![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
321 Cards in this Set
- Front
- Back
|
What is haemostasis? |
Haemostasis is the mechanisms in place to preventor minimise haemorrhage
|
|
|
What are the 3 components of haemostasis? |
§Formation of the blood clot (coagulation)
§Removal of a clot once the tissue has repaired(fibrinolysis) §Prevention of clotting in normal vessels |
|
|
Describe primary haemostasis |
• Platelet plug formation - Vasoconstriction – reduce blood flow to haemorrhage - Platelet adhesion- platelets stick to exposed collagen – mediated by Von Willebran’s Factor - Platelet aggregation - Platelet contraction |
|
|
Describe secondary haemostasis |
Secondary haemostasis
• Stabilisation of platelet plug with fibrin - Triggered when factor XII contacts collagen or when Factor III is spilled out of damaged cells |
|
|
What is the role of calcium and vitamin K in haemostasis? |
Calcium acts as a bridge between factors (NB: some anticoagulants are calcium chelators) Vitamin K is required to activate factors II, VII, IX and X |
|
|
Describe fibrinolysis |
o The breakdown of fibrin clots
o Plasminogen activated into plasmin by many enzymes when it binds to clots o Plasmin breaks down fibrin and fibrinogen It cleaves these into smaller products known as fibrin degradation products (FDP) |
|
|
What is the difference between disorders of primary haemostasis and disorders in secondary haemostasis? |
Disorders of primary haemostasis involvesomething going wrong with the platelet plug (primary haemostasis), secondaryhaemostasis disorders are when something goes wrong with the stabilisation of aplatelet plug with fibrin (secondary haemostasis)
|
|
|
What clinical signs and clinical pathology abnormalities would you see with a disorder in primary haemostasis? |
Clinical signs · Ecchymoses (discolouration of the skin resultingfrom bleeding underneath) or petechiae (a small dot of haemorrhage) · Commonly see epistaxis (nose bleeds),haematochezia (blood in solid poos), haematuria or melaena · Prolonged bleeding post-surgery · Affects multiple sites Abnormal Clinical Pathology • Prolonged BMBT • Normal PT, ACT/APTT • See decreased platelets (only if its thrombocytopenia and not thrombocytopathy)• Decreased vWF if its Von Willebrans Fatcor defect |
|
|
What does TT assess and what can a prolonged one indicate? |
It assesses conversion of fibrinogen to fibrin. A prolonged one can indicate DIC |
|
|
What is BMBT and what is its normal range in a dog? What can a prolonged one indicate? |
Buccal mucosal bleeding time. Assesses platelet function and the amount of vonWillebran’s factor. Normal range in a dog is 2-3mins. A prolonged one can indicate a disorder in primary haemostasis (like thrombocytopenia, Erlichiosis, thrombocytopathies or von Willebrans defect) |
|
|
What can cause Disseminated Intravascular Coagulopathy (DIC)? |
Toxicities e.g. rat bait
Bacterial sepsis (most common cause) Pancreatitis Heat stroke Shock IMHA GDV Snake bite Hemangiosarcoma |
|
|
Describe the pathogenesis of DIC |
§Endothelial damage means there is widespread release of tissue factor (which activates the extrinsic pathway of haemostasis)/ increased pro-coagulant proteins
§Multiple fibrin clots then form within arterioles and capillaries causing ischaemia and necrosis §Then fibrinolysis is activated, resulting in the formation of plasmin and large-scale production of FDPs – inhibits coagulation §Patients will be hyper or hypo-caogulable depending on the balance of anti and pro-coagulants |
|
|
What CBC and coagulation profile abnormalities would you expect in a patient with DIC? What further test could you do to support a diagnosis of DIC? |
§CBC and coagulation profile
· Schistocytes · Thrombocytopenia · Decreased fibrinogen (not in chronic form) · Prolonged APTT, PT and TT · Increased FDPs (not in chronic form) · Decreased ATIII You could perform a D-dimer test. This measures a specific FDP and it will be increased in patients with DIC. |
|
|
What are the two main categories of thrombocytopenia? |
Pseudothrombocytopenia (not actually due to a pathological process) and true thrombocytopenia (true pathological process) |
|
|
What can cause pseudothrombocytopenia |
· Platelet clumping: the machine doesn’t recognise clumped platelets as platelets and so you get a falsely low reading
· CKC spaniels often have macroplatelets which also don’t get recognised as platelets · Greyhounds and Shiba Inus have naturally lower platelet counts |
|
|
What can cause true thrombocytopenia? |
Decreased production of platelets can cause it
• This can happen if there is an infectious agent causing it, suppression of the bone marrow (oestrogen induced or from chemotherapy) • Myelophthisis Increased destruction of platelets is another cause • Primary immune mediated thrombocytopenia: Antibodies produced against own platelets • It can also occur secondary to an underlying condition (SLE, neoplasia or vaccine/drug induced) • Sequestration of platelets is also a cause: usually its only a mild decrease (happens with splenic congestion) • Increased consumption is another cause: happens when there is severe haemorrhage or DIC |
|
|
Give examples of acquired and congenital coagulation factor defects |
Congenital= Haemophilia Acquired= vitamin K antagonism (e.g. rat bait toxicity) - vitamin K reactivation (vitamin K recycling) is inhibited |
|
|
What factors affect the severity of rat bait poisoning in dogs? |
o High fat diets
§Facilitate absorption of rat bait §Decreased protein binding and thus increasesplasma concentration of rat bait o Some drugs §Displace rat bait bound to albumin §Increases free active form §E.g. sulphonamides and antifungals o NSAIDs, ACP, C/S and adrenaline §Liver disease · Gonna run out of active vit K sooner – so animalbleeds to death sooner after consumption of rat bait |
|
|
What are the components of a CNS post-mortem exam? |
o We examine the CNS in cases of neurologicaldisease or cases where no other lesions are apparent in the other major organso Whenever there is a history of paralysis andparesis, the spinal cord should be examined o You need to take representative samples frommultiple anatomic locations if the lesion location has been identified. If thelesion location has been identified, then the CNS examination can be concentratedon a specific location
o Brain examination § Cerebellar and cerebrum size § Evidence of · Malformation · Swelling · Dissymmetry · Cerebellar coning · Meningeal opacity § A similar examination should be done for thespinal cord o Always wear protective gear when handling rabiessuspects and suspects with potential zoonotic diseases o For routine examination, fixation of the brainand spinal cord in 10:1, 10% formalin solution is best (lasts 5-10 days) |
|
|
Define Anencephaly |
absenceof the brain. Arrest closure of the rostral portion of the neural tube (thecranium failed to develop) – the terms Aplasia and Proencephalic hypoplasia aremore accurate if the medulla or remnants of the mesencephalon are present"
|
|
|
Define Hydranencephaly |
Abnormallarge fluid filled cavities form in the CNS
|
|
|
Define Porencephaly |
Abnormal small fluid filled cavities form in the CNS
|
|
|
Define Cyclopia |
Partial fusion of the orbits so there appears to be a single eye
|
|
|
Define Encephalocele |
Protrusion of the brain through a defect in the cranium
If only the meninges protrude, it is called Meningocele |
|
|
Define Lisencephaly (Agyria) |
Convolutions (gyri and sulci) are almost entirely absent from the brain – smooth brain
|
|
|
Define Hydrocephalus |
Abnormal accumulation of CSF in the cranial cavity
|
|
|
Define Dysraphism |
a broad term given to a group of congenital spine abnormalities that result from defective closure of the neural tube
|
|
|
Define Spina Bifida |
Dorsal defect in the closure of 1 to several vertebral arches that form the spinal column. May result in the herniation of the meninges (and maybe spinal cord).
|
|
|
Define Hydromyelia |
Abnormal dilatation of the central spinal cord |
|
|
Define Syringomyelia |
tubular cavitation of the spinal cord that extends over several segments |
|
|
Define Encephalitis |
Inflammation of the brain |
