
language- both receptive and expressive |
|
|
What is the most common developmental delay in preschool children? |
language delay |
|
|
Mental Retardation |
as defined by the DSM IV-TR 1) IQ 2) onset prior to age 18 3) impaired adaptive functioning (in at least two of the following areas: communication, self-care, home living, social/interpersonal skills, work, leisure, health, and safety) * the cause of MR is only identified in about 1/2 of cases |
|
|
What are the most commonly used IQ tests in the Pediatric population? |
1. Wechsler - preschool and school age 2. Stanford-Binet - school age |
|
|
Mild, Moderate, Severe and Profound Mental Retardation by IQ |
|
|
|
How common in language delay in preschoolers? |
up to 15% of preschoolers have some sort of speech/language delay at one time or another. In most cases there is underlying biologic abnormality such as genetic syndrome etc |
|
|
Language disorders |
inability to understand or acquire vocabulary, grammatical rules, or conversation patterns of language (expressive and receptive disorder) |
|
|
Speech disorders |
difficulty producing sounds and rhythms of speech (expressive disorder) |
|
|
Phoentic disorders |
problems with articulation (expressive disorder) |
|
|
Dysfluency |
interruptions in the flow of speech - this is observed in many preschoolers and usually resolves by age 4 - true dysfluency = stuttering and is characterized by signs of tension and struggle when speaking, sound repetition, or complete speech blockage and significant impedes the ability to communicate |
|
|
What should any child with a suspected language delay receive? |
a full audiologic (hearing) assessment followed be referral to a speech pathologist * early and intensive speech therapy often results in significant and sustained improvement in communication skills over time |
|
|
What is the most common cause of mild-to-moderate hearing loss in young children |
otitis media with effusion |
|
|
Attention-deficity/hyperactivity disorder (ADHD) |
- syndrome characterized by inattention, hyperactivity and impulsivity, which are inconsistent with the developmental stage of the child and manifested through maladaptive behaviors - the classic form is more common in boys and is usually diagnosed during elementary school - school performance and peer relationships often suffer, placing the child at risk for low self-esteem - a form that is solely characterized by inattentiveness is more common in girls, and is often diagnosed later - symptoms persist into adulthood in the majority of patients |
|
|
Diagnosis of ADHD |
This is a clinical diagnosis and the inattention, hyperactivity and impulsivity must be present by age 7, persist for at least 6 months, and be observed in multiple environments - initial assessment relies firmly on history obtained from parents and teachers - age appropriate rating scales are available and standardized (Conner's Parent and Teacher Rating Scale) |
|
|
Management of ADHD |
|
|
|
Autistic spectrum disorder - definition - prevalence - gender distribution - age of typical diagnosis |
A collection of chronic, nonprogressive disabilities characterized by impairments in social interaction, communication, and behavior.
|
|
|
Autism - characteristics - what differentiates this condition from Asperger's syndrome |
|
|
|
Asperger's Syndrome - characteristics |
|
|
|
Management of Autistic Spectrum Disorder |
|
|
|
What is the best prognostic indicator for patients with Autistic Spectrum Disorder? |
The extent of language development during the preschool years |
|
|
Hand-foot-and mouth disease |

|
|
|
Giannoti-Crosti Syndrome (aka papular acrodermatitis of childhood) |

|
|
|
Varicella |
|
|
|
Herpes Zoster/Shingles - characteristics |

|
|
|
Management of herpes Zoster/shingles |
|
|
|
Molluscum contagiosum |

|
|
|
Treatment of Molluscum Contagiosum |
|
|
|
Verrucae- characteristics and types |
"warts"
|
|
|
Management of warts/verruca |
Treatment depends on the type of wart and location
|
|
|
Pityriasis Rosea |
|
|

|
Pityriasis Rosea- herald patch |
|
|
unilateral thoracic exanthem |

asymmetric periflexural exanthem of childhood
|
|
|
What are the most common cause of bacterial infections of the skin in children? |
group A beta-hemolytic streptococus or S. aureus |
|
|
Bullous impetigo |

|
|
|
Nonbullous impetigo- causes and characteristics |

|
|
|
Treatment of non-bullous impetigo |
|
|
|
Staphylococcal Scalded Skin Syndrome |

|
|
|
Treatment of staphyloccal scalded skin syndrome |
|
|
|
Folliculitis |
|
|
|
furuncles and carbuncles |
|
|
|
Treatment of superficial folliculitis |
|
|
|
Treatment of furuncles and carbuncles |
|
|
|
What is the cause of "hot tub folliculitis" and how is it managed? |
Pseudomonas aeruginosa - These lesions are self-limited so long as exposure is discontinued |
|
|
What are the two most common superficial fungal infections? |
Tricophyton and Microsporum |
|
|
What is the most common cause of tinea capitis in the US? How does this manifest? Treatment? |

