Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
What is the microscopic anatomy of the liver
|

Microscopic anatomy of the liver. The portal tract carries branches of the portal vein, hepatic artery, and bile duct system. The portal vein gives rise to branching septal veins, which penetrate the hepatocellular parenchyma at regular intervals. Blood from the septal veins enters directly into the parenchymal sinusoids between hepatocytes. The hepatic artery gives off capillaries that supply the bile duct system; these capillaries usually dump into the portal vein but may deposit blood directly into sinusoids. Arterioles also occasionally convey blood directly to the sinusoids. The bile duct system gives off bile ductules, which traverse the mesenchyme of the portal tract to penetrate the parenchyma; at that point, they become hemicircular, abutting hepatocytes (not shown) to form the canals of Hering. Bile traveling through the bile canalicular system between hepatocytes enters into the biliary tree through these canals of Hering. Blood from the portal vein and hepatic artery travels through the sinusoids of the parenchyma toward the terminal hepatic vein, leaving the liver by this route. On the basis of blood flow, three zones can be defined, zone 1 being the closest to the blood supply and zone 3 being the farthest. Pathologists refer to the regions of the parenchyma as "periportal, midzonal, and centrilobular," the last term owing to the historical concept that the terminal hepatic vein was at the center of a "lobule."
|
|

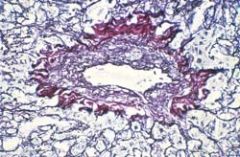
What does this picture represent
|

Photomicrograph of liver (trichrome stain). Note the blood-filled sinusoids and cords of hepatocytes; the delicate network of reticulin fibers in the subendothelial space of Disse stains light blue
|
|
|
What are the major clinical consequences of portal hypertension
|

The major clinical consequences of portal hypertension in the setting of cirrhosis, shown for the male. In women, oligomenorrhea, amenorrhea, and sterility are frequent, owing to hypogonadism
|
|
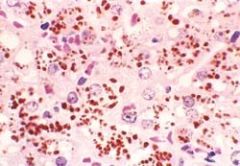
What does this picture demonstrate
|
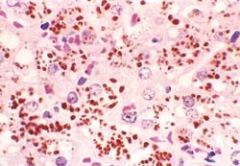
Dubin-Johnson syndrome, showing abundant pigment inclusions in otherwise normal hepatocytes (H&E).
|
|
|
What is the sequence of serologic markers in acute Hep A
|

Sequence of serologic markers in acute hepatitis A viral hepatitis.
|
|
|
What are the morphologic features of both acute and chronic hepatitis
|

Diagrammatic representations of the morphologic features of acute and chronic hepatitis. Bridging necrosis (and fibrosis) is shown only for chronic hepatitis; bridging necrosis may also occur in acute hepatitis (not shown).
|
|

What do these pictures demonstrate
|

Hepatitis B viral infection. A, Liver parenchyma showing hepatocytes with diffuse granular cytoplasm, so-called ground glass hepatocytes. (H&E) B, Immunoperoxidase stain for HBsAg from the same case, showing cytoplasmic inclusions of viral particles.
|
|

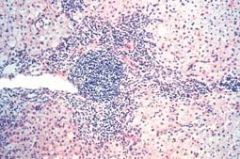
What does this picture demonstrate
|

Acute viral hepatitis showing disruption of lobular architecture, inflammatory cells in the sinusoids, and hepatocellular apoptosis
|
|
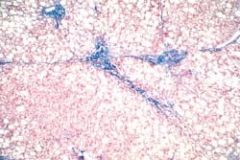
What does this picture demonstrate
|

Chronic viral hepatitis due to hepatitis C virus, showing portal tract expansion with inflammatory cells and fibrous tissue and interface hepatitis with spillover of inflammation into the adjacent parenchyma. A lymphoid aggregate is present
|
|

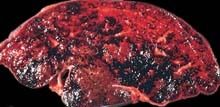
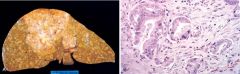
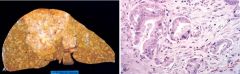
What does this picture demonstrate
|

Cirrhosis resulting from chronic viral hepatitis. Note the broad scar and coarse nodular surface
|
|

What does this picture demonstrate
|

Massive necrosis. A, Cut section of liver. The liver is small (700 gm), bile-stained, and soft. The capsule is wrinkled. B, Microscopic section. Portal tracts and terminal hepatic veins are closer together than normal, owing to necrosis and collapse of the intervening parenchyma. The rudimentary ductal structures are the result of early ductular regeneration. An infiltrate of mononuclear inflammatory cells is present
|
|
What does this picture demonstrate
|

Alcoholic liver disease: macrovesicular steatosis, involving most regions of the hepatic lobule. The intracytoplasmic fat is seen as clear vacuoles. Some early fibrosis (stained blue) is present (Masson trichrome).
|
|