|
|
Define Myelitis |
Inflammation of the spinal cord |
|
|
Define encephalomyelitis |
Inflammationof the brain and spinal cord |
|
|
Define Ependymitis |
Inflammationof the ependymal cells (a type of glial cell) |
|
|
Define Choroiditis |
Inflammationof the choroid plexus |
|
|
Define Meningitis |
Inflammationof the meninges |
|
|
What are the 2 main categories of meningitis? |
Leptomeningitis: Inflammation of the pia-arachnoid
Pachymeningitis: Inflammation of the dura mater |
|
|
Define malacia |
Softening/necrosisof the tissue in the CNS
|
|
|
Define poliomalacia |
Softening of the grey matter
|
|
|
Define Leukomalacia |
Softening of the white matter
|
|
|
What cells in the CNS are most susceptible to injury? |
Neurons (neurons> oligodendroglia > astrocytes > microglia > blood vessels |
|
|
How do nerve fibres heal? |
By repair (fibrosis) o Nerve fibres in the CNS have little to no regenerative capacity o Nerve fibres in the PNS can regenerate under certain circumstances |
|
|
Explain the difference between the healing of wounds deep within the CNS and superficial CNS wounds |
o Wounds deep in the CNS heal by proliferation of astrocytes’ processes
o Superficial wounds or wounds that extend throughout the meninges, heal by deposition of collagen by fibroblasts |
|
|
What is Wallerian degeneration |
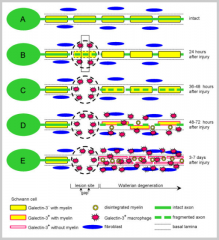
o Axonal degeneration with secondary myelin losso This occurs when there is injury to axons
o Wallerian degeneration occurs to the axons distal to the point of injury |
|
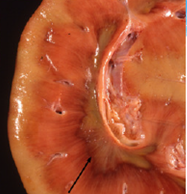
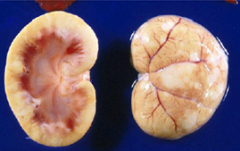
What is wrong with the dog brain on the top? |
Cerebellar Hypoplasia |
|
|
What animal's are predisposed to inter-vertebral disc disease? |
Dogs (rarely cats) Occurs as an ageing change in non-chondrodystrophic dogs Occurs in young dogs of chondrodystrophic breeds |
|
|
What is the pathogenesis of cervical stenotic myelopathy |
Causedby narrowing of the cervical vertebral canal and the resultant compression ofthe spinal cord, often in combination with malalignment and malformation of thecervical vertebrae
|
|
|
What CNS lesions may be present on PM in ruminants with Leptospirosis? |
o Encephalitis of the brainstem
o Lesions most severe in the medulla and pons dueto the bacteria having an affinity for there o Multifocal microabscesses and usually someleptomeningitis – characteristic histological lesions |
|
|
What can cause polioencephalomalacia in ruminants? |
Thiamine deficiency is the most common cause (thiamine is usually produced by rumen microflora)- happens when there is a change in diet causing a change in microflora (↑concentrates, ↓fibre)
Excess dietary sulphur, sulphates and sulphites may also induce PEM in ruminants (by inducing change in thiamine metabolism and by decreasing ATP and leading to cytotoxic oedema) |
|
|
What clinical signs may be present in animal's with lead toxicity? |
o In acute cases, calves stagger, develop muscletremors and are recumbent. In less severe cases there may be drooling, grindingof teeth, dullness, immobility and hyperesthesia
o In subacute cases, there may be laminar corticalnecrosis |
|
|
What cells in the CNS do equine encephalitis viruses replicate in? |
Neurons, Glial cells and blood vessels (so all of them) |
|
|
What does West Nile Encephalomyelitis cause? |
§ Inflammation of the grey matter of the spinalcord and brain
§ Gliosis – change in glial cells in response todamage to the CNS § Glial nodule formation § Occasional neuronal degeneration and necrosis |
|
|
What CNS lesions does FIP cause? |
leptomeningitis, chorioependymitis, focal encephalomyelitis and ophthalmitis
|
|
|
What is the pathogenesis of the rabies virus? |
§ Inoculation of the virus into a wound bite (biteof a rabid animal) and establishment of infection
§ Virus replicates in myocytes around the wound § Viral particles invade the local neuromuscularjunction to ascend to the CNS and paravertebral ganglia via axoplasmic flow§ Viral replication in the CNS is followed byspread to the major exit portals (adrenal gland, nasal mucosa and salivaryglands) § Virus shed in saliva |
|
|
What is the pathogenesis of Canine Distemper virus? |
Following primary viraemia, a secondary viraemia occurs with systemic epithelial colonisation and viral shedding
Dogs with adequate humoral and cell-mediated immunity may recover within 14 days, otherwise they may develop severe disease Virus spreads haematogenously to the brain and choroid plexus and infects astrocytes and microglia White matter vacuolation (intramyelinic oedema) is thought to result from a direct effect of the virus on oligodendrocytes |
|
|
What is significant about Oligodendrocytomas? |
All are malignant :O |
|
|
How does the location of a Meningioma affect the neoplasms behaviour? |
§ Most intracranial mengiomas are benign,extracranial ones tend to be aplastic and locally aggressive
|
|
|
What causes Equine Laryngeal Hemiplegia? |
§ Clinical manifestations are the consequence ofdenervation atrophy of the intrinsic muscles of the left side of the larynx
§ The underlying lesion is idiopathic degenerationof the left recurrent laryngeal nerve |
|
|
What Nervous system lesions does Acute Polyradiculoneuritis (Coonhound Paralysis) cause? |
Wallerian degeneration affecting ventral roots with axonal reaction in motor neurons and denervation muscle atrophy in muscle
|
|
|
What is the normal function of skin? |
• Physical barrier that protects the body from desiccation and infection: layer of keratin important to keep bacteria out and fluid in
• Regulates body temperature, blood pressure and electrolytes • Produces vitamin D • Skin is a key component of the immune system |
|
|
What are 2 skin or muscle abnormalities that have been intentionally breed into domestic animals? |
Congenital hypotrichosis: Animal born with not enough hair e.g. Mexican hairless or Chinese Crested dogs Congenital muscle hypertrophy e.g. Belgian Blue cattle |
|
|
What is the difference between acute solar dermatitis and photosensitisation? |
• Acute solar dermatitis (sunburn) is caused by too much UV light hitting the skin. Some of the UV goes through the epithelium and hits the basal cells. This causes mutations in the basal cells that makes most of them atrophied or die. The red adjacent undamaged basal cells divide and move under dead basal cells
• Acute solar dermatitis is uncommon in animals without prior sensitisation • Photosensitisation has the same pathogenesis as sunburn but it involves a photosensitisation agent. The UV hits photosensitisation agent in the basal cells, causing them to release free radicals that kill basal cells o Primary photosensitisation agents are dietary factors such as St John’s Wart or tetracycline o Secondary photosensitisation is hepatogenous |
|
|
List potential sequelae of chronic sun exposure |
- Solar elastosis and fibrosis (causes thickened,wrinkled skin) - Squamous cell carcinoma - Hemangiomas and hemangisarcomas in dogs - Melanomas in goats |
|
|
Describe the pathogenesis of facial eczema |
· Ruminant eats plant contaminated with Sporidesmin. This toxin causes liver damage
· Normally chlorophyll is broken down into protoporphyrin and excreted into bile · But when there is liver damage, protoporhyrin can’t be excreted and it subsequently builds up in the dermis. When the protoporphyrin in the dermis is struck with UV light, it releases free radicals which damage the basement membrane |
|
|
Name and describe 2 skin conditions caused by behavioural disorders |
Acral lick dermatitis (dogs) o Animal gets addicted to chewing and licking feet o Causes skin to become thickened and recurrent bacterial infections o Considered canine variant of obsessive compulsive dermatitis Feline Psychogenic Alopecia o Cats chronically groom – behavioural disorder in middle-aged anxious female cats o Alopecia without epidermal or dermal changes o Ventral abdomen and medial thigh most affected |
|
|
What causes a callus? |
o Skin squished between overly bony prominences (e.g. ankle) and hard bedding
o Fibrosis leads to follicular plugging which predisposes them to bacterial furunculosis and callus pyoderma |
|