Tricophyton tonsurans (although microsporum canis can be spread from animals)
|
|
|
Tinea corporis- presentation and treatment |

|
|
|
Tinea pedis- cause, presentation, and treatment |

|
|
|
Tinea cruris- cause, presentation, and treatment |

|
|
|
When are systemic antifungal drugs needed for superificial fungal infections? |
When these infections affect the hair or nails |
|
|
Tinea (pityriasis) versicolor- characteristics and treatment |

|
|
|
Diaper rash - causes, characteristics and treatment |

|
|
|
Acne vulgaris |
|
|
|
Pathogenesis of acne vulgaris |
|
|
|
Risk factors for acne vulgaris |
|
|
|
Treatment of acne vulgaris |
|
|
|
Psoriasis - characteristics, epidemiology |

|
|
|
eczema vs psoriasis |
Eczema generally affects flexural creases and is pruritic, while psoriasis generally affects extensor surfaces and is non-pruritic |
|
|
What bacterial commonly causes an exacerbation of psoriasis? |
Group A beta hemolytic streptococcus (S. pyogenes) |
|
|
Management of psoriasis |
|
|
|
Erythema multiforme |
|
|
|
What is the most common cause of Erythema Multiforme in children?? |
Herpes Virus type I |
|
|
Stevens-Johnson Syndrome (SJS) |
|
|
|
Toxic Epideral Necrolysis (TEN) |
|
|
|
Treatment of Erythema Multiforme (EM) |
|
|
|
treatment of SJS |
|
|
|
Treatment of TEN |
|
|
|
Allergic reactions to drugs |
|
|
|
Risk factors for melanoma and non-melanoma skin cancer in children |
|
|
|
Congenital nevi vs acquired nevi |
|
|
|
Acquired nevi |
|
|
|
Spitz nevus |

|
|
|
Halo nevus |

|
|
|
Prevention of skin cancers in children |
|
|
|
Infantile hemangiomas |

|
|
|
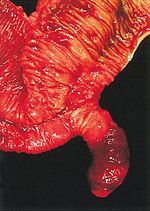
Superficial vs deep hemangiomas |

Superficial hemagiomas are bright red and non-compressible, whereas deep hemangiomas are subcutaneous, compressible and often have a bluish hue and superficial telangiectasias * Image shows deep infantile hemangioma
|
|
|
Management of infantile hemagiomas |
|
|
|
Type I Diabetes Mellitus - definition, symptoms, risk factors, epidemiology |
|
|
|
At what blood glucose level does glucose start appearing in the urine and leading to osmotic diuresis? |
180 mg/dL |
|
|
What is the most common endocrine disease in childhood and what is the prevalence of this disease? |
Type I Diabetes Mellitus - 0.25-0.5% of the population (1 in 400 children)
|
|
|
If a child is suspected of being in DKA, what questions should be asked during the history? |
|
|
|
Presentation of a child with DKA |
|
|
|
Symptoms of hypoglycemia |
|
|
|
Causes of secondary diabetes |
Secondary diabetes can be caused by insulin antagonism from excess glucocorticoids (Cushing syndrome or iatrogenic), hyperthyroidism, pheochromocytoma, GH excess, or medications such as thiazide diuretics |
|
|
Cystic Fibrosis Related Diabetes (CFRD) |
beta cell destruction from auto-digestion of the pancreas and inflammation |
|
|
Maturity-onset diabetes of the young (MODY) |
|
|
|
Diagnosis of Type I Diabetes Mellitus |
|
|
|
Blood chemistry in DKA |
|
|
|
Potassium in DKA |
|
|
|
Treatment of new-onset DM |
|
|
|
What is the starting insulin dose in a newly diagnosed type I diabetic? |
0.5-1 units per kg per day (40 kg child--> 20-40 units of insulin per day) divided in 2-3 doses - often a long acting insulin is given in the morning and then fast acting insulin/sliding scale is given with meals |
|
|
Treatment of DKA |
|
|
|
Annual screening for diabetic children |
|
|
|
Pathogenesis of Type II Diabetes Mellitus |
Type II DM is a polygenic condition that results from relative insulin resistance and beta cell dysfunction. The insulin resistance initially causes a compensatory increase in insulin secretion, however, with time there is a progressive decline in the glucose-stimulated insulin secretion |
|
|
Epidemiology of Type II DM |
|
|
|
Acanthosis nigricans |

