Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
236 Cards in this Set
- Front
- Back
|
MICRODONTIA is more common in:
|
females
|
|
|
MACRODONTIA is more common in:
|
males
|
|
|
What is TRUE GENERALIZED MICRODONTIA?
|
All teeth are smaller than normal. Uncommon, seen in examples like pituitary dwarfism
|
|
|
What is RELATIVE MICRODONTIA?
|
Normal-sized teeth in larger than normal jaws, macrognathia
|
|
|
What is the most frequent case of ISOLATED MICRODONTIA?
|
Maxillary lateral incisors
|
|
|
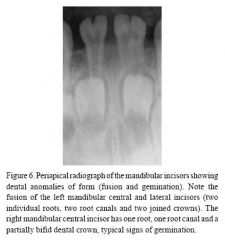
What is GEMINATION?
|
A single enlarged tooth or joined (double) tooth in which the tooth count is normal when the anomalous tooth is counted as one.
|
|
|
GEMINATION has a higher frequency in which group of teeth?
|
Anteriors
|
|
|
GEMINATION: ______ are most often affected of the permanent dentition, and ______ are most often affected of the deciduous dentition.
|
1. maxillary permanent incisors
2. mandibular deciduous incisors |
|
|
What is FUSION?
|
A single enlarged tooth or joined tooth in which the tooth count reveals a missing tooth when the anomalous tooth is counted as one.
|
|
|
What are possible complications of FUSION and/or GEMINATION?
|
crowding
abnormal spacing delayed or ectopic eruption of underlying permanent teeth |
|
|
What is CONCRESCENCE?
|
Union of two fully formed teeth, joined along the root surfaces by cementum.
|
|
|
Which teeth are most commonly affected by CONCRESCENCE?
|
Maxillary molars
|
|
|
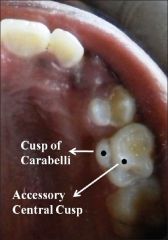
What is the CUSP OF CARABELLI?
|
An additional cusp typically seen on the palatal surface of the mesiolingual cusp of a maxillary molar
|
|
|
What is the most common example of supernumerary cusps?
|
CUSP OF CARABELLI
|
|
|
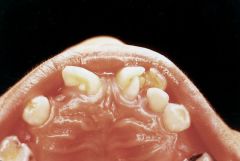
What is a TALON CUSPID?
|
An additional cusp located on the surface of an anterior tooth
|
|
|
TALON CUSPIDS are found predominantly on which tooth?
|
permanent maxillary lateral
|
|
|
TALON CUSPIDS occur more frequently in which ethnic groups?
|
Asian
Native American Inuit Arab |
|
|
What is the main reason TALON CUSPS get removed?
|
Interfere with occlusion
|
|
|
Describe DENS EVAGINATUS:
|
A focal area of crown that projects outward and produces what appears as an extra-cusp centrally located on occlusal surface b/w buccal and lingual cusps of premolars and occasionally in molars
|
|
|
What is the occurrence pattern of DENS EVAGINATUS?
|
Typically occurs on premolar teeth
Usually bilateral Mandibular predominance - in Asians, Inuit and N.Americans |
|
|
Clinical features of the DENS EVAGINATUS:
|
Cusp contains enamel, dentin and pulp.
|
|
|
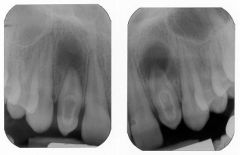
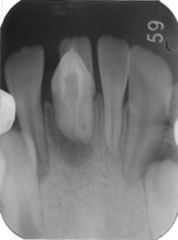
What is DENS INVAGINATUS?
|
A deep surface invagination of the crown or root that is lined by enamel
|
|
|
What is the occurence pattern of DENS INVAGINATUS?
|
Most commonly in maxillary lateral incisors, follow by central incisors, premolars, canines and molars
|
|
|
What is the clinical significance of DENS INVAGINATUS?
|
Predisposes the tooth to early decay and subsequent pulpitis.
|
|
|
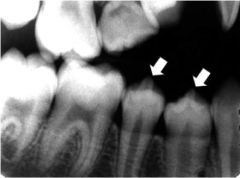
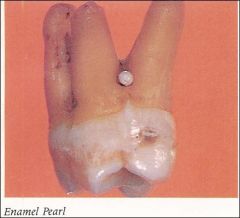
What are ENAMEL PEARLS?
|
small, spheric enamel projections located on the root surface.
|
|
|
What clinical significance is there of ENAMEL PEARLS?
|
Weak point of periodontal attachment and point of plaque retention.
Some contain vital pulp tissue |
|
|
What are the clinical features of ENAMEL PEARL?
|
A well-defined radiopaque nodule along the root surface
|
|
|
CERVICAL ENAMEL EXTENSIONS occur most frequently where?
|
Mandibular molars (1st -> 2nd -> 3rd)
|
|
|
What are TWO associated clinical findings of CERVICAL ENAMEL EXTENSIONS?
|
- localized loss of periodontal attachment with bifurcation involvement