What's going on here? |
Skin Fold Dermatitis |
|
|
What is the difference between superficial and deep bacterial skin infections? |
• Superficial skin infections is when bacteria are present outside the basal cells (in the epidermis). Deep skin infections occur when bacteria are present within the dermis
• In superficial skin infections, the body doesn’t have to amount an immune response as normal basal cell maturation will push the infection out – cannot cause systemic infection |
|
|
List 6 superficial bacterial skin diseases |
o Superficial pustular dermatitis: puppy pimples
o Canine pyotraumatic dermatitis: initiated by self-trauma o Dermatophilosis: chronic dampness damages epidermis, and bacteria colonise damaged epidermis o Exudative epidermatitis of pigs (greasy pig disease): abrasions on skin infected by Staph Hyicus, marked smelly lesions spread over body – can be fatal in neonates o Fleece rot: long fleece entraps moisture allowing colonisation by Pseudomonas Aerugninosa o Equine Pastern Dermatitis: Like dermatophysis except no laminar crusts. Chronic damp housing leads to bacterial infection of the pastern and heel |
|
|
List 4 different deep bacterial skin diseases |
o Staph Folliculitis (superficial pustules) and Furunculosis (deeper boils)
Follicles rupture, allowing bacterial spread to the dermis o Cat bite abscesses o Mycobacterial infection: granulomatous dermatitis o Botryomycosis: secondary wound infection – with little yellow granules |
|
|
Name 3 virus families that can cause only skin lesions |
Poxviruses, Parapoxviruses and papillomaviruses |
|
|
Name 3 different diseases caused by Papillomaviruses |
o Canine oral papillomatosis: spontaneously resolve in a few months
o Bovine fibropapillomas: develop most commonly on the penis and vulva o The equine sarcoid: most common skin neoplasm of horses, recurrence common,metastasis uncommon |
|
|
Tell me about Dermatophytosis |
That's ringworm o Young animals, crowded and humid conditions predispose animals to ringworm o Microsporum canis is the most common cause o Fungi cause lysis of hair shaft, lytic keratin stimulates inflammation causing further damage to keratin o If severe they can develop furunculosiso See focal crusting and alopecia o Zoonotic disease o Shine a UV light on the animals to see if it fluoresces (not a great test) o Self-resolving |
|
|
When might you see Malassezia dermatitis |
o Normal ear inhabitant, but overgrowth can cause otitis and dermatitis if defences are down Seborrhoea (overactive sebaceous glands – oily skin) predisposes
o West highland terriers are predisposed |
|
|
What is the most common systemic mycosis in companion animals? |
• Cryptococcus Neoformans (cryptococcosis)
|
|
|
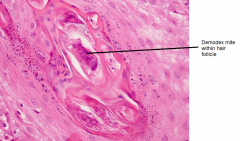
Under what conditions can demodectic and sarcoptic mange develop? |
• Demodectic mites are present in the skin of all animals. They become a problem and cause demodectic mange when there is immunosuppression
• Sarcoptic mites are not normally present and can cause mange regardless of immunosuppression • Sarcoptic mange can develop with only a few mites, demodectic mange needs lots |
|
|
What are some differences between sarcoptic and demodectic mange? (excluding how they develop) |
• Sarcoptic mange responds well to treatment, demodectic mange is difficult to treat
• Sarcoptic mange is intensely pruritic while demodectic mange is pruritic in dogs but not in cats • If you see sarcoptic mites in skin scrape, it is pretty uch diagnostic for sarcoptic mange. However, if you see demodex mites, it does not necessarily mean that the animal has demodectic mange • Demodectic mange most commonly affects young animals (<1 yr). Sarcoptic mange affects any age • Sarcoptic mites live in tunnels they made in the epithelium, demodectic mites live in follicles • Sarcoptic mange in contagious and zoonotic, demodectic mange is not |
|
|
What’s the difference between allergic skindisease and auto-immune skin disease?
|
• Allergic skin disease is an abnormal response against an antigen (allergen) • Auto-immune skin disease is where antibodies are produces against skin cells • Allergic skin disease is common, auto-immune is not
|
|
|
What are the 4 groups of allergen in dogs and cats? |
• Fleas• Atopy (environmental)• Food• Contact allergies
|
|
|
What are the 4 ways feline allergic dermatitis can present? |
1- Chronic self-trauma (as with canine allergic dermatitis) 2- Miliary dermatitis 3- Feline eosinophilic granuloma 4- Feline eosinophilic plaque |
|
|
What is miliary dermatitis |
o Multiple small hard nodules, especially over the dorsum
o Histologically appear as intradermal eosinophilic and neutrophilic pustules covered by a serocellular crust – associated more with flea allergy |
|
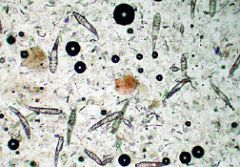
Here's a skin scraping from a dog with skin lesions. What does it have? |
Demodectic mange |
|