skin condition involving hyperpigmentation and thickening of the skin folds, found primarily on the back of the neck and flexor areas, which may indicate DM |
|
|
What is the only oral diabetes medication approved for use in children? |
Metformin-- and only in children > 10 yo |
|
|
What is the definition of hypoglycemia - at what plasma and whole blood glucose level does it occur? |
plasma glucose < 50 mg/dL whole blood glucose < 60 mg/dL |
|
|
Causes of hypoglycemia |
|
|
|
Clinical manifestations of hypoglycemia |
These are divided into two categories: 1) activation of the autonomic nervous system and release of epinepherine, 2) neuroglycopenia
|
|
|
Evaluation of hypoglycemia |
|
|
|
Diabetes Insipidus - definition and causes |
|
|
|
Clinical manifestations of diabetes insipidus |
|
|
|
Diagnosis of DI |
|
|
|
Treatment of DI |
Administration of Desmopressin acetate (DDAVP), an ADH analogue that can be given intranasally, subQ, or orally |
|
|
SIADH |
Syndrome of Inappropriate ADH secretion-- excess ADH is released, resulting in:
|
|
|
Treatment of SIADH |
|
|
|
What are the two most common causes of short stature (causing 80% of cases)? |
familial/genetic short stature and constitutional delay. These both cause proportionate short stature, which is most commonly the case in pathologic causes as well |
|
|
What disorders can cause a disproportionate short stature? |
Rickets (vitamin D deficiency) and Achondroplasia (dwarfism) |
|
|
Causes of proportionate short stature |
|
|
|
What is the affect of precocious puberty on height? |
Initially there is a growth acceleration prior to their peers, however the patient then stops growing sooner and their final adult height is shorter than it would otherwise have been |
|
|
By what age to children with familial short stature manifest this condition? |
children with familial causes of short stature manifest growth curves at or below the 5%ile by 2 years of age.
|
|
|
Constitutional delay |
|
|
|
Growth hormone deficiency |
|
|
|
When should you suspect a tumor as the cause of growth problems? What tests should you order? |
|
|
|
What questions are important to ask in taking the history of someone who presents for evaluation of short stature in a child? |
|
|
|
In failure to thrive, what is the head circumference like generally compared with the height and weight? |
Height and weight are generally normal, whereas head circumference is normally spared |
|
|
What is the most common cause of hyperthyroidism in children? |
Grave's disease- an autoimmune disorder caused by circulating thyroid stimulating antibodies binding to throptropin receptors on thyroid cells, which results in diffuse hyperplasia and increased levels of T4. TSH is suppressed
|
|
|
Clinical manifestations of hyperthroidism |
|
|
|
Physical exam findings consistent with Grave's disease/hyperthyroidism |
|
|
|
Symptoms of malignant hyperthyroidism |
acute onset of tachycardia, hyperthermia, diaphoresis, fever, nausea, and vomiting = thyroid storm which can be life-threatening but is fortunately rare in children |
|
|
clinical manifestations in infants with neonatal Grave's disease |
staring, jittery, hyperactive, increased appetite but poor weight gain. Tachycardia is usually present and the thyroid may feel enlarged on palpation. There may also be evidence of CHF as the CV system is very sensitive to increased thyroid levels |
|
|
Treatment of neonatal Grave's disease |
Neonatal grave's disease generally resolves over the first several months of life as maternal antibodies are cleared. In infant who are not hemodynamically stable, IV fluids, digoxin, propanolol, and antithyroid meds may be needed |
|
|
Management of Grave's disease in children |
|
|
|
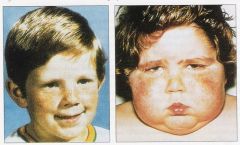
What is the most common cause of juvenile or acquired hypothyroidism? What are the characteristics of this disease? |
|
|
|
Clinical manifestations of hypothyroidism |
|
|
|
Diagnostic evaluation of hypothyroidism |
|
|
|
Treatment of hypothyroidism in children |
|
|
|
What is the most common type of congenital adrenal hyperplasia? What is elevated in this condition? What is decreased? |
21-hydroxylase deficiency. Lack of this enzyme leads to build up of the precursor 17-hydroxyprogesterone. There is decreased production of both cortisol and aldosterone. - this is an autosomal recessive condition |
|
|
What is elevated in 11-hydroxylase deficiency? What is decreased? |
11-deoxycortisol builds up and cortisol and aldosterone are both decreased - this is an autosomal recessive condition |
|
|
Clinical manifestations of 21-hydroxylase deficiency |
|
|
|
How is 21-hydroxylase deficiency diagnosed? |
Elevated serum levels of 17-hydroxyprogesterone > 5,000 ng/dL |
|
|
How does 21-hydroxylase deficiency differ from 11-hydroxylase deficiency in terms of electrolyte levels? |
In 11-hydroxylase deficiency there is a build up of deoxycorticosterone which has mineralocorticoid activity. This leads to hypernatremia, hypokalemia and hypertension-- the opposite of what is seen in 21-hydroxylase deficiency where there is decreased mineralocorticoids |
|
|
What is the treatment for congenital adrenal hyperplasia? |
|
|
|
Addison disease |
|
|
|
What are the causes of primary adrenal insufficiency in the newborn? |
|
|
|
What is the most common cause of primary adrenal insufficiency in older children and adolescents? |
Autoimmune adrenal insufficiency - other potential causes are tuberculosis, hemorrhage, fungal infection, neoplastic infiltration and HIV infection |
|
|
Adrenoleukodystrophy |
X-linked recessive disorder of long-chain fatty acid metabolism that results in adrenal insufficiency and progressive neurologic dysfunction |
|
|
What is the most common cause of ACTH deficiency (secondary adrenal insufficiency)? |
Chronic steroid therapy that results in pituitary suppression -- decreased ACTH * congenital hypopituitarism or pituitary tumors (craniopharyngioma) are also possible causes |
|
|
Adrenal crisis |
A medical emergency resulting from inadequate cortisol production that is characterized by fever, vomiting, dehydration and shock. This may be precipitated by intercurrent illness, trauma or surgery, especially if a stress dose of cortisol is not given in these situations |
|
|
What electrolyte abnormalities would you expect to see in untreated Addison's disease? |
|
|
|
Treatment of adrenal crisis? Addison's disease long-term management? |
|
|
|
Cushing syndrome - cause and symptoms |
|
|
|
What is the most common cause of cushing syndrome in children older than 7 yo? |
Cushing disease- bilateral adrenal hyperplasia due to a pituitary overproduction of ACTH (usually due to a pituitary adenoma) |
|
|
What is the most common cause of cushing syndrome in children younger than 7 yo? |
adrenal tumors |
|
|
How do you diagnose cushing syndrome? |
|
|
|
Treatment of cushing disease |
|
|
|
Precocious puberty- definition |
Secondary sex characteristics presenting in a girl before the age of 7 or a boy before the age of 9. This may be either gonadotropin dependent or independent. gonadotropin dependent is much more common. |
|
|
What is the difference in the etiology of precocious puberty in females vs males? |
|
|
|
McCune-Albright syndrome |