- development of inflammatory cyst |
|
|
What is TAURODONTISM?
|
An enlargement of the body and pulp chamber of a multi-rooted tooth, with apical displacement of the pulpal floor and furcation of the roots.
|
|
|
What is the etiology of TAURODONTISM?
|
Probably from late invagination of Hertwig's root sheath.
|
|
|
What are some clinical features of TAURODONTISM?
|
- body of the tooth is enlarged at the expense of the roots
- constriction at CEJ is absent/reduced. - primarily affects permanent teeth |
|
|
How is diagnosis of TAURODONTISM made?
|
Radiography
|
|
|
What is the treatment for TAURODONTISM?
|
Not required, but can be a complicating factor during RCT
|
|
|
What is HYPERCEMENTOSIS?
|
non-neoplastic deposition of excessive cementum that is continuous with the normal radicular cementum.
|
|
|
What part of the root does HYPERCEMENTOSIS usually affect?
|
Apical third
|
|
|
What are the LOCAL factors associated with HYPERCEMENTOSIS?
|
- occlusal trauma
- adjacent inflammation - unopposed teeth - repair of vital root fracture |
|
|
What are the SYSTEMIC factors associated with HYPERCEMENTOSIS?
|
- Paget's disease of bone
- acromegaly |
|
|
What are the clinical features of HYPERCEMENTOSIS?
|
Teeth exhibit thickening and blunting of roots (bulbous pear shaped root) radiographically
Premolar teeth most commonly affected |
|
|
What complications may arise from HYPERCEMENTOSIS?
|
Problems during extraction
|
|
|
What is the clinical significance of SUPERNUMERARY ROOTS?
|
Detection is important when extractions or RCT are undertaken
|
|
|
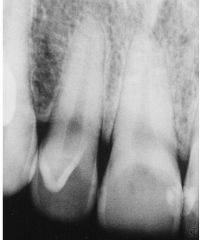
What is DILACERATION?
|
an abnormal curvature to the root
less frequently the crown |
|
|
What is the etiology of DILACERATION?
|
Most cases are idiopathic, other cases appear to be related to trauma to tooth during root development
|
|
|
What are some complications of DILACERATION?
|
- failure to erupt
- endodontic treatment (root perforation) - extraction (root fracture) |
|
|
Describe TRANSLUCENT enamel:
|
appears bluish-white and teeth appear yellow at cervical one-third and bluish-white at the incisal edge
|
|
|
Describe OPAQUE enamel:
|
gray-white and teeth are more uniform
|
|
|
What are EXTRINSIC STAINS?
|
abnormal teeth colourations arising from the surface accumulation of exogenous pigment
|
|
|
What are 5 main causes of EXTRINSIC STAINS?
|
- tobacco, food, beverage
- gingival hemorrhage - restorative materials - medications - antiseptics |
|
|
What are INTRINSIC STAINS?
|
Abnormal discolouration of teeth secondary to endogenous factors that result in the discolouration of the underlying dentin
|
|
|
What are 5 main causes of INTRINSIC STAINS?
|
- Trauma
- medications - Amelogenesis imperfecta, dentinogenesis imperfecta, fluoriosis - congenital erythropoietic porphyria - erythroblastosis fetalis |
|
|
What is CONGENITAL ERYTHROPOIETIC PORPHYRIA?
|
an autosomal recessive disorder of porphyrin metabolism that is responsible for the development of a defective pathway for the metabolism of hematoporphyrins, resulting in excessive porphyrins circulating in blood : leading to discolouration
|
|
|
Developmental alterations in the number of teeth. What is their pathogenesis?
|
Probably related to the development of excess or loss of dental lamina and influence by genetic and environmental factors.
|
|
|
What is ANODONTIA?
|
total lack of tooth development
|
|
|
ANODONTIA is often associated with which condition?
|
Ectodermal dysplasia
|
|
|
What is HYPODONTIA?
|
Lack of development of one or more teeth.
|
|
|
What is OLIGODONTIA?
|
Lack of development of six or more teeth.
|
|
|
What is the most common developmental abnormality?
|
Failure of teeth to form
|
|
|
An increased prevalence of hypodontia is noted in patients with which two conditions?
|
- nonsyndromic cleft lip
- cleft palate |
|
|
