![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back
|
What is the main pathogenesis pattern of Sjögren Syndrome?
Main population affected? |
Lymphocyte infiltration and fibrosis of salivary and lacrimal glands mainly by CD4+ cells, some infiltration by B cells and plasma cells.
Females 35-45 (90%)
|
|
|
Antibody involvement with Sjögren?
Eliciting factors? |
No direct evidence for antibody involvement or which antigen(s) elicit Sjögren Syndrome.
Potential role for alpha-fodrin autoantigen or retrovirus infection for initiating events. |
|
|
Chief symptoms include _____ of eyes and mouth. Eyes tested with _______'s Test. |
dryness (keratoconjunctivitis and xerostomia); Schirmer's Test |
|
|
Extra-glandular symptoms include (3): |
1) pulmonary fibrosis (30-40% of patients, can progress to complete respiratory failure) 2) synovitis 3) peripheral neuropathy |
|
|
Is Sjögren Syndrome associated with malignancy? |
Yes: Follicular B cell hypertrophy leads to lymphadenopathy and 40x risk for malignant lymphoma
Better recognize niggas. |
|
|
Most specific antibodies for Sjögren Syndrome?
High ____ associated with ________. |
SSA (Ro) and SSB (La) - elevated in 90% of Sjögren patients
High SSA (Ro) levels more likely to exhibit extraglandular disease. enG |
|
|
RF levels in Sjögren Syndrome: |
Elevated in 75% Sjögren patients (in absence of RA) |
|
|
ANA levels and immunofluorescence pattern? |
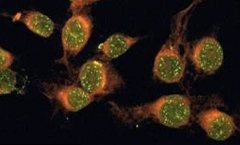
Elevated in 50-80% of Sjögren patients overall.
Speckled Pattern specific for Sjögren Syndrome. |
|
|
Part of glands affected first by lymphocyte infiltration? |
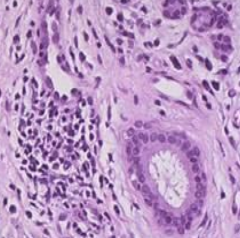
Acini obliterated before more sturdy ducts |
|
|
HLA alleles associated with Sjögren Syndrome (3): |
B8, DR3 and DRW52 |
|
|
Main pathogenesis pattern for scleroderma (systemic sclerosis)? |
Excessive fibrosis throughout the body - skin especially, then GI, kidneys, heart, muscles, lungs. |
|
|
Cells and factors involved with epithelial scleroderma pathogenesis: |
Antigen-activated CD4+ T cells induce inflammatory cells recruitment and release of inflammatory cytokines (IL-4, IL-13, PDGF, TGF-B) that stimulate myofibroblasts and lead to excessive collagen deposition. |
|
|
Cells and factors associated with endothelial scleroderma pathogenesis: |
Endothelin: endothelial injury associated with irreversible intimal fibrosis and platelet activation that can lead to ischemia |
|
|
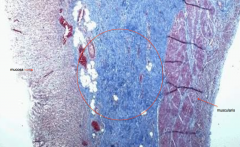
Skin-related symptoms of scleroderma: |
- Sclerotic atrophy of skin beginning distally
- Thickening/occlusion of small vessels can lead to ischemia
- Loss of rete pegs/dermal appendages can lead to ulcers
|
|
|
Chief histologic dermal findings with scleroderma (3): |
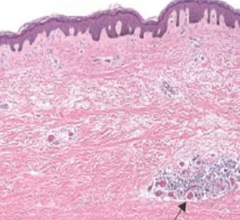
- dense collagen deposition in dermis - eccrine sweat gland degeneration - hair follicles missing (only arrector pili muscles left behind)
|
|
|
Most common extra-dermal finding of scleroderma is? |
GI/Esophagus (90%) - Collagen deposition at the esophagus that disrupts the muscularis --> GERD and Barrett's Esophagus - Loss of villi in small bowel --> malabsorption |
|
|
Fibrosis in small vessels of the ______ can lead to hypertension and _____ failure |
Kidney involvement for 2/3 of patients: - Hypertension (30%) - Renal failure (50% deaths) |
|
|
The most common causes of morbidity/mortality in scleroderma are: |
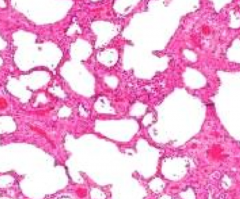
Pulmonary HTN and pulmonary fibrosis |
|
|
Heart symptoms associated with scleroderma (2): |
More fibrosis - myocarditis and myocardial fibrosis |
|
|
Diffuse scleroderma characteristics: |

- Affects all skin - Nucleolar ANA pattern - Anti-DNA topoisomerase 1 (Scl-70) in 28-70% of patients |
|
|
Limited scleroderma characteristics: |
- Only affects skin at distal limbs (acral skin) - Does not affect skin at trunk or proximal limbs - Ant-centromere ANA - Extracutaneous CREST symptoms |
|
|
What does CREST stand for? |
- Calcinosis - Raynaud's - Esophageal dysmotility - Sclerodactyly - Telengectasia
O'Hara says Calcinosis not an associated finding anymore, internet says otherwise. God FTW |
|
|
Basic pathogenesis pattern of Rheumatoid Arthritis (RA): |
Chronic inflammatory autoimmune disorder that attacks joints, can lead to destroyed articular cartilage and ankylosis |
|
|
Chief factor elevated in 80% of those with RA? Role in pathogenesis? |
Rheumatoid factor (RF) = anti-IgG IgM
Circulating IgG-IgM complexes that deposit in vessels though to to contribute to extra-articular symptoms.