|
|
|
Precocious telarche |

|
|
|
Premature adrenarche |
|
|
|
How can you tell the difference between precocious puberty and precocious thelarche or premature adrenarche? |
In precocious thelarche, gonadotropin and estrogen levels are in the prepubertal range and their is no accelerated growth or advanced skeletal maturation. In premature adrenarche, adrenal androgens are elevated above norms for chronological age but are normal for the pubertal stage. The bone age is slightly advanced but there is a normal growth rate. In gonadotropin dependent precocious puberty there is development of secondary sex characteristics in combination with a growth spurt. There is advanced bone age and pubertal levels of LH, FSH, estrogen or testosterone. |
|
|
Treatment of precocious puberty |
If the cause if gonadotropin dependent, then GnRH (Leuprolide) is given. This suppresses the release of endogenous GnRH and decreases secondary sex characteristics, slows skeletal growth and prevents premature fusion of the epiphyseal plates |
|
|
Pubertal delay- definition |
|
|
|
What is the most common cause for pubertal delay? |
Constitutional delay- this account for 90-95% of cases and there is usually a family history of it. |
|
|
Differential diagnosis for pubertal delay |
|
|
|
What should the evaluation of pubertal delay include? |
|
|
|
Treatment of pubertal delay |
|
|
|
What are the body's two main regulators of calcium homeostasis? |
|
|
|
How does PTH act to increase serum calcium levels? |
|
|
|
What is the differential diagnosis of hypocalcemia? |
|
|
|
What is high risk for vitamin D deficiency and secondary hypocalcemia? |
|
|
|
Clinical manifestations of hypocalcemia |
|
|
|
What are serum calcium and phosphate levels like in hypoparathyroidism? Vitamin D deficiency? |
|
|
|
Treatment of functional hypoparathyroidism |
oral calcium supplements and an active metabolite of vitamin D (calcitriol) |
|
|
Differential diagnosis for hypercalcemia |
|
|
|
Clinical manifestations of hypercalcemia |
|
|
|
Treatment of hypercalcemia |
|
|
|
How do you calculate the amount of maintenance fluid needed for a child? |
|
|
|
What is the best type of maintenance IV fluid for children? |
|
|
|
Why are infants and toddlers particularly susceptible to dehydration? |
The immature kidneys have limited ability to conserve water and electrolytes. And because the child is dependent on their caretakers to supply them with hydration |
|
|
What are important benchmarks of the degree of dehydration in children? |
weight loss and decreased urine output |
|
|
Physical examination findings that are suggestive of dehydration? |
The primary mechanism of compensation for dehydration in children is tachycardia. IMPORTANTLY, while hypotension is sensitive early indicator of dehydration in adults, it is a very late and ominous finding in children! |
|
|
What is the definition of hypotonic/hyponatremia dehydration? |
Serum sodium less than 130 mEq/L -- this may happen in children who electrolytes or supplement with free water excessively |
|
|
Hypertonic (hypernatremic) dehydration |
serum sodium greater than 150 mEq/L. This is very uncommon in children, but can occur when there are excessive free water losses, such as in diabetes insipidus. |
|
|
What is the preferred treatment for mild-to-moderate dehydration in children? |
Oral rehydration therapy (ORT) with 90 mEq/L sodium, 20 mEq/L potassium, and 20 g/L of glucose. This is labor intensive as it requires small volumes of fluid to be given very frequently |
|
|
When there are fluid deficits, what timeline should be used to replace them? |
|
|
|
Hyponatremia 1. definition 2. signs and symptoms 3. when does this most often occur? |
|
|
|
What should the lab workup for hyponatremia entail? |
|
|
|
How does hyperglycemia affect measured serum sodium levels? How can it be corrected? |
|
|
|
What is the treatment of hyponatremia due to either SIADH or renal failure? |
Fluid restriction and treatment of the underlying disorder. |
|
|
When should hypertonic saline (3%) be used in the setting of hyponatremia? |
Its use should be reserved for life-threatening situations, such as intractable seizures |