HYPODONTIA is associated with which 4 conditions?
|
- microdontia
- reduced alveolar development - increased freeway space - retained primary teeth |
|
|
In PRIMARY IMPACTION what are the three risks of non-intervention?
|
- development of pathologic conditions ie cyst/tumour
- crowding of the dentition - resorption and worsening of the periodontal status of adjacent teeth |
|
|
In PRIMARY IMPACTION what are the 6 risks of intervention?
|
- sensory loss
- alveolitis - trismus - infection - fracture - TMJ injury to adjacent teeth |
|
|
The most critical discovery related to HYPODONTIA is in which gene mutation?
|
AXIN2 gene
|
|
|
AXIN2 gene mutation has also been associated with development of what?
|
- adenomatous polyps of the colon
- colorectal carcinoma |
|
|
What are the most commonly affected teeth for HYPODONTIA?
|
THIRD MOLARS > 2nd premolars > lateral incisors
|
|
|
HYPODONTIA occurs more frequently in which gender?
|
FEMALES
|
|
|
Define SUPERNUMERARY:
|
additional teeth
|
|
|
HYPERDONTIA occurs more commonly in which gender?
|
MALE
|
|
|
HYPERDONTIA may be associated with what two conditions?
|
- Gardner's syndrome
- Cleidocranial dysplasia |
|
|
What are the two categories of supernumerary teeth?
|
- supplemental (normal size and shape)
- rudimentary (abnormal shape and smaller size) |
|
|
Define MESIODENS:
|
supernumerary between maxillary anterior incisors
|
|
|
Define DISTODENS:
|
fourth molar
|
|
|
Define NEONATAL TEETH:
|
teeth arising within the first 30 days of life
|
|
|
Define PRIMARY IMPACTION:
|
teeth that cease to erupt before emergency
|
|
|
What teeth are more commonly impacted?
|
MAND THIRD MOLAR > Max third molar > max cuspids
|
|
|
What is the treatment of an IMPACTED TOOTH?
|
- surgical removal most frequently
- long-term observation - orthodontic assisted eruption - transplantation |
|
|
What is the risk of NON-INTERVENTION for an IMPACTED TOOTH?
|
- development of pathologic conditions (cyst/tumour)
- crowding of dentition - resorption or worsening of the periodontal status of adjacent teeth |
|
|
What is the risk of INTERVENTION for an IMPACTED TOOTH?
|
- sensory loss
- alveolitis - trismus - infection - fracture - TMJ injury to adjacent teeth |
|
|
Define ANKYLOSIS:
|
cessation of eruption after emergency / occurs from fusion of the tooth with surrounding bone
|
|
|
ANKYLOSIS occurs more commonly in which teeth?
|
erupted primary molars
|
|
|
What are the clinical features of ANKYLOSIS?
|
- absence of PDL space
- sharp, solid sounds on percussion (only when 20% of the root is fused to the bone) |
|
|
What is the treatment of an ANKYLOSED TOOTH?
|
- extraction of the tooth to allow for eruption of the underlying permanent tooth and space maintenance
|
|
|
ANKYLOSED TEETH that are allowed to remain in position can lead to what:
|
- occlusal and periodontal problems
- over-eruption of the opposing teeth - the adjacent teeth often incline toward the affected tooth - occasionally impaction of the underlying permanent tooth |
|
|
Define ATTRITION:
|
loss of tooth structure caused by TOOTH-TO-TOOTH contact during occlusion and mastication.
|
|
|
Define ABRASION:
|
Pathologic loss of tooth structure as a result of an abnormal habit or an abnormal use of abrasive substances orally
|
|
|
What is the most common cause of ABRASION in the mouth?
|
aggressive toothbrushing
|
|
|
What are some other common causes of ABRASION in the mouth?
|
- thread biting
- pipe stems - bobby pin - inappropriate dental floss use - toothpicks |
|
|
Define EROSION:
|
The loss of tooth structure from a non-bacterial chemical process
|
|
|
What are some etiologic factors of EROSION of teeth?
|
ACIDS from:
- foods - medications - internal sources - industrial atmosphere - swimming pools |
|
|
What is the CLASSIC pattern of EROSION of teeth?
|
cupped lesion
|
|
|
What is bla bla
|
bla
|
|