If you found this little bitch on an animal, you can be pretty confident if has what? |
sarcoptic mange |
|

So this puppy has been very itchy in the past couple of days. You also notice the client is itchy too. What does the dog have? |
Sarcoptic mange |
|

this dog initially developed lesions around the eyes. It has been treated with antibiotics and steroids and it responded initially but now the lesions are everywhere. What is the most likely diagnosis? |
Demodectic Mange |
|
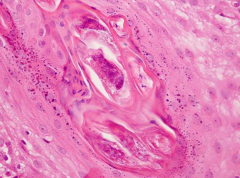
What does this skin biopsy reveal? |
|
|

This rabbit has had mild pruritis and a mild thickening of dried keratin. What is the most likely diagnosis? |

Cheyletiellosis |
|
|
What lesions do you see usually in equine allergic dermatitis? What allergen is usually responsible? |
· More commonly localised pustules or nodules inplaces where flies bite · See eosinophils and lytic collagen in histo · Lesions are ulcerative · Horses only species that commonly develop hivesin response to allergen exposure · Caused by stable flies usually |
|
|
What's the difference between flea allergy dermatitis and atopic dermatitis? |
• Flea allergy dermatitis occurs most frequently in the summer, atopic dermatitis occurs most often in the spring (depending on allergen)
• Flea allergy dermatitis has characteristic Christmas tree lesion distribution on lower back, atopic dermatitis usually causes foot-chewing and face rubbing • The allergens causing atopic dermatitis are present in the environment, often inhaled. Flea saliva is the allergen in flea allergy dermatitis |
|

What's this dog got? |
Flea Allergy Dermatitis |
|

This 9yo dog has recently developed bilateral alopecia (but not on the head or limbs) and a pot belly. The owner also thinks the dog might be drinking more. What is the most likely diagnosis |
Cushing's Disease |
|
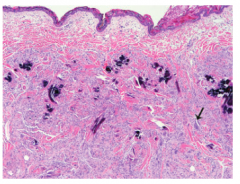
This slide from a skin biopsy is showing multifocal mineral deposition with significant inflammation and multinucleated giant cells (arrow). What does this dog most likely have |
This histology slide shows calcinosis cutis: a distinctive lesion of cushing's disease in dogs |
|
What skin condition in cats do these pictures show? |
Feline Eosinophilic plaque |
|
|
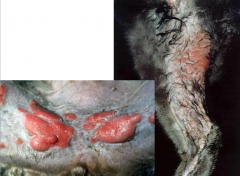
What is the most likely diagnosis of a heifer that has developed crusting lesions over the dorsum and around the hindquarters (and some lesions on the hooves). On histology, the skin showed a characteristic multi-layered appearance with lots of degenerative neutrophils and thick keratin |