|
|
Hypernatremia 1. definition 2. signs and symptoms 3. rate of correction |
|
|
|
Hyperkalemia 1. definition 2. most common cause in children 3. differential diagnosis 4. signs and symptoms |
|
|
|
What are the progressive ECG changes seen in the setting of hyperkalemia? |
|
|
|
Treatment of hyperkalemia |
|
|
|
Hypokalemia 1. definition 2. signs and symptoms 3. causes |
|
|
|
Progressive ECG changes seen in the setting of HYPOkalemia? |
|
|
|
What is the differential diagnosis for patients with hypokalemia and elevated blood pressure? |
|
|
|
What is the differential diagnosis for patients with hypokalemia, normal blood pressure, and increased urine potassium? |
|
|
|
What is the differential diagnosis for patients with hypokalemia, normal blood pressure, and decreased urine potassium? |
|
|
|
What is the most consistent physical exam finding in children with metabolic acidosis? |
Hypernea |
|
|
What is the most common and acid-base disorder and children and what is its definition? |
Metabolic acidosis- pH= 7.35 that results from either a loss of HCO3- or increased H+ in the extracellular fluid. |
|
|
How do you determine the expected PCO2 for adequate respiratory compensation in the setting of metabolic acidosis? |
Winter formula PaCO2 = 1.5 x HCO3- +8 (+/- 2)
|
|
|
What clinical manifestations are seen in metabolic acidosis? |
|
|
|
What lab workup should be conducted for metabolic acidosis? |
|
|
|
How do you calculate an anion gap and what is the normal range? |
(cations - anions) = (Na+ + K+) - (Cl- + HCO3-). Normal gap = 12 +/- 4 |
|
|
What are some causes of anion gap metabolic acidosis? |
|
|
|
What is the differential diagnosis for a non-anion gap metabolic acidosis? |
|
|
|
What is the differential diagnosis for a decreased anion gap metabolic acidosis? |
|
|
|
What is the treatment of metabolic acidosis? |
|
|
|
Metabolic alkalosis 1. definition 2. potential causes 3. potential complications 4. treatment |
|
|
|
Respiratory acidosis 1. Definition 2. Causes |
|
|
|
Respiratory alkalosis 1. definition 2. causes |
1. decrease in PaCO2 below 35 mmHg from a respiratory cause 2. lung disease-hyperventilation, mechanical ventilation or any cause (metabolic or neurological) that results in an increased respiratory rate |
|
|
Chronic abdominal pain 1. definition 2. most frequent cause in children |
1. at least three bouts of abdominal pain severe enough to affect activities over a period of at least 3 months 2. If there is no objective evidence of an underlying organic disorder, the abdominal pain is most often functional |
|
|
Differential diagnosis for acute abdominal pain in children |
|
|
|
Differential diagnosis for chronic abdominal pain in children |
|
|
|
What should you consider in the setting of abdominal pain, anemia, and poor growth? |
Celiac disease |
|
|
What is the most common surgical cause of abdominal pain in children? |
appendicitis |
|
|
What should you think of in a young child with intermittent severe bouts of abdominal pain which may also involve lethargy? |
intussusception |
|
|
What is the classic presentation of appendicitis in a child?
|
Fever, emesis, anorexia, diffuse periumbilical pain which then localizes to the RLQ. There is also commonly guarding, rebound tenderness, obturator, and psoas signs.
|
|
|
At what time from pain onset does the appendix typically perforate if it is going to?
|
36 hours after the pain begins
|
|
|
Treatment of appendicitis in children
|
|
|
|
What is one of the most common causes of intestinal obstruction in infancy?
|
intussusception
|
|
|
What are some potential lead points in intussusception?
|
Meckel diverticulum, intestinal polyp, lymphoma, or a foreign body
|
|
|
Clinical presentation of intussusception
|

|
|
|
Treatment of intussusception
|
|
|
|
Complications of persistent vomiting in children
|
|
|
|
What is important to determine when taking the history regarding a vomiting child?
|
|
|
|
Physical exam findings that suggest increased ICP as a cause for vomiting?
|
Bulging fontanelle, papilledema
|
|
|
Diagnostic evaluation of vomiting in a child
|
|
|
|
Pyloric stenosis
|