What are the different courses in alcoholic liver disease
|
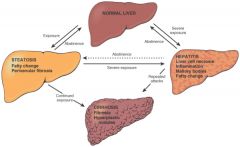
Alcoholic liver disease. The interrelationships among hepatic steatosis, hepatitis, and cirrhosis are shown, along with a depiction of key morphologic features at the morphologic level.
|
|

What does this picture demonstrate
|

Alcoholic hepatitis. A, The cluster of inflammatory cells marks the site of a necrotic hepatocyte. A Mallory body is present in a second hepatocyte (arrow). B, Eosinophilic Mallory bodies are seen in hepatocytes, which are surrounded by fibrous tissue (H&E
|
|

What do these pictures demonstrate
|

Alcoholic cirrhosis. A, The characteristic diffuse nodularity of the surface reflects the interplay between nodular regeneration and scarring. The greenish tint of some nodules is due to bile stasis. A hepatocellular carcinoma is present as a budding mass at the lower edge of the right lobe (lower left of figure). B, The microscopic view shows nodules of varying sizes entrapped in blue-staining fibrous tissue. The liver capsule is at the top (Masson trichrome).
|
|
|
What is the function of HFE in the intestine
|

Schematic diagram of HFE function in the intestine. The crypt epithelial cell expresses HFE on its basolateral surface; complexing of HFE with β2-microglobulin is required for its expression on the cell surface. HFE-β2-microglobulin complexes with the transferrin receptor (TfR) to bind circulating transferring (Tf). Endocytosis ensues; on acidification of the recycling endosome, transferrin-bound iron (Fe(II)) is released and enters into the cytoplasm. High levels of cytoplasmic iron downregulate levels of the iron-regulatory proteins (IRP), a family of proteins with potent effects on nuclear transcription. With low levels of cytoplasmic iron, the IRP content of the cell remains high. IRPs upregulate nuclear transcription of the genes for several proteins required for intestinal absorption of dietary iron: Dcytb (duodenal cytochrome B), DMT1 (divalent metal transporter 1), ferritin (a cytoplasmic iron-binding protein), and FP1 (ferroportin 1). A mutation in HFE prevents "sensing" of circulating iron levels by the crypt epithelial cell, leading to unregulated expression of these four proteins. The crypt epithelial cell is the precursor cell of the mature absorptive enterocyte on the tip of the villus, through migration up the villus axis. On the apical membrane of the absorptive enterocyte, Dcytb reduces dietary ferric iron (Fe(III)) to ferrous iron (Fe(II)). Fe(II) is then taken up by DMT1 into the enterocyte. Iron can be bound to ferritin (and hence sloughed back into the gut lumen) or transported across the basolateral plasma membrane by FP1 for binding to transferrin and entry into the systemic circulation. In the patient with mutant HFE, the inability to downregulate expression of these four proteins leads to lifelong excessive absorption of dietary iron.
|
|
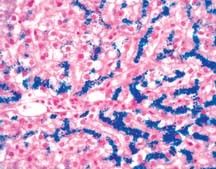
What does this picture demonstrate
|
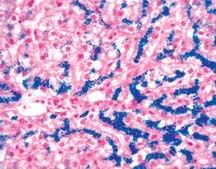
Hereditary hemochromatosis. Hepatocellular iron deposition is blue in this Prussian blue-stained section of an early stage of the disease, in which parenchymal architecture is normal
|
|

What does this picture represent
|

α1-Antitrypsin deficiency. Periodic acid-Schiff stain of the liver, highlighting the characteristic red cytoplasmic granules
|
|

What does this picture represent
|

Biliary cirrhosis. Sagittal section through the liver demonstrates the fine nodularity and bile staining of end-stage biliary cirrhosis
|
|

What does this picture demonstrate
|

Primary biliary cirrhosis. A portal tract is markedly expanded by an infiltrate of lymphocytes and plasma cells. The granulomatous reaction to a bile duct undergoing destruction (florid duct lesion) is highlighted by the arrowheads
|
|

What does this picture demonstrate
|

Primary sclerosing cholangitis. A bile duct under-going degeneration is entrapped in a dense, "onion-skin" concentric scar.
|
|
|
What are the common bile duct anomalies
|

Bile duct anomalies. The morphologic features of the four major groups are diagrammed, along with apparent patterns of inheritance and associations with polycystic kidney disease. PV, portal vein. HA, hepatic artery.
|
|
|
What are the common manifestations of hepatic circulatory disorders
|

Hepatic circulatory disorders. The forms and clinical manifestations of impaired blood flow are contrasted.
|
|

What does this picture demonstrate
|

Liver infarct. A thrombus is lodged in a peripheral branch of the hepatic artery and compresses the adjacent portal vein; the distal hepatic tissue is pale, with a hemorrhagic margin.
|
|