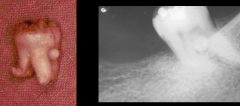
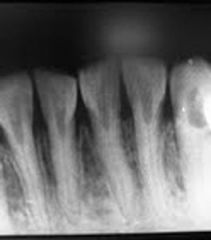
Identify the dental abnormality:
|
MICRODONTIA
|
|

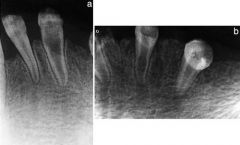
Identify the dental abnormality:
|
MICRODONTIA
|
|

Identify the dental abnormality:
|
MICRODONTIA
|
|

Identify the dental abnormality:
|
MICRODONTIA
|
|

Identify the dental abnormality:
|
MICRODONTIA
|
|

Identify the dental abnormality:
|
MACRODONTIA
|
|

Identify the dental abnormality:
|
MACRODONTIA
|
|

Identify the dental abnormality:
|
MACRODONTIA
|
|

Identify the dental abnormality:
|
MACRODONTIA
|
|

Identify the dental abnormality:
|
GEMINATION/FUSIOn
|
|

Identify the dental abnormality:
|
GEMINATION/FUSIOn
|
|

Identify the dental abnormality:
|
GEMINATION/FUSIOn
|
|

Identify the dental abnormality:
|
GEMINATION/FUSIOn
|
|
Identify the dental abnormality:
|
GEMINATION/FUSIOn
|
|

Identify the dental abnormality:
|
GEMINATION/FUSIOn
|
|

Identify the dental abnormality:
|
GEMINATION/FUSIOn
|
|

Identify the dental abnormality:
|
CUSP OF CARABELLI
|
|
Identify the dental abnormality:
|
CUSP OF CARABELLI
|
|

Identify the dental abnormality:
|
TALON CUSPID
|
|
Identify the dental abnormality:
|
TALON CUSPID
|
|
Identify the dental abnormality:
|
TALON CUSPID
|
|

Identify the dental abnormality:
|
TALON CUSPID
|
|

Identify the dental abnormality:
|
TALON CUSPID
|
|

Identify the dental abnormality:
|
TALON CUSPID
|
|

Identify the dental abnormality:
|
DENS EVAGINATUS
|
|

Identify the dental abnormality:
|
DENS EVAGINATUS
|
|

Identify the dental abnormality:
|
DENS EVAGINATUS
|
|

Identify the dental abnormality:
|
DENS EVAGINATUS
|
|

Identify the dental abnormality:
|
DENS EVAGINATUS
|
|

Identify the dental abnormality:
|
DENS EVAGINATUS
|
|
Identify the dental abnormality:
|
DENS EVAGINATUS
|
|
Identify the dental abnormality:
|
DENS INVAGINATUS
|
|

Identify the dental abnormality:
|
DENS INVAGINATUS
|
|
Identify the dental abnormality:
|
DENS INVAGINATUS
|
|
Identify the dental abnormality:
|
ENAMEL PEARL
|
|
Identify the dental abnormality:
|
ENAMEL PEARL
|
|
Identify the dental abnormality:
|
TAURODONTISM
|
|

Identify the dental abnormality:
|
TAURODONTISM
|
|

Identify the dental abnormality:
|
TAURODONTISM
|
|

Identify the dental abnormality:
|
HYPERCEMENTOSIS
|
|

Identify the dental abnormality:
|
HYPERCEMENTOSIS
|
|

Identify the dental abnormality:
|
HYPERCEMENTOSIS
|
|

Identify the dental abnormality:
|
HYPERCEMENTOSIS
|
|

Identify the dental abnormality:
|
HYPERCEMENTOSIS
|
|

Identify the dental abnormality:
|
ROOT DILACERATION
|
|

Identify the dental abnormality:
|
ROOT DILACERATION
|
|

Identify the dental abnormality:
|
ROOT DILACERATION
|
|

Identify the dental abnormality:
|
ROOT DILACERATION
|
|

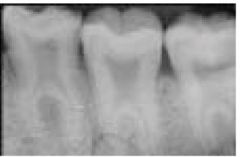
Identify the dental abnormality:
|
ATTRITION
|
|