|
|
|
Malrotation and volvulus
|
Malrotation- occurs when the small intestines rotate abnormally in utero, resulting in malposition in the abdomen. When this improperly attached intestine twists on its own vascular supply, this is volvulus
|
|
|
What is the most common age for volvulus to present?
|
less than 1 month
|
|
|
Clinical manifestations of volvulus
|
|
|
|
Gastroesophageal reflux disease (GERD)
1. definition 2. diagnosis 3. clinical manifestations |
|
|
|
Treatment of GERD in children
|
|
|
|
Diarrhea vs enteritis vs colitis
|
1. Diarrhea- increase in the frequency and the water content of stools
2. Enteritis- small bowel inflammation 3. Colitis- large bowel inflammation |
|
|
What is the most common cause of acute diarrhea illness in the world?
|
Viral gastroenteritis
|
|
|
What findings on physical exam are consistent with diarrhea as a cause for abdominal pain?
|
|
|
|
Diagnostic evaluation of diarrhea in children
|
|
|
|
Treatment of diarrhea in children
|
|
|
|
Treatment of a child with a positive stool culture and a fever
1. younger than 3 months 2. infant older than 3 months 3. any infant who looks toxic or has a positive blood culture |
1. admit to the hospital, get blood culture and start IV abx. A LP and UA should be considered
2. admit to hospital, get blood culture, but wait on abx until results of the blood culture is known 3. admit for IV abx. Evaluate for pyelonephritis, meningitis, pneumonia, and osteomyelitis |
|
|
Treatment of C. difficile colitis
|
|
|
|
Constipation
1. definition 2. complications |
1. infrequent passage of hard, dry stools
2. impaction, abdominal pain, overflow diarrhea resulting from leakage around the fecal mass, anal fissure, rectal bleeding, UTI due to extrinsic pressure on the urethra, encopresis - accidental soiling/stooling |
|
|
What is the most common cause of constipation after the neonatal period?
|
Functional constipation- voluntary withholding of stool - 90-95%. This may be due to pain associated with defecating, which becomes worse as the stool becomes more hard with increasing constipation
|
|
|
When should an organic cause for constipation be sought out?
|
in any patient who fails to pass meconium in the first 24-48 hours of life (e.g. cystic fibrosis, hirshsprung disease)
|
|
|
Treatment of constipation during childhood
|
|
|
|
What is the preferred agent for disimpaction in children? for daily medication/prophylaxis?
|
Polyethylene glycol (PEG) 3350 for both. The goal is to achieve a soft (mashed potato consistency) stool on a daily or more frequent basis
|
|
|
Hirschsprung Disease- definition, characteristics and epidemiology
|
|
|
|
Diagnosis of Hirschsprung Disease
|

|
|
|
Treatment of Hirschsprung Disease
|
Treatment is generally surgical in two stages
1. creation of a diverting colostomy 2. resection of the aganglionic segment of the of the bowel and anastamosis of the ganglionic section with the rectum * This procedure is often postponed until the infant is 12 months old or 3-6 months after diagnosis in an older child |
|
|
GI bleeding in children- types
|
|
|
|
Differential diagnosis of upper GI (proximal to the ligament of Treitz) bleeds in children
|
|
|
|
What is the most common cause of minor rectal bleeding in children (stool streaked with blood)?
|
Anal fissure of polyp
|
|
|
Differential diagnosis of lower GI bleeds in children (distal to the ligament of Treitz)
|
|
|
|
What is the immediate priority in the assessment of a child with GI bleeding?
|
|
|
|
Diagnostic evaluation of a child with GI bleeding
|
|
|
|
Treatment of GI bleeding in children
1. what if there is a normal hgb or hct? 2. what should guide fluid replacement? |
1. a normal hgb or hct does not rule out severe acute bleeding as full hemodilution takes up to 12 hours in the acutely bleeding patient
2. IV normal saline or LR should be given in 20 mL/kg boluses until the vitals improve. Tachycardia should guide fluid replacement as hypotension is a late finding |
|
|
Meckel Diverticulum
1. definition 2. peak age of incidence |
1. vestigial remnant of the omphalomesenteric duct that is the most common anomaly of the GI tract
2. 2 years of age |
|
|
Clinical manifestations of meckel diverticulum
|
|
|
|
Diagnosis and Treatment of Meckel Diverticulum
|
|
|
|
Inflammatory Bowel Disease- types
|
|
|
|
Clinical manifestations of IBD
|
|
|
|
Definition of mild, moderate and severe disease in IBD
|
|
|
|
What is the risk of developing colon cancer in ulcerative colitis, and how should this risk be managed?
|
After 10 years of disease, there is a cumulative risk of 1-2% per year. After ten years, patients should have annual colonoscopy with biopsy.
|
|
|
What are some extraintestinal manifestations of IBD?
|
|
|
|
What does Upper GI studies of patients with crohn's disease often reveal?
|