Not 100% responsible for symptoms - found in healthy people and not found in some with RA |
|
|
T cell type related to RA? Cells and enzymes they acticvate? |
CD4+ T cells
Activate endothelial cells to express adhesion molecules
Activates collagenase, elastase, stromelysin, PGE2 and other enzymes that help break down joint tissue |
|
|
Result of immune complex deposition and CD4+ T cell activation = |
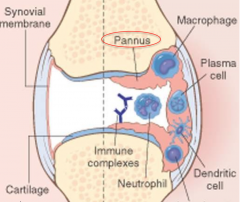
Pannus: tumor-like mass of granulation tissue that destroys articular cartilage and bone. Can lead to ankylosis |
|
|
Primary joint affected by RA? Spared joints? |
Primarily affects small joints - MCP, PIP, wrist, ankles, elbows
Large joints usually spared |
|
|
______ deviation of the wrist and ______ deviation of the phalangeal joints is a sign of progressed RA |
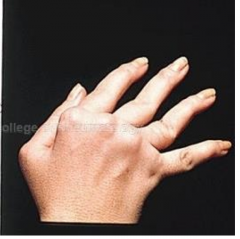
Radial deviation of the wrist, ulnar deviation of the phalangeal joints |
|
|
Effects at synovium with RA due to CD4+, macrophage and plasma cell infiltration (5): |
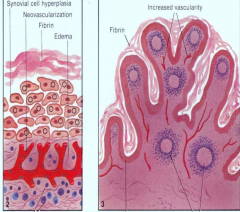
- synovial hyperplasia - edema - synovial membrane thickening - increase vascularity - fibrin deposition |
|
|
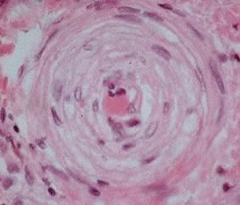
Fibrinoid necrosis of collagen surrounded by inflammatory cells =
|
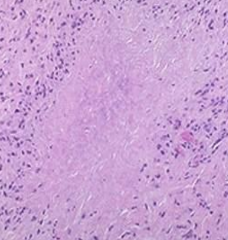
Rheumatoid nodules
Can be found at skin (usually extensor surfaces) or lung, heart, spleen |
|
|
Name 3 organ specific autoimmune diseases: |
1) Hasimoto's thyroiditis 2) Atrophic gastritis 3) Hemolytic anemia
All directed against one tissue |
|
|
4 examples of systemic auto-immune diseases: |
1) SLE 2) RA 3) Scleroderma 4) Sjögren Syndrome |
|
|
Indirect immunofluorescence test technique |
Introduce anti-IgG antibodies with fluorescent component after permeabilizing cell membrane and nuclear membrane |
|
|
Auto-antibodies and ANA pattern for SLE |
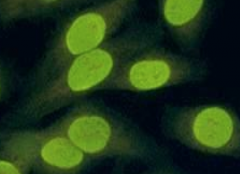
- anti-dsDNA and anti-Sm antigen - homogenous ANA pattern |
|
|
Auto-antibodies and ANA pattern for Sjögren Syndrome |
- SSA (Ro) an SSB (La) anti-RNPs - Speckled ANA pattern |
|
|
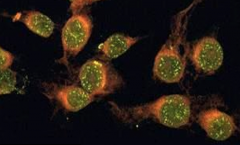
Auto-antibodies and ANA pattern for scleroderma |
- anti-DNA topoisomerase 1 (Scl-70) - Nucleolar ANA pattern (most sensitive of the ANA patterns) |