Bovine Dermatophilosis |
|
|
What is the mechanism behind Pemphigoid skin diseases? |
• Antibodies produced against cell adhesion molecules. This leads to loss of cell adhesion in the epidermis, causing pustule and vesicle formation
• Different pemphigoid disease relate to the specific cell adhesion molecules the auto-antibodies target (different kind of cell adhesion molecule in each layer of the epidermis) |
|
|
What is Pemphigus Foliaceus? |
o Least severe pemphigoid disease but most common
o Causes pustules in the superficial epidermis o Seasonal and pruritic, oriental dog breeds predisposed o Face, ears and feet affected |
|
|
What is the difference between Discoid Lupus Erythematosus (DLE) and Systemic Lupus Erythematosus (SLE)? |
• DLE is benign, localised disease due primarily to sunlight – like acquired photosensitivity. Lymphocytes are activated by sunlight. Treat by limiting sunlight
• SLE is generalised and usually fatal and true autoimmune disease. Systemic deposition of antigen-antibody complexes due to antinuclear antibody. The immune complexes get stuck in between dermis and epidermis. Lymphocytes come along and attack immune complexes |
|
|
List the 4 non-thyroid skin endocrinopathies of dogs |
1- Cushing's Disease 2- Cyclical Flank alopecia 3- Sex hormone responsive dermatosis 4- Growth hormone responsive dermatosis |
|
|
Describe the clinical signs of a dog with hypothyroidism |
o Obesity
o Lethargic o Seek heat sources o It may cause Seborrhoea Reduced hair growth after clipping Increased dermal mucin Secondary bacterial or yeast skin infection |
|
|
(T/F) Hypothyroidism is underdiagnosed |
False. It is overdiagnosed. It is hard to accurately diagnose as T4 will be decreased in all sick dogs |
|
|
Describe the skin lesions common to all non-thyroid endocrinopathies
|
· Follicles in telogen phase with loss of hairbulb – diagnostic
· Follicular atrophy and plugging |
|
|
What clinical signs does cyclical flank alopecia cause? Is it treatable? |
No clinical signs, just seasonal alopecia. Don't need to treat it as it resolves itself and doesn't bother the dog |
|
|
How can nutritional deficiencies result in hair loss
|
• Hair is protein, insufficient dietary protein prevent hair production
• Deficiency in some minerals also prevents hair production |
|
|
What is seborrhoea |
Excessive discharge of sebum from sebaceous glands
|
|
|
Describe puppy Strangles |
Juvenile Sterile Granulomatous Dermatitis o See in puppies <4 months - idiopathic cause o Nodular swelling in the dermis, involving the face, ears and mucocutaneous junctions o Mandibular lymphadenopathy common – strangles o Responds to corticosteroids suggesting the immune system plays a role |
|
|
Describe Plasma cell Pododermatitis |
o AKA cushion/pillow pad
o Swelling of one or multiple paws o Cytology reveals a lot of plasma cells o Only in cats o Some cases respond spontaneously, other respond to corticosteroids o Primary lesion not painful unless it ulcerates o Can diagnose with FNA |
|
|
What is the normal ratio of thickness of the right ventricle wall to the left ventricle wall? |
Left ventricle wall is 3x thicker |
|
|
Describe how cardiac muscle heals and the implications of it
|
• Cardiac muscle cannot regenerate, so it must heal by fibrosis
• This results in decreased contractility and strength • The heart has only a 3-5 fold functional reserve before compensation is required – then CHF |
|
|
What can cause left-sided congestive heart failure? |
Valvular dysfunction (left AV or aortic) – regurgitates blood back into heart
Left ventricular myocardial necrosis – cannot produce enough force Endocardiosis – shortens the AV valves |
|
|
Describe the mechanism behind a 'night cough' |
Left sided congestive heart failure results in excess blood being in the pulmonary circuit. This causes pulmonary oedema, which isn't a problem to the animal when it is moving around but when it goes to sleep at night, the fluid has time to accumulate and the dog coughs (night cough). |
|
|
What can cause right sided congestive heart failure? |
Pulmonary hypertension – due to left-sided CHF or equine COPD (heaves)
Heart filling defects e.g. pericarditis Myocardial damage |
|
|
How does right sided congestive heart failure usually present in different species? |
§ Ascites common in dogs affected by RSCHF
§ Hydrothorax common in cats § Dependent subcutaneous tissues common in horsesand production animals – most obvious in brisket or mandible |
|
|
How are the liver and kidneys affected by right-sided congestive heart failure? |
o Liver usually the most severely affected by RSCHF Leads to hypoxia and necrosis Hepatocytes repaired by fibrosis – see in PM (nutmeg liver) + dilated central veinso Additionally, renal blood flow is reduced, activating the renin-angiotensin system Releases aldosterone, promoting sodium retention – increased osmotic pressure in blood This increases blood volume, making congestion worse |
|
|
What are the different categories of cardiac hypertrophy? |
• Physiologic
o Exercise-trained animals • Primary pathologic hypertrophy o Disease within the myocardium, such as idiopathic hypertrophy • Secondary pathologic hypertrophy o In response to a non-myocardial disease process, such as a sub-aortic stenosis |
|
|
Describe a patent ductus arteriosus |
o Common in dogs, esp. poodles
o Ductus arteriosus normally connects the aorta and pulmonary artery in the foetus. It is supposed to close at birth but sometimes can remain open o Changes the normal 1:3 ratio between the right and left ventricles’ myocardial thickness |
|
|
What are the 4 things wrong with the cardiovascular system of an animal suffering from tetrology of Fallot? |
Ventricular septal defect
Pulmonary valve stenosis Aortic transposition Secondary right ventricular hypertrophy |
|
|
What is a subaortic stenosis? |
o Narrowing of the left ventricle just below the aortic valve
o Predisposes to myocardial infarction – heart attacks |
|
|
What are the 2 most common congenital large blood vessel abnormalities? |
Persistent Right Aortic arch and Transposition of the aorta or pulmonary artery |
|
|
Describe the different variations of a transposition of the aorta or pulmonary artery |
Both arteries originate within the same ventricle
Aorta and pulmonary artery swapped so that aorta originates in the right ventricle One artery originates within both ventricles |
|
|
What are the 2 forms of pericarditis? |
Purulent- pyogenic bacteria – e.g. Hardware disease
Fibrinous – usually due to haematogenous spread of bacteria, damaged blood vessels leak into pericardial sac – e.g. Haemophilus Parasuis |
|
|
What causes Mulberry heart disease in pigs? |
Vitamin E/Selenium deficiency results in free radical damage to the endothelium. Endothelial damage can result in blood and fibrin leaking into the pericardium. |
|
|
What are 3 potential causes of Haemopericardium |
1- idiopathic 2- In dogs, it’s most commonly due to rupture of a right atrial Hemangiosarcoma 3- In pigs and horses, it is most commonly due to spontaneous rupture of the proximal aorta |
|
|
What major cardiovascular lesion does enterotoxaemia cause? |
o Large fibrin clots within the pericardium
o Overgrowth of clostridium produces toxins, toxins absorbed, damages blood vessels, fibrin leaking out everywhere |
|
|
Identify a common cause of endocardial mineralisation in most species and a different cause common in cattle
|
• Endocardial mineralisation is most commonly a jet lesion due to valvular insufficiency
o Jet lesions can occur when valves are regurgitating blood or when there are narrow valves • Cattle can get endocardial mineralisation due to chronic debilitation e.g. Johne’s disease |
|
|
Describe endocardiosis
|
• Idiopathic degeneration of valvular collagen
• Almost ubiquitous in older dogs, Esp. CKC Spaniels • Valve cusps shortened and nodular • Severe lesions result in loss of patency and CHF |
|
|
What are the predispositions of atrial thrombosis? |
o Slow or turbulent blood flow pre-disposes to this condition e.g. atrial hypertrophy and valvular regurgitation
o Blood flow slowest in atria – so atria common place |
|
|
What are some potential sequelae of atrial thrombosis? |
o Large thrombi can result in sudden death
o Small thrombi can produce emboli and infarction elsewhere in the body – kidneys and aortic trunk are common places emboli get stuck |
|
|
What's the difference between lesions of endocarditis and lesions of endocardiosis? |
• Endocardiosis has short nodular cusps, endocarditis has bacteria, fibrin and blood cells that attaches to thrombi – may become large proliferative lesions - vegetative
|
|
|
What can cause Myocardial necrosis? |
o Vitamin E/selenium deficiency
o Ionophore toxicity o Doxorubicin toxicity o Physical injury and shock |
|
|
Describe the appearance of acute and chronic myocardial necrosis |
Acute appears as poorly defined white streaks on heart
Chronic often has a chalky appearance due to mineralisation |
|
|
What are 2 causes of a cardiomyopathy? |
o Primary (idiopathic)
o Secondary (e.g. Taurine deficiency) |
|
|
Describe feline hypertrophic cardiomyopathy |
• Idiopathic or due to hyperthyroidism
• Ventricle walls become thickened with markedly reduced chamber volume • Myocardial fibrosis and loss of normal myocyte arrangement • The bigger the cat the more likely it is to develop HCM |
|
|
What are some potential sequelae of feline hypertrophic cardiomyopathy? |
o Die without any clinical signs
o Die during anaesthesia o Develop atrial thrombi and aortic emboli o Develop CHF |
|
|
Briefly describe dilated cardiomyopathy |
• More common in dogs
• Idiopathic in large breeds • CHF most common presenting sign • Radiograph revels large round heart • Histologically get myocyte replacement with adipose |
|
|
List the infectious causes of Myocarditis
|
• Viral e.g. canine parvovirus or encephalomyocarditis vrus in pigs
• Bacterial, usually secondary to bacteraemia e.g. Clostridial and mycobacterial myocarditis • Parasitic e.g. toxoplasmosis in young dogs and cats, Neospora in calves or intermediate stages of tapeworms in sheep |
|
|
Describe 2 of the most common neoplasms ofthe heart
|
• Canine Right Atrial Hemangiosarcoma
o Common site for Hemangiosarcomao Results n extensive myriad lung metastases • Lymphosarcoma in cattle o Infection with bovine leukaemia virus causes tumours in the heart, abomasum, uterus, spinal cord and lymph nodeso Often present with CHFo Prevalent in the dairy industry in the Americaso Most of the myocardium is infiltrated with neoplastic cells |
|
|
Explain how changes to the endothelium affect blood coagulation
|
• Damage to the endothelium prevents the production of factors crucial for preventing clotting
• Exposure of blood vessel collagen causes activation of the clotting cascade |
|
|
Define aneurysm
|
• A focal outpouching of an arterial wall
• Any reduction in vessel wall strength predisposes aneurysm formation |
|
|
Describe the predisposing factors of arterial thrombosis
|
• Altered or damaged endothelium – can’t produce anti-clotting factors
• Turbulent or slowed blood flow • Hypercoagulability of the blood – not really an important cause in animals |
|
|
What can cause an arterial embolism? |
o hypertrophic cardiomyopathy in cats
o Rarely seen with dogs with DCM o Septic endocarditis o Septic emboli from bovine hepatic abscesses o Strongylaris Vulgaris o Air or hair emboli o Fibrocartilage from the intervertebral discs |
|
|
What is the most common kind of arterial embolism |
Saddle embolus
o Stuck at aortic bifurcation – causes infarction of hind limbs o Animals get cold legs with pain or paresis with no femoral pulse |
|
|
What is atheroschlerosis? |
• Atheroschlerosis is loss of compliance of an artery due to focal accumulation of fatty fibrous tissue
|
|
|
What animals does atheroschlerosis affect most commonly |
Primates (incl. humans) and parrots |
|
|
What can cause arterial calcification? |
o Occurs in cattle due to chronic debilitation – won’t show symptoms of cardiovascular diseases
o In other animals it is usually caused by cholecalciferol toxicity |
|
|
What are 5 causes of infectious arteritis? |
1- Erysipelothrix 2- FIP 3- Malignant Caterrhal Fever 4- Strongylus Vulgaris 5- Heartworm |
|
|
Describe the pathogenesis of FIP? |
• Ab-Ag complexes trapped within smaller blood vessels
• Inflammatory cells destroy immune complexes and vessels in the process- Vasculitis • Fibrin leaks out of blood vessels -oedema • Thrombi form within vessels, resulting in ischaemic tissue damage |
|