Identify the dental abnormality:
|
ATTRITION
|
|

Identify the dental abnormality:
|
ATTRITION
|
|

Identify the dental abnormality:
|
ATTRITION
|
|

Identify the dental abnormality:
|
ATTRITION
|
|

Identify the dental abnormality:
|
ATTRITION
|
|
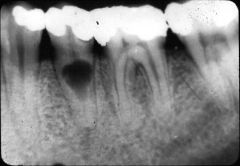
Identify the dental abnormality:
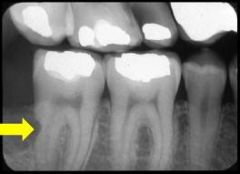
|
INTERNAL ROOT RESORPTION
|
|

Identify the dental abnormality:
|
INTERNAL ROOT RESORPTION
|
|

Identify the dental abnormality:
|
INTERNAL ROOT RESORPTION
|
|
Identify the dental abnormality:
|
INTERNAL ROOT RESORPTION
|
|

Identify the dental abnormality:
|
INTERNAL ROOT RESORPTION
|
|
Identify the dental abnormality:
|
EXTERNAL ROOT RESORPTION
|
|

Identify the dental abnormality:
|
EXTERNAL ROOT RESORPTION
|
|
|
Define PINK TOOTH OF MUMMERY:
|
Characteristic clinical appearance of INTERNAL RESORPTION when the coronal portion of the pulp is involved
|
|
|
Which is more common INTERNAL or EXTERNAL RESORPTION?
|
External is more common.
Internal is rare. |
|
|
EXTERNAL RESORPTION is accomplished by which cells?
|
Cells located on the PDL
|
|
|
What are a few potential etiologic factors of EXTERNAL RESORPTION?
|
- trauma
- pressure from tumor/cyst - adjacent tooth growth - mechanical forces (ortho) - inflammatory effects - idiopathic |
|
|
What are the two main patterns of EXTERNAL RESORPTION?
|
- resorption occurs immediately apical to CEJ on root surface
- Resorption starts at tooth apex and progress occlusally |
|
|
What is the treatment of EXTERNAL RESORPTION?
|
identifying and elimination of any accelerating factor.
Removal of all soft tissue from the sites of dental destruction |
|
|
Define HYPOPLASIA:
|
occurs in the form of pits, grooves, or large areas of missing enamel
|
|
|
Define DIFFUSE OPACITIES:
|
variations in translucency of enamel
|
|
|
Define DEMARCATED OPACITIES:
|
areas of decreased translucency increased opacity and sharp boudnary with adjacent enamel
|
|
|
Define TURNER'S HYPOPLASIA:
|
enamel defect seen in permanent teeth secondary to periapical inflammatory disease of the overlying deciduous tooth or trauma
|
|
|
TURNER'S HYPOPLASIA occurs more commonly in which teeth?
|
- premolars
- max. incisors |
|
|
Define DENTAL FLUOROSIS:
|
Ingestion of excess amounts of fluoride, usually in drinking water, can result in pitting in the enamel, or a "chalky" surface to the enamel. Presents bilaterally and with symmetric distribution
- PRIMARILY AESTHETIC |
|
|
What are the characteristic dental defects of SYPHILIS?
|
- Hutchinson's incisors (shaped like screwdrivers)
- Mulberry Molars (multiple tiny globues of enamel instead of cusps) |
|
|
Define "MATRIX FORMATION OF ENAMEL:
|
enamel proteins are laid down
|
|
|
Define MINERALIZATION OF ENAMEL:
|
minerals are deposited and most of the original proteins are removed
|
|
|
Define MATURATION OF ENAMEL:
|
final mineralization and the remnant of the original proteins are removed
|
|
|
Define AMELOGENESIS IMPERFECTA:
|
a group of inherited conditions affecting the enamel of teeth in absence of a systemic disorder. Genes that encode for ENAMEL proteins are mutated in patients with this condition.
|
|
|
To date, mutations of five genes have been associated with AMELOGENESIS IMPERFECTA, list them:
|
- AMELX
- ENAM - MMP-20 - KLK4 - DLX3 |
|
|
What are the 4 main types of AMELOGENESIS IMPERFECTA?
|
- HYPOPLASTIC
- HYPOCALCIFIED - HYPOMATURATION - HYPOPLASTIC-HYPOMATURATION |
|
|
What is another name for HYPOPLASTIC-HYPOMATURATION AMELOGENESIS IMPERFECTA?
|
AI with TAURODONTISM
|
|
|
Define HYPOPLASTIC AMELOGENESIS IMPERFECTA:
|
tooth enamel does not develop to a normal thickness because of failure of the ameloblasts to lay down enamel matrix properly
|
|
|
What is the radiographic appearance of HYPOPLASTIC AMELOGENESIS IMPERFECTA?
|
Abnormal enamel contrasts normally with dentin, thin peripheral outline of radiopaque enamel