ileal or proximal small bowel disease with segmental narrowing of the ileum ("string sign") and longitudinal ulcers
|
|
|
What type of anemia is common in IBD and why?
|
Megaloblastic anemia due to folate or B12 deficiency
( In Crohn's disease, the terminal ileum is often involved and this is where B12 is absorbed in the gut) |
|
|
Treatment of IBD in children
|
|
|
|
What is the period of childhood when the mortality rate is the highest?
|
The late fetal and early and neonatal period
|
|
|
What does the perinatal mortality rate refer to?
|
fetal deaths occurring from the 20th week of gestation until the 7th day after birth. Intrauterine death represents 40-50% of the perinatal mortality rate.
|
|
|
What does the neonatal mortality rate refer to?
|
infants who die between birth and 28 days of life
|
|
|
What does the postneonatal mortality rate refer to?
|
death between 28 days to the first year of life. Modern NICUs have allowed children with life-threatening diseases to live longer, leading to an increase in the postneonatal mortality rate when some of these children eventually die
|
|
|
What is the definition of infant mortality rate and how does it differ with respect to race?
|
|
|
|
APGAR Scoring
|
|
|
|
What does the APGAR at 1 minute reflect vs that at 5 minutes?
|
|
|
|
What does an APGAR score of 8-10 represent? 0-3?
|
|
|
|
What is assessed in APGAR measurements and how many points are awarded for what?
|
A- Appearance - Pale or cyanotic = 0 pts, cyanotic extremities = 1 pt, pink throughout = 2 pts
P- Pulse - absent = 0 pts, <100 = 1 pt, > 100 = 2 pts G- Grimace/reflex irritability- absent = 0 pts, grimace suction or aggressive stimulation = 1 pt, active cry and avoidance with stimulation A- Activity/ muscle tone- absent = 0 pts, weak, slightly flexed extremities = 1 pt, flexed arms and legs that resist extension = 2 pts R- Respiration - absent = 0 pts, irregular with weak cry, gasping = 1 pt, vigorous cry = 2 pts |
|
|
Cephalohematoma
1. definition 2. predisposing factors 3. course 4. complications |

|
|
|
Caput Succedaneum
1. definition 2. how does it form and when is it usually seen? |

|
|
|
Clavicle Fractures in Neonates
1. prevalence 2. Which clavicle is more likely to be fractured? 3. Predisposing factorss 4. How is this usually diagnosed and what is the appropriate management? |
|
|
|
Erb Palsy in Neonates
1. definition 2. When should this be expected? 3. Management? |
1. Injury to the nerves of the brachial plexus (C5 and C6) that results from excessive traction on the neck, leading to paresis. The infant's arm will be held in the waiter's tip position, with the arm extended and the wrist flexed.
2. If there is an absent Moro reflex in the right arm and the right hand grasp is intact, then Erb palsy should be suspected. 3. 90% of these lesions will resolve spontaneously by 4 months of age. If the deficit persists ten nerve grafting should be considered. |
|
|
Low Birth Weight (LBW) vs Very Low Birth Weight (VLBW)
1. definitions 2. associated risks/complications 3. incidence over time |
1. LBW = infants weighing less than 2,500 g, VLBW = infants weighing less than 1,500 g
2. LBW infants make up only 7% of all births, but account for up to 2/3 of all neonatal deaths, whereas VLBW infants make up only 1% of all births but represent 50% of all neonatal deaths 3. Although the overall infant mortality rate has declined, there has NOT been an improvement/decrease in the number of LBW births. This is one of the reasons that the infant mortality rate in the US is the worst for any large, industrialized, modern country. However, the survival rate of LBWs s the highest in the US |
|
|
Causes of LBW
|
1. Premature Birth
2. Intrauterine Growth Retardation |
|
|
Causes of Premature Birth by category
1. fetal 2. placental 3. uterine 4. maternal 5. other |
|
|
|
Causes of Intrauterine Growth Retardation (IUGR) by category
1. Fetal 2. Placental 3. Maternal |
|
|
|
What are maternal factors associated with birth of a LBW infant?
|
|
|
|
Postmaturity
1. definition 2. cause 3. Clinical manifestations 4. Treatment |
|
|
|
Small for Gestational Age (SGA)
1. Definition 2. Incidence 3. Pathogenesis - (early onset and late onset) |
|
|
|
Factors to consider in delivery of SGA neonates
|
|
|
|
Large for Gestational Age (LGA)
1. definition 2. risk factors 3. complications and perinatal management |
|
|
|
Macrosomia
1. definition 2. macrosomia vs LGA 3. complications 4. risk factors |
1. Birth Weight > 4000 g
2. All macrosomic infants are LGA, but not all LGA infants are macrosomic. 3. increased risk of shoulder dystocia and other birth trauma 4. maternal diabetes, obesity, and postmaturity |
|
|
Polyhydramnios
1. definition 2. causes of/associations with acute polyhydramnions 3. causes of chronic polyhydramnios |
|
|
|
Oligohydramnios
1. associations 2. complications 3. intrapartum management |