What does this picture demonstrate
|

Centrolobular hemorrhagic necrosis. The cut liver section, in which major blood vessels are visible, is notable for a variegated, mottled, red appearance (nutmeg liver).
|
|

What does this picture demonstrate
|
Budd-Chiari syndrome. Thrombosis of the major hepatic veins has caused extreme blood retention in the liver
|
|
What does this picture demonstrate
|

Veno-occlusive disease. A reticulin stain reveals the parenchyma framework of the lobule and the marked deposition of collagen within the lumen of the central vein.
|
|

What does this picture demonstrate
|

Eclampsia. Subcapsular hematoma dissecting under Glisson's capsule in a fatal case of eclampsia.
|
|

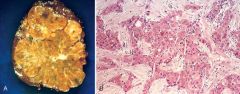
What do these pictures demonstrate
|

Focal nodular hyperplasia. A, Resected specimen showing lobulated contours and a central stellate scar. B, Low-power photomicrograph showing a broad fibrous scar with hepatic arterial and bile duct elements and chronic inflammation, present within hepatic parenchyma that lacks the normal sinusoidal plate architecture (H&E).
|
|

What does this picture demonstrate
|

Nodular regenerative hyperplasia. Autopsied liver showing diffuse nodular transformation
|
|

What do these pictures demonstrate
|
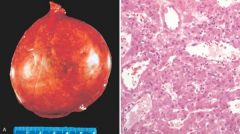
Liver cell adenoma. A, Resected specimen presenting as a pendulous mass arising from the liver. B, Microscopic view showing cords of hepatocytes, with an arterial vascular supply and no portal tracts
|
|

What do these pictures demonstrate
|

Liver cell adenoma. A, Resected specimen presenting as a pendulous mass arising from the liver. B, Microscopic view showing cords of hepatocytes, with an arterial vascular supply and no portal tracts
|
|

What do these pictures demonstrate
|

Hepatocellular carcinoma. A, Autopsied liver showing a unifocal, massive neoplasm replacing most of the right hepatic lobe in a noncirrhotic liver; a satellite tumor nodule is directly adjacent. B, In this microscopic view of a well-differentiated lesion, tumor cells are arranged in nests, sometimes with a central lumen, one of which contains bile (arrow). Other tumor cells contain intracellular bile pigment.
|
|
What do these pictures demonstrate
|

Fibrolamellar carcinoma. A, Resected specimen showing a demarcated nodule in an otherwise normal liver. B, Microscopic view showing nests and cords of malignant-appearing hepatocytes separated by dense bundles of collagen
|
|
What do these pictures demonstrate
|
Cholangiocarcinoma. A, Autopsied liver showing a massive neoplasm in the right hepatic lobe and innumerable metastases permeating the entire liver. B, Microscopic view showing tubular glandular structures embedded in a dense sclerotic stroma
|
|

What does this picture demonstrate
|

Multiple hepatic metastases from a primary colon adenocarcinoma
|
|

What does this picture represent
|

Normal gallbladder histology. The undulating mucosal epithelium overlies a delicate lamina and only one smooth muscle layer. This is different from elsewhere in the gut, where two muscle layers exist (muscularis mucosa and muscularis propria).
|
|

What does this picture demonstrate
|

Phrygian cap of the gallbladder; the fundus is folded inward.
|
|
|
What are the four contributing factor for cholelithiasis
|

Schematic representation of the four contributing factors for cholelithiasis: supersaturation, gallbladder hypomotility, crystal nucleation, and accretion within the gallbladder mucous layer
|
|

What does this picture demonstrate
|

Cholesterol gallstones. Mechanical manipulation during laparoscopic cholecystectomy has caused fragmentation of several cholesterol gallstones, revealing interiors that are pigmented because of entrapped bile pigments. The gallbladder mucosa is reddened and irregular as a result of coexistent chronic cholecystitis
|
|

What does this picture demonstrate
|

Pigment gallstones. Several faceted black gallstones are present in this otherwise unremarkable gallbladder from a patient with a mechanical mitral valve prosthesis, leading to chronic intravascular hemolysis
|
|

What does this picture demonstrate
|

Acute calculous cholecystitis; the stone was not photographed
|
|

What does this picture demonstrate
|

Chronic cholecystitis with cholesterol stones. The gallbladder wall is thickened and gray-white, owing to fibrosis and inflammation. The mucosa is effaced. Multiple faceted cholesterol gallstones are present within the lumen. The exterior of the specimen is black as a result of India ink application.
|
|

What do these pictures demonstrate
|

Gallbladder adenocarcinoma. A, The opened gallbladder contains a large, exophytic tumor that virtually fills the lumen. B, Malignant glandular structures are present within a densely fibrotic gallbladder wall.
|