|
|
|
Define HYPOCALCIFIED AMELOGENESIS IMPERFECTA:
|
quantity of enamel proteins is normal, but no significant mineralization occurs, therefore the enamel is very soft and easily lost
|
|
|
What are the radiographic features of HYPOCALCIFIED AMELOGENESIS IMPERFECTA?
|
- enamel has a moth eaten appearance and is LESS RADIOPAQUE than dentin
|
|
|
Define HYPOMATURATION AMELOGENESIS IMPERFECTA:
|
defect in the maturation of the enamel's crystal structure.
Enamel is of NORMAL THICKNESS but not of normal hardness and translucency |
|
|
What are the radiographic features of HYPOMATURATION AMELOGENESIS IMPERFECTA?
|
- radiodensity of enamel is almost equal to that of normal dentin
|
|
|
What is the mildest form of hypomaturation AI?
|
snow-capped teeth - where the enamel is of normal hardness and exhibits a white opaque zone on the incisal or occlusal one quarter to one third of the crown
|
|
|
Define HYPOPLASTIC-HYPOMATURATION AMELOGENESIS IMPERFECTA:
|
thin enamel is yellow to brown and pitted. Taurodont radiographic appearance.
|
|
|
What are the main problems experience in AMELOGENESIS IMPERFECTA patients?
|
- aesthetics
- dental sensitivity - loss of vertical dimension SOMETIMES: - anterior open bite - delayed eruption - tooth impaction |
|
|
DENTINOGENESIS IMPERFECTA is what kind of disorder?
|
Autosomal dominant
|
|
|
DENTINOGENESIS IMPERFECTA is associated with mutation of what gene?
|
DSPP (dentin sialophosphoprotein)
|
|
|
Which teeth are more severely affected in DENTINOGENESIS IMPERFECTA?
|
deciduous teeth are affected more severely followed by permanent incisors and first molars
|
|
|
What are the radiographic features of teeth in DENTINOGENESIS IMPERFECTA?
|
- bulbous crowns
- cervical constrictions - thin roots - early obliteration of the root canals and pulp chambers |
|
|
Define DENTIN DYSPLASIA:
|
- autosomal dominant inherited disorder that affects dentin
|
|
|
What are the two main types of DENTIN DYSPLASIA?
|
TYPE 1: Radicular DD
TYPE2: Coronal DD |
|
|
Define DENTIN DYSPLASIA TYPE I:
|
RADICULAR TYPE
(rootless teeth) The enamel and coronal dentin are normal clinically and well formed, but radicular dentin loses all organization and subsequently is shortened dramatically Pulp is often OBLITERATED but may show crescent or chevron-shaped pulp chamber |
|
|
CRESCENT or CHEVRON-SHAPED PULP CHAMBER is seen in what condition?
|
DD TYPE I: Radicular
|
|
|
DD TYPE II (CORONAL) is associated with mutation in what gene?
|
DSPP
|
|
|
Define DD TYPE II:
|
Coronal type of DENTIN DYSPLASIA.
Deciduous teeth closely resemble that of DENTINOGENESIS IMPERFECTA. Bulbous crowns, cervical constrictions, thin roots, early obliteration of pulp. |
|
|
What are the radiographic features in permanent teeth of DD TYPE II: CORONAL?
|
- clinical coloration
- coronal pulps are enlarged with apical extension of the pulp chamber "thistle tube shaped / flame-shaped" - pulp stones - root lengths normal - narrow pulp canals |
|
|
What is the treatment modality for each type of DENTIN DYSPLASIA?
|
TYPE I: Retention of teeth as long as possible, no good prognosis
TYPE II: Retention of teeth as long as possible, meticulous oral hygeine, better prognosis |
|
|
Define REGIONAL ODONTODYSPLASIA (ghost teeth):
|
uncommon localized developmental abnormality of severe adjacent teeth in which the enamel, dentin and pulp tissue are affected. Idiopathic mostly. Alteration in vascular supply.
|
|
|
What are the clinical features of GHOST TEETH?
|
- teeth fail to erupt
- small yellow to brown crowns with rough surfaces - caries and periapical lesions common |
|
|
What are the radiographic features of GHOST TEETH?
|
- faint outlines of teeth
- large pulp chambers - short roots |
|
|
What are the most common presenting signs of GHOST TEETH?
|
- delayed / failure of eruption
- early exfoliation / abcess formation - malformed teeth - non-inflammatory gingival enlargement |
|