This is a heart from a 1yo sheep. What has it got? |
Endocarditis (bacterial/streptococci endocarditis to be exact) |
|

This is a heart from an 11yo dog. What has it got? |
Endocardiosis |
|
A 14yo German Shepherd has died suddenly. What was going on here? |
Right Atrial Hemangiosarcoma |
|
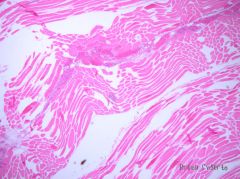
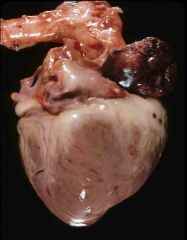
This slide from muscle in a cow's leg shows necrotic myocytes, oedema and emphysema. What is the most likely diagnosis? |
Blackleg |
|
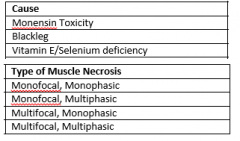
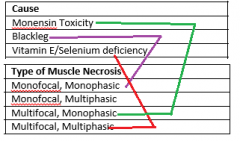
Match the type of muscle necrosis with the cause |
|
|
|
Describe how skeletal muscle heals |
• If the sarcolemma is intact, complete regeneration possible
o Macrophages enter and remove debris o Satellite cells produce more muscle proteins o Cells return to sarcolemma surrounding myocyte • More severe damage causes complete myocyte necrosis and fibrosis fills in the gap left in the muscleo Decreased contractile force of muscle o Fibrous cells tend to be shorter – can’t strectch |
|
|
Describe different ways an animal can have altered myocyte size
|
• Denervation atrophy: rapid and marked decrease in myocyte size due to nerve damage to the nerve supplying that muscle
• Disuse atrophy: caused by restricted movement of limb. Less severe than denervation atrophy • Cachexia atrophy: marked malnutrition or neoplasia causes it. Tyically postural muscles less affected • Physiologic hypertrophy: due to exercise • Pathologic hypertrophy: due to loss of contralateral limb or loss of other myocytes within muscle (compensation) |
|
|
What clinical pathology abnormalities might you expect in skeletal muscle disease? |
• Myocyte necrosis releases CK, AST and myoglobin – can see on biochemistry
o CK specific for muscle but has a short half-life – so only elevated for a short period following necrosis event o AST released from muscle and hepatocytes but has a longer half-life o The higher the enzymes, the more severe the necrosis o If both CK and AST are up then active necrosis is going on, if only AST is up, then multiphasic • Marked increase in myoglobin results in brown blood, urine and myoglobinuric nephrosis |
|
|
Describe the pathogenesis of malignant hyperthermia in pigs
|
• Triggered by stress or halothane
• Defect in ryanodine receptor causes uncontrolled sustained contraction of skeletal muscle • Excessive heat produced by this contraction results in myocyte necrosis – so all cells die at the same time – so multifocal, monophasic necrosis |
|
|
What is the most common skeletal muscle storage disease |
• The most common is polysaccharide myopathy o Common in draft breed horses
o Recurrent episodes of exertional rhabdomyolysis results in fibrosis and associated weakness o Muscle biopsy used to diagnose – it reveals large quantities of intracellular carbohydrate |
|
|
What is the pathogenesis of exertional rhabdomyolysis in horses |
o Horses/zebrausually run in the wild until glycogen runs out. This happens before there is damage to muscles by excessive heat and lactic acid. So horses did not develop a system to say ‘hey, we are making too much lactic acid and heat’. But in domestic horses, we feed them lots, so they can build up heaps of glycogen. This enables them to run for ages and risk damage to muscles caused by excessive lactic acid and heat production
|
|
|
Describe the clinical presentation of a horse with exertional rhabdomyolysis |
o Stiffness, muscle swelling, pain immediately following strenuous exercise
o Myocyte necrosis results in an initial increase in serum CK – followed by an increase in AST o Can get myoglobinaemia and myoglobinuria nephrosis |
|
|
Briefly describe capture myopathy
|
• Necrosis caused by prolonged muscle activity – damage done by heat and lactic acid
• Animals can die quickly of metabolic acidosis or later of myoglobinuric nephrosis |
|
|
Describe the pathogenesis of Blackleg |
o Clostridial spores ingested and remain dormant in oxygenated muscle
o Traumatic injury results in muscle hypoxia o Spores then germinate and bacteria proliferate in this newly anaerobic environment o Toxins cause vasoconstriction resulting in more muscle hypoxia and inhibiting inflammation – expands zone of inflammation o Animals can die rapidly of toxaemia |
|
|
Describe the pathogenesis of gas gangrene |
o Environmental Clostridia invade deep penetrating wounds
o Wounds have local hypoxia allowing proliferation o Toxin production causes further necrosis and inhibits inflammation o Death often rapid due to toxaemia |
|
|
What is 'Big Head' |
o Specific type of gas gangrene, usually caused by C.Novyi
o Tissue damage occurs due to head-butting rams |
|
|
Briefly describe wooden tongue
|
· Usually involves connective tissues of the tongue, but can extend to a glossal myositis· Caused by infection of cuts by Actinobacillus Lignieresii
|
|
|
What are the 2 most common parasitic myositis'? |
Cysticercosis and Sarcocystosis |
|
|
Compare and contrast polymyositis and masticatory myositis
|
• Polymyositis involves antibodies attacking all skeletal muscle – multiphasic
• Masticatory myositis involves auto-immunity against type II masticatory myosin – fibrosis and atrophy of masticatory muscles |
|
|
Describe the pathogenesis of Vitamin E/Selenium Deficiency |
o When mitochondria produce ATP, free radicals are also produced.
o VitaminE/selenium scavenge free radicals, preventing oxidative damage. But when there is a deficiency, the free radicals are able to cause damage. o Muscle affected most as it contains the most mitochondira. It also causes vasculitis o Cardiac muscle and more active skeletal muscles affected first o Death due to heart failure or respiratory failure by costal muscle damage |
|
|
Under what conditions is Monensin Toxicity most likely? |
When horses are fed cattle rations of monensin, when animals are fed incorrectly mixed rations or when dogs scavenge monensin boluses |
|
|
What is the pathogenesis of Monensin Toxicity? |
o Monensin prevents mitochondria producing ATP
o ATP essential for maintaining cell integrity – Na+/K+ pump o Fluid moves into cell and cell swells o Multifocal monophasic necrosis o If sublethal dose, animals’ often die of CHF due to cardiac necrosis and fibrosis |
|
|
What are the components of the glomerular filtration barrier? And what is a consequence of it being damaged? |
o Gaps between endothelial cells
o Basement membrane o Gaps between podocytes (visceral epithelialcells) Damage to it may result in protein loss into the urine (protein-losing nephropathy) |
|
|
What role do medullary solutes play? and what happens when their concentration is lowered? |
o Maintains an osmotic gradient causing fluid to move out of the tubules
o Disruption to this osmotic gradient means the kidneys are unable to concentrate urine – polyuria |
|
|
Define Isosthenuria |
Urine specific gravity equals serum (1.008-1.012)
|
|
|
Why are animals with renal failure also in a state of metabolic acidosis? |
Renal failure causes increased urinary loss of bicarbonate and decreased tubular secretion of H+
|
|
|
One potential consequence of renal failure is endothelial damage. How does this happen? What are some potential sequelae of this? |
o Caused by uraemic toxins
o Causes thrombosis o Mucosal ulcers Caustic effect plus infarction due to thrombosis of small vessels Oral cavity and stomach affected in small animals, colon in large animals o Endothelial damage results in increased vascular permeability and fluid loss into body cavities – hydropericarium, ascites, pulmonary oedema |
|
|
What is the mechanism behind renal secondary hyperparathyroidism? |
As filtration decreases, P starts to be retained (hyperphosphataemia). P combines with Ca and precipitates (metastatic calcification). This reduces the concentration of serum calcium (hypocalcaemia) which causes increased PTH secretion. The body tries to increase Ca but P get increased aswell. This results in the parathyroid gland becoming enlarged
|
|
|
What type of azotaemia will a cat with bloody, tarry faeces, elevated urea and normal creatinine have? |
Non-renal |
|
|
What causes post-renal azotaemia? How do they cause it? |
o Caused by obstruction of excretion of urine – ruptured bladder or urinary tract obstruction
o In bladder ruptures, the urine is leaked into the peritoneal cavity and the urea and creatinine is reabsorbed into the blood stream o In urinary tract obstructions, the urea and creatinine build up and are backed up through the kidneys and blood |
|
|
What aspects of an animal's clinical presentation will be different for acute renal failure, compared with chronic renal failure |
o Will be very ill all of a sudden
o If supported through uremic stage, then they can recover full renal function o Oliguria/anuria o Kidney can be very painful and swollen o Uremic breath o Hyperkalaemia |
|