Decreased amniotic fluid volume
1. IUGR, postmaturity, congenital anomalies of the fetal kidneys 2. bilateral renal agenesis results in Potter syndrome - clubbed feet, compressed facies, low-set ears, scaphoid abdomen, and diminished chest wall size accompanied by pulmonary hypoplasia. Uterine compression in the absence of amniotic fluid retards lung growth and patients with this condition often die from respiratory failure or renal failure. 3. The risk for fetal distress during labor can be reduced by normal saline amnioinfusion |
|
|
Neonatal sepsis
1. early-onset sepsis 2. late-onset sepsis 3. nosocomial sepsis |
1. birth to 3 days- caused by bacteria residing in the mother's GU tract. Responsible organisms include: group B Strep, E. coli, Klebsiella, and Listeria. Administration of penicillin to mother's with GBS colonization can decrease this risk. Risk factors include prolonged ROM (>24 hours), chorioamnionitis, maternal fever or leukocytosis, fetal tachycardia, preterm birth, African American race, and male sex
2. late-onset sepsis- occurs between 3-28 days, and often happens in a full-term baby who was discharged healthy from the hospital. Bacteremia can lead to meningitis (GBS or E.coli), osteomyelitis (GBS or S. aureus), arthritis (N. gonorrhea, S. aureus, Candida albicans, or gram neg bacteremia) and UTI (gram neg bacteremia) 3. Nocosomially acquired sepsis- day 3- discharge- usually occurs in premature infants in the NICU as many of these infants are colonized by multidrug resistant bacteria indigenous to the NICU. Multiple indwelling devices increases the risk of this. Main culprits include: S. aureus, S. epidermidis, gram neg bacteria and candida albicans |
|
|
About what % of women in the US are positive for GBS at that time of delivery?
|
About 20% -- need penicillin intrapartum
|
|
|
Clinical manifestations of early-onset sepsis
|
|
|
|
Clinical manifestations of late-onset sepsis
|
|
|
|
Evaluation of early-onset sepsis
|
|
|
|
Evaluation of late-onset sepsis
|
Very similar to the evaluation of early-onset sepsis, except more attention is given to the bones, lab values and urine culture (via suprapubic aspiration or urethral catheterization)
|
|
|
Treatment of early-onset or late-onset sepsis
|
|
|
|
Treatment of nosocomial sepsis
|
|
|
|
Risk of Chlamydia infection in the newborn
|
|
|
|
Clinical manifestations of chlamydia infection in the newborn
|

|
|
|
Treatment of chlamydial infection in the newborn
|
14 days of oral erythromycin, as topical treatment of the conjunctivitis is often ineffective and does not treat or prevent pneumonia. Test mother and treat her as well as all partners.
|
|
|
What is the most common cause of respiratory failure in newborn infants?
|
Respiratory Distress Syndrome (hyaline membrane disease)
|
|
|
Respiratory Distress Syndrome - pathophysiology
|
|
|
|
How can fetal lung maturity be predicted in utero?
|
Measurement of amniotic fluid lethicin to sphingomyelin ratio (>2 if mature) and phosphatidylglycerol content (present if mature).
|
|
|
How can the production of surfactant be accelerated when delivery is expected to be pre-term?
|
Administration of steroids.
The following have also been noted to accelerate fetal lung maturity:
|
|
|
What maternal factors have been noted to increase the risk of Respiratory Distress Syndrome
|
|
|
|
Clinical manifestations of Respiratory Distress Syndrome
|
within the first few hours of life:
|
|
|
What is the natural course of neonatal Respiratory Distress Syndrome
|
|
|
|
Acute complications of neonatal RDS
|
|
|
|
Treatment of neonatal RDS
|
|
|
|
Bronchopulmonary dysplasia
|
|
|
|
Meconium production, incidence, and risk factors for intrauterine passage
|
|
|
|
Meconium Aspiration Syndrome |
|
|
|
Clinical manifestations of Meconium Aspiration Syndrome |

|
|
|
Treatment of Meconium Aspiration Syndrome |
|
|
|
Persistent Pulmonary Hypertension of the Newborn |
|
|
|
Risk Factors for Pulmonary Hypertension of the Newborn (PPHN) |
|
|
|
Clinical manifestations of PPHN |
|
|
|
Treatment of persistent pulmonary hypertension of the newborn |
|
|
|
Manifestations of hyperbilirubinemia and at what level of bilirubin is it noticeable in a) neonates and b) older children? |
|
|
|
What are the potential dangers associated with neonatal hyperbilirubinemia? |

Kernicterus - yellow staining of the basal ganglia and hippocampus, resulting in widespread cerebral dysfunction. Clinical features include lethargy, irritability, hypotonia, opisthotonos (state of severe hyperextension and spasticity), seizures, mental retardation, cerebral palsy, and hearing loss |
|
|
Physiologic jaundice |
|
|
|
breast milk jaundice |
|
|
|
When should intervention be considered in neonatal jaundice |
|
|
|
What history is essential to gather in the setting of neonatal hyperbilirubinemia? |
|
|
|
How might you determine the extent of hyperbilirubinemia/jaundice in a neonate by physical exam? |
jaundice tends to progress in a cephalopedal sequence, so infants with clinically apparent jaundice below the umbilicus are likely to have higher levels than those with only facial jaundice |
|
|
Diagnostic evaluation of neonatal jaundice |
|
|
|
Treatment of neonatal jaundice |
|