Identify the dental abnormality:
|
PINK TOOTH OF MUMMERY
|
|

Identify the dental abnormality:
|
PINK TOOTH OF MUMMERY
|
|

Identify the dental abnormality:
|
PINK TOOTH OF MUMMERY
|
|

Identify the dental abnormality:
|
PINK TOOTH OF MUMMERY
|
|

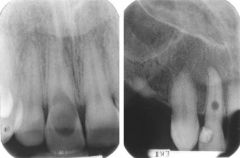
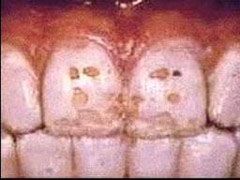
Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|

Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|

Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|

Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|

Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|

Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|

Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|
Identify the dental abnormality:
|
TURNER'S HYPOPLASIA
|
|

Identify the dental abnormality:
|
MULBERRY MOLAR
|
|

Identify the dental abnormality:
|
MULBERRY MOLAR
|
|

Identify the dental abnormality:
|
MULBERRY MOLAR
|
|

Identify the dental abnormality:
|
HUTCHINSON's INCISORS
|
|

Identify the dental abnormality:
|
HUTCHINSON's INCISORS
|
|

Identify the dental abnormality:
|
HUTCHINSON's INCISORS
|
|
Identify the dental abnormality:
|
HUTCHINSON's INCISORS
|
|

Identify the dental abnormality:
|
DENTAL FLUOROSIS
|
|

Identify the dental abnormality:
|
DENTAL FLUOROSIS
|
|

Identify the dental abnormality:
|
DENTAL FLUOROSIS
|
|

Identify the dental abnormality:
|
DENTAL FLUOROSIS
|
|

Identify the dental abnormality:
|
DENTAL FLUOROSIS
|
|

Identify the dental abnormality:
|
AMELOGENESIS IMPERFECTA
|
|

Identify the dental abnormality:
|
AMELOGENESIS IMPERFECTA
|
|

Identify the dental abnormality:
|
AMELOGENESIS IMPERFECTA
|
|

Identify the dental abnormality:
|
AMELOGENESIS IMPERFECTA
|
|

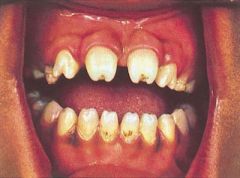
Identify the dental abnormality:
|
DENTINOGENESIS IMPERFECTA
|
|

Identify the dental abnormality:
|
DENTINOGENESIS IMPERFECTA
|
|

Identify the dental abnormality:
|
DENTINOGENESIS IMPERFECTA
|
|

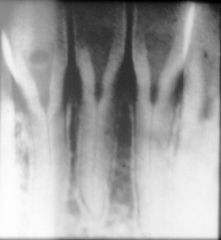
Identify the dental abnormality:
|
DENTIN DYSPLASIA TYPE I
|
|

Identify the dental abnormality:
|
DENTIN DYSPLASIA TYPE I
|
|
Identify the dental abnormality:
|
DENTIN DYSPLASIA TYPE II
|
|

Identify the dental abnormality:
|
DENTIN DYSPLASIA TYPE II
|
|
Identify the dental abnormality:
|
DENTIN DYSPLASIA TYPE II
|
|

Identify the dental abnormality:
|
REGIONAL ODONTODYSPLASIA "ghost teeth"
|
|

Identify the dental abnormality:
|
REGIONAL ODONTODYSPLASIA "ghost teeth"
|
|
Identify the dental abnormality:
|
REGIONAL ODONTODYSPLASIA "ghost teeth"
|
|

Identify the dental abnormality:
|
REGIONAL ODONTODYSPLASIA "ghost teeth"
|