What's going on here? |
Fused kidneys (Horseshoe kidneys) |
|

What's going on here? |
Cystic Kidneys |
|

What's going on here? |
Glomerulonephritis |
|

What's going on here? |
Amyloidosis |
|

What's going on in this kidney? |
Suppurative Glomerulitis |
|

What the f*ck is this? |
White-spotted kidney disease in cattle (caused by E.Coli septicaemia) |
|

What does this poor kitty have? |
Pyelonephritis |
|
What's the little black arrow pointing to? |
Renal papillary necrosis |
|

What happened to these kidneys? |
Hydronephritis |
|
This isn't amyloidosis, so it must be... |
renal lymphoma in a cat |
|

What is wrong with this urinary tract? |
ectopic ureters |
|

What is responsible for this little urinary bladder diverticulum? |
Patent Urachus |
|

What is the yellow arrow pointing to? |
Uroliths in the bladder |
|
What is causing this cat's bladder to look like this? |
A urinary tract obstruction. Note large size and haemorrhage |
|
|
Describe the potential clinical presentation of an animal with acute renal failure |
o History
Sudden onset Has eaten something they shouldn’t haveo Clinical signs Oliguria/anuria Uremic breath Abdominal pain on palpation Dehydration o Abnormal Clinical pathology Swollen, large kidneys Azotaemia Hyperkalaemia Isosthenuria (maybe) Metabolic acidosis Petechial haemorrhages in oral cavities, ulcers on gums Black, tarry faeces |
|
|
Describe the potential clinical presentation of an animal with chronic renal failure |
o History
Been ill for a while Older dog/cat o Clinical signs Polyuria/polydipsia Dehydration Pale MM (maybe) Oral or GIT ulcers Petechial haemorrhages in oral cavity Black, tarry faeces o Abnormal Clinical pathology Azotaemia Isosthenuria Small, firm kidneys Non-regenerative anaemia Metabolic acidosis Hyperphosphataemia Normal or decreased Ca Radiolucent bones, especially the mandible (maybe) Calcium phosphate ppt in lungs and renal tubules – histology Enlarges parathyroid gland Hypokalaemia (maybe) Fluid in body cavities Bleeding diathesis
|
|
|
What lesions does pyelonephritis cause? |
o Inflammation of the renal pelvis and renal parenchyma
Accumulation of pus in pelvis Atrophy of the renal medulla and interstitium Fibrosis of capsule |
|
|
What are some predisposing factors of pyelonephritis? |
§ Urethral obstruction
§ Bacterial cystitis § Congenital malformation of ureters or sphincter § Specific gram –ve infections § Bacterial adhesion factors § Shape of female urethra |
|
|
What does immune-mediated glomerulonephritis cause? |
o Causes inflammation of the glomerulus, which constricts the blood supply to the nephron. Eventually causing necrosis of the whole nephron and fibrosis throughout the whole kidney
Also causes activation of complement Attracts neutrophils Produce proteases and free-radicals |
|
|
Where is Amyloid deposited in the kidney of a dog? What clinical abnormalities does this cause? |
Amyloid deposited in glomerulus (causes a protein-losing nephropathy) - Proteinuria - Hypoalbuminaemia - Oedema |
|
|
Where is Amyloid deposited in the kidney of a cat? What clinical abnormalities does this cause?
|
Amyloid deposited in medullary interstitium
- Usually asymptomatic - Can cause renal papillary necrosis |
|
|
What can amyloid be made from? |
Can be made from acute phase proteins or light chains from immunoglobulins
|
|
|
What are some predisposing factors for urolithiasis? |
Urinary stasis
Dehydration Urinary tract infection High mineral content in urine pH of urine affects solubility of minerals Males predisposed to obstruction |
|
|
What clinical signs would you expect in an animal with urolithiasis (without obstruction)? |
a. Dysuria (difficulty urinating)
b. Stranguria (straining) c. Haematuria (whole blood in urine) d. Pollakiuria (increased frequency of urination) e. Behavioural changes f. Inappropriate urination |
|
|
What additional clinical abnormalities would you expect in an animal with urolithiasis and obstruction compared to an animal with urolithiasis with no obstruction? |
Uraemia (every clinical abnormality associated with renal failure) and shock (brick red mucous membrane and sometimes dehydrated and pale). Also a firm, full bladder on palpation |
|
|
What type of urinary crystals are most common in cats? |
Predominantly calcium phosphate crystals (use to be predominanty struvite back in the day)
|
|
|
What type of urinary crystals are most comon in dogs? |
§ 50% of crystals are struvite
§ 30% of crystals are calcium oxalate |
|
|
Does it matter what kind of urinary crystal an animal has? |
Yes. Even though they cause the same disease, the treatment will be different depending on what type of crystal is there |
|
|
What predisposes sheep to urolithiasis? Is it a significant problem? |
Caused by pastures high in oxalates, phosphates or oestrogens. Not a significant problem, usually an incidental finding
|
|
|
What is the most common site for urinary tract obstruction in dogs and cats? |
• Cats: entire urethra • Dogs: proximal end of os penis (urethra most narrow there) |
|
|
What is the most common site for urinary tract obstruction in bulls/steers and rams/whethers?
|
• Bull/steers: ischial arch, sigmoid flexure
• Rams/wethers: urethral process |
|
|
What can obstruct the urinary tract? |
Masses – neoplasms, polyps
Inflammatory diseases e.g. FLUTD Uroliths Urethral plugs Scarring – trauma, catheterisation |
|
|
What are the 4 possible causes of Feline Lower urinary Tract Disease (FLUTD)? |
I. Idiopathic – most common
II. Urolithiasis III. Bacterial cystitis IV. Neoplasia – least common |
|
|
What are the clinical signs of Feline Lower urinary Tract Disease (FLUTD)? |
-Dysuria -Pollakiuria -Haematuria -Vocalisation -Inappropriate urination |
|
|
What can cause cystitis? |
Chemical agents and natural toxins
a. Cyclophosphamide b. Blister beetles c. Bracken fern Uroliths, tumours and bacterial infection Bacteria a. E.Coli most common b. Mostly gram –ve |
|
|
What factors predispose an animal to a UTI |
i. Female urethra
ii. Trauma (uroliths, catheterisation) iii. Glucosuria (diabetes mellitus) iv. Urine stasis v. Dilute urine vi. Urinary pH changes |
|
|
Name 2 causes of toxic interstitial nephritis |
- Leptospirosis - E.Coli Septicaemia |
|
|
What can cause ischaemic nephrosis? |
Haemolytic disease
Renal vasoconstriction – hypovolaemia or NSAIDs Severe hypoxia Sudden onset of severe anaemia |
|
|
What toxins can potentially cause toxic nephrosis? |
Heavy metals
Certain Plants Certain Antibiotics NSAIDs Oxalates Vitamin D Mycotoxins Certain Therapeutic drugs |
|
|
If both kidneys are suffering from hydronephrosis, then where is the most likely place for the urinary tract obstruction responsible? |
The urethra - this means that no urine can get out and so it backs up into both kidneys. If the blockage was in a ureter, then only the corresponding kidney would be affected. |
|
|
What are the 2 ways in which a patent urachus can present? |
o Present with constant dribbling of urine from umbilicus if the urachus is open along its whole length
o If it is only partially open, urine can sit in it (urinary diverticulum). This is a constant source of infection |
|
|
What are two common causes of bladder rupture? |
Foals at parturition- mares contractions so strong they burst the bladder
Urethral obstructions in dogs, cats and small ruminants |
|
|
What is the pathogenesis of Leptospirosis in regards to kidney disease? |
o Enter host via damaged epithelial surfaces
Mucous membrane Traumatised Skin o Bacteria enter blood vessels and travel throughout the body o Localise in the kidneys (also the uterus and liver) o Exit into interstitium – chronic interstitial nephritis o Migrate to renal tubules o Localise in tubular epithelium o Shed in urine |
|
|
How many nephrons need to be damaged before the animal is in renal failure? |
>75% |
|
|
Describe the 2 main categories of immune-mediated glomerulonephritis |
o Anti-basement membrane antibodies attack the basement membrane OR pre-formed complexes are trapped in the basement membrane (see lesions elsewhere in the body too)
|
|
|
What 3 things are required for pyelonephritis to develop? |
Vesiculoreteral reflux
Bacterial contamination of urine Defences must be overcome |
|
|
What Taylor Swift song am I listening to right now? |
Sparks Fly |
|
|
Why is proper and efficient processing of eyes post-mortem so important? |
o The eye undergoes rapid post-mortem/post-enucleation changes that may obscure degenerative lesions and resemble real developmental or degenerative diseaseso Improper handling of the specimen may result in poor quality histologic sections
|
|
|
Describe the cornea histologically |
Histologically, the cornea has an outer stratified squamous epithelium, a central avascular stroma, and an inner endothelium with a thick basement membrane called Descemet's membrane
|
|
|
What structures make up the uveal tract? |
The iris, choroid and ciliary bodies |
|
|
Briefly describe the retina's structure |
The retina is considered an outpouching of brain tissue and is composed of three layers of neurons separated by cell free layers created by the axons and dendrites of these neurons
|
|
|
Describe the direction of flow of aqueous humor |
The aqueous humor is produced by the ciliary body and flows through the pupil and drains into the filtration angle formed by the iris and the cornea (iridocorneal angle). Fluid moves into the trabecular meshwork, to the corneoscleral meshwork and into the scleral vasculature
|
|
|
Define Collie Eye Anomaly |
- AKA Scheleral ectasia - Inherited autosomal recessive trait of collie dogs - Disease is always bilateral but severity may vary between the eyes: it features Retinal vessel tortuosity, focal to difuse choroidal and tapetal hypoplasia, optic nerve coloboma and retinal separation with intraocular haemorrhage |
|
|
Define Coloboma |
Notch-like defects of optic disc, retina, ciliary body and/or iris as a result of defective closure of the embryonic fissure of the eye. It is an outpouching of the eye
|
|
|
Explain the difference between primary and secondary glaucoma |
o Primary: malformation of the trabecular network or the filtration angle, thus impairing filtration resulting in the build-up of intraocular pressure
o Secondary: anything capable of obstructing the outflow of aqueous humor from the pupil or trabecular network. Can be caused by closure of the ciliary cleft/drainage angle, peripheral anterior synechiae, posterior synechiae or obliteration of the trabecular network by inflammatory exudate or neoplasia |
|
|
Briefly describe the pathological changes seen as a result of glaucoma |
Atrophy of the retina and optic nerve Enlargement of the eye (Buphthalmia)
|
|
|
What is Ankyloblepharon? Is it normal? |
Adhesion of the eyelid margins to each other. It's normal in dogs and cats (have physiologic ankyloblepharon until 10-14 days of age)
|
|
|
What is ectropion? What pathological changes might you see in conjunction with it? |
Eversion of the eyelid. There may also be keratitis and hyperaemia |
|

What is wrong with this dog? |
Entropion and secondary trichiasis |
|
|
What can FHV-1, Sarcoptes Scabei, Staph Aureus and sunlight exposure all cause? |
o Blepharitis (inflammation of the eyelid)
|
|
|
List the 3 most common causes of infectious conjunctivitis in cats |
FHV-1 Chlamydophila Felis Mycoplasma Felis
|
|
|
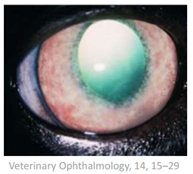
Define what a corneal ulcer is |
A corneal ulcer is an open sore in the outer layer of the cornea. It is often caused by infection.
|
|
|
What are some common causes of keratitis in horses? |
Mycotic keratitis associated with traumatic breaks in the epithelial barrier. Keratitis can also be cause by inappropriate use of topical steroid used on corneal ulcers. |
|
|
What is pinkeye? |
Keratoconjunctivitis in ruminants caused by Moraxella Bovis |
|
|
What happens if a corneal ulcer is deep enough that it reaches Descemet's membrane? |
Descemetocele (outpouching of Descemet's membrane through the ulcer) |
|
|
What is pannus? |
AKA chronic superficial keratitis or German Shepherd pannus Immune-mediated disease that results in corneal vascularisation and pigmentation that may advance across the entire cornea
|
|
|
What is panuveitis and what usually causes it? |
Inflammation of the whole uveal tract (iris, choroid and ciliary body)o Many or most of the inflammations may be related to hypersensitivity in which case the primary cause may be distant to the globe
|
|
|
What does chronic uveitis syndrome in cats look like? |
§ Chronicuveitis with keratic precipitates and darkening and thinning of the iris alongwith small grey raised ‘follicles’ and blood vessel prominence on the irissurface
|
|
|
Outline the equine recurrent uveitis |
o Hypersensitivity to infectious agents is commonly implicated as a cause e.g. Leptospirao Variable degree of uveitis in one or both eyeso Most common cause of blindness in horses
|
|
|
What is Synechiae? What is the difference between the 2 main types? |
The iris adheres to either the cornea (anterior synechiae) or lens (posterior synechiae)
|
|
|
List causes of cataracts |
Occur secondary to glaucoma, diabetes (excessively high level of glucose within the aqueous), endopthalmitis, ocular trauma and anterior segment anomalies. Can also be caused by solar or other irradiation, cold, increased intraocular pressure, toxins, nutritional excesses and deficiencies, nearby inflammation, and direct trauma They can also be familial in certain breeds (inborn errors of lentricular metabolism)
|
|
|
What is retinal dysplasia? |
Abnormal retinal differentiation characterised by jumping of retinal layers and by glial proliferation
|
|
|
What is the most common cause of retinal detachment? |
Usually caused by inflammation of the choroid (breakdown of blood-retinal barrier)
|
|
|
List 3 neoplasms of the eyelid |
Meibomian (Sebaceous) gland adenoma Melanoma Squamous Cell Carcinoma
|
|
|
Are uveal melanomas benign or malignant? |
• Benign in the dog but malignant in the cat
|
|
|
What is the most common intraocular neoplasm? |
Uveal Melanoma |
|
|
List 4 intraocular neoplasms |
-Uveal melanoma - Lymphoma - Ciliary body tumours - Intraocular sarcoma |
|
|
What are some causes for ear tip necrosis? |
Commonly seen in Pigs (May be idiopathic) Typically associated with vascular injury of various etiologies (frostbite, ergotism, thrombosis associated with septicaemia) or trauma Necrotic ear syndrome in pigs (Spirochetosis)
|
|
|
What causes auricular haematomas? |
Occurs as a consequence of trauma, usually excessive head shaking (dogs with otitis externa)
|
|
|
What is the most common cause of otitis externa in cats? |
Otodectes Cynotis mites |
|
|
What predisposes a dog to otitis externa? |
- Increased moisture and inadequate air circulation within the air canal - the presence of foreignbodies or microorganisms (Staphylococcus, Pseudomonas, Proteus, Malasseziapachydermatis) - Atopy or Seborrhoea |
|
|
What pathological changes can occur in the ear due to otitis externa? |
• Epidermal hyperplasia• Acanthosis• Follicular atrophy• Hyperkeratosis • Inflammation crusts• Ulceration• Inflammation• Fibrosis
|
|
|
T/F Otitis media is almost always bacterial |
True |
|
|
List some potential sequelae of otitis media |
May lead to otitis interna, damage to the brainstem or local nerves (facial and vestibulocochlear)
|
|
|
What pathogen commonly causes otitis media in cattle? |
Mycoplasma Bovis |
|
|
How does otitis interna normally present? |
With vestibular signs e.g. head tilt |
|
|
List 3 neoplasms of the external ear of dogs and cats |
- Squamous cell carcinoma - Cutaneous histiocytoma - Cutaneous adenoma/adenocarcinoma |
|
|
Describe the structure of a nasopharyngeal polyp |
Composed of loose connective tissue with numerous small blood vessels, covered by a characteristic simple to bilayered ciliated columnar epithelium
|
|
|
Why are respiratory disease so important in intensive production systems? |
It is estimated that respiratory disease is oneof the leading cause of mortality and loss of production in intensive productionsystems
|
|
|
Describe a normal lung in post mortem |
o Lungs should be smooth and pinko Palpate them and they should be spongy
|
|
|
List the respiratory system's defences |
• Physical barriers• Turbulent airflow in conducting airways and mucociliary transport• Bronchial-associated lymphoid tissue• Alveolar macrophages
|
|
|
List common causes of viral rhinitis in horses |
Equine viral rhinotracheitis (EHV-1 and 4) Equine influenza virus Equine rhinoviruses Equine viral arteritis virus
|
|
|
What is inclusion body rhinitis? |
Infection causing lymphocytic rhinitis with characteristic intranuclear inclusions in pigs
|
|
|
Define Pulmonary Atelectasis |
o Reversible collapse of alveoli without injury to alveolar septa
|
|
|
Define Pulmonary Emphysema |
o Permanent enlargement of alveoli with damage to the alveoli wall
|
|
|
What are the two main mechanisms of pulmonary oedema? List causes for each of them |
Increased permeability of the alveolar capillaries• Interstitial pneumonia• Toxic insults• Anaphylactic shock
Increased hydrostatic pressure in pulmonary vessels - Left-sided congestive heart failure |
|
|
What are some causes of pulmonary haemorrhage? |
Exercise-induced pulmonary haemorrhage in racing horses Trauma with rupture of blood vessels Abscesses which erode pulmonary blood vessels (cattle with embolic lung abscesses) Secondary to septicaemia, DIC, pulmonary thrombosis or embolism
|
|
|
How does the respiratory system respond to injury? |
• Initially there is an increased secretion by serous cells which is followed by increased secretion of mucus by goblet cells• Excessive mucus within the bronchi or bronchioles can impair normal respiratory defences of the lungs• If there is damage to respiratory membranes – fluid leaks in • More type II pneumocytes may be evident as they proliferate to try and cover up defects in alveoli
|
|
|
What is squamous metaplasia |
o Respiratory epithelium is replaced by more resistant squamous epithelium, which cannot undergo gas exchange or move the mucus blanketo May lead to neoplasia
|
|
|
What is bronchiectasis |
o Permanent outpouching of the bronchiole because the airway is dilated and filled with mucus and exudate
|
|
|
What is Bronchiolitis Obliterans |
o Large amounts of epithelium are degraded and the basement membrane is covered by exudate.
The exudate becomes infiltrated by fibroblasts. As the fibrous tissue becomes organised, the lesion contracts causing shrinkage and obliteration of the bronchiole |
|
|
In what ways can you classify pneumonia |
Morphological (bronchopneumonia, interstitial, embolic or granulomatous) - Can add further descriptive terms to describe distribution (e.g. cranioventral), colour, exudation (e.g. suppurative) or texture. Aetiological - based on what caused it (toxic, bacterial, viral, parasitic, fungal etc) |
|
|
Define bronchopneumonia. What do you see histologically? |
o Inflammation initially centred on terminal bronchioles with extension into alveolio Microscopically see neutrophils and necrotic cell debris within bronchioles and alveoli
|
|
|
Describe the gross pathology of interstitial pneumonia |
Lungs appear normal on post-mortem. However, on palpation they will be abnormally firm. The lesions are diffuse. |
|
|
Describe the appearance and texture of Embolic pneumonia |
Multifocal, random, firm nodules. Colour depends on chronicity of the lesion |
|
|
What are some sequelae of bronchopneumonia? |
Pleural adhesions, lung abscesses, bronchiectasis
|
|
|
What is usually the cause of interstitial pneumonia (be broad)? |
o Usually associated with viral infectionso Also caused by protozoal infections, sepsis and toxic gases
|
|
|
What are the 2 main causes of embolic pneumonia |
Tumour metastases or septic emboli |
|
|
What are some causes of granulomatous pneumonia? |
Mycobacterium, systemic mycoses or dead parasites and their ova
|
|
|
Define Bovine enzootic pneumonia |
• Broad and ill-defines entity characterised by infectious respiratory disease affecting young cattle (<6 months)• Usually related to stress, environmental conditions and compromised host defences• Etiology includes interactions amongst a variety of viral and bacterial pathogens
|
|
|
Describe the clinical presentation of pneumonic mannheimiosis (shipping fever)? |
• Usually affects cattle > 6 months old and <2 years old• Presents as numerous animals suddenly developing respiratory signs within a few weeks of a transport event. On PM you will see an acute fibrinous pneumonia with a cranioventral distribution
|
|
|
What lesions and clinical signs would you see with bovine tuberculosis? |
Gross lesions include chronic, caseating granulomas in lung, retropharyngeal and tracheobronchiallymph nodes, and in other organs. Lesions may erode through the pleural and implant on pleuralsurfaces |
|
|
What parasite is most commonly associated with pneumonia in cattle in NZ? |
Dictyocaulus Viviparous |
|
|
What are some potential sequelae to M.Wolfii infection in cattle? |
Placentitis, abortion or fatal embolic pneumonia |
|
|
Describe the mechanism of 'Fog fever' |
Cattle grazing pasture rich in L-Tryptophan. L-Tryptophan is metabolised in the rumen to 3-methylindole. This is absorbed into the blood and transported tot he lungs. Here it is metabolised by clara cells (non-ciliated bronchiolar secretory cells) into a highly pneumotoxic compound. This causes extensive necrosis of bronchiolar epithelium and type I pneumocytes (diffuse alveolar damage) |
|
|
What are 3 causes of rhinitis in sheep? |
Viral rhinitis (OAV, OPIV, ORSV), Oestrus Ovis and enzootic nasal tumours |
|
|
What are the consequences of ovine enzootic pneumonia |
• Rarely fatal but causes reduced weight gain and carcass downgrading• May predispose to pulmonary abscessation or acute pneumonia later in life following stress
|
|
|
What do pleural adhesions indicate? |
The respiratory disease is chronic |
|
|
What is the pathogenesis of acute fibrinous pneumonia in sheep? |
· Severe stress allows bacteria to multiply and produce toxins resulting in pulmonary necrosis and toxaemia
|
|
|
Describe the transmission and lesions of lentiviral pneumonias in sheep and goats |
o Major method of disease spread is via colostrumintake
Lesions include slow progressive pneumonia, encepahlitis, arthritis and mastitis. Lungs on PM will be pale, heavy and firm, they wont collapse on opening of the chest |
|
|
Come up with a list of differentials for pneumonia in a cat |
o Viral – feline calicivirus
o Bacterial – Pasteurella Multicida (secondary to viral infections) o Mycotic – Cryptococcus Neoformans o Parasitic – Aleurostrongylus Abstrusus, Paragonimus Kellicotti, Toxoplasma Gondii (causes liver lesions and interstitial pneumonia) o Other – feline asthma, interstitial pneumonia |
|
|
What are some common causes of pneumonia in a foal? |
Meconium aspiration Hyaline membrane disease Equine herpesvirus Septicaemia
|
|
|
Describe the most common primary pulmonary neoplasm of horses |
Granular cell tumour: o Grossly the mass is white to beige, multinodular and associated with the large bronchi |
|
|
Describe the ovine enzootic nasal tumours |
o Viral adenomas and carcinomas caused by ENTV-1 and ENTV-2. Virus closely related to the ovine pulmonary adenocarcinoma viruso Tumours can arise unilaterally or bilaterally; they originate from the ethmoid turbinates and often expand to occlude the nasal cavity
|
|
|
What is the most common lungworm of sheep and what lesions does it leave? |
Muellerius Capillaris: Gross lesions are characterised by 1-20mm subpleural nodules in the dorsal regions of the caudal lobes |
|
|
What is PRDC? |
Porcine Respiratory Disease Complex Results from a combination of infectious agents and environmental stressors. Pathogens overwhelm the respiratory defences causing decreased production and increased mortality. PRDC also predisposes the pigs to secondary infections. |
|
|
Outline the differences between Atrophic and Inclusion body rhinitis in pigs |
Atrophic rhinitis occurs in pigs 5-8 months of age, while inclusion body rhinitis occurs in pigs less than 5 weeks of age. Atrophic rhinitis is caused by Pasteurella Multicida type D. Its colonisation of the nasal mucosa is predisposed to by concurrent infection from a variety of bacteria. Inclusion body rhinitis is caused by suid herpesviru. Both cause coughing and sneezing. |
|
|
What are the 3 main clinical presentation of PRRS? |
o Reproductive failureo Primary viral pneumonia in neonateso Predisposes to bacterial pneumonia and septicaemia in nursery-grower-finisher pigs
|
|
|
What lesions in the respiratory tract does PMWS cause? |
As the disease is caused by a virus that travels in the blood, the inflammation is centred on the interstitium resulting in a granulomatous interstitial pneumonia. It also predisposes the pig to bacterial pneumonia and septicaemia |
|
|
What lesions (gross and histological) and clinical signs are caused by Mycoplasma Hyopneumoniae |
Gross Lesions: include cranioventral lobular pattern of bronchopneumonia Histological Lesions: lymphocyticcuffing of airways Clinical Signs: • Chronic cough and reduced growth rates• Reduced mucociliary clearance and impaired macrophage function may lead to fatal bacterial pneumonias (so it sort of acts like a virus). It also exacerbates duration and severity of PRRS. |
|
|
What kind of pneumonia and pleuritis does Actinobacillus Pleuropneumoniae cause? |
Middle/caudal lobe bronchopneumonia and fibrinous pleuritis with pleural adhesions
|
|
|
How can you diagnose Fungal rhinitis in dogs? What is the prognosis? |
Diagnose with clinical signs – sneezing, chronic, purulent or haemorrhagic discharge. You can also do a nasal wash for cytology. Should be able to see Apergillus Fumigatus. Difficult to treat; guarded prognosis
|
|
|
What infectious agents usually cause rhinitis in dogs? What about in cats? |
• Dogs: Canine distemper virus, Canine adenovirus, Canine parainfluenza virus or Aspergillus Fumigatus
• Cats: Feline herpesvirus 1, Feline calicivirus, Chlamydophila Felis or Cryptococcus Neoformans |
|
|
What's bad about Brachycephalic Airway Syndrome in dogs? |
Increased air-flow resistance caused by stenotic nostrils and nasal meatuses and an excessively long soft palate. • Secondarily changes, such as laryngeal and nasal oedema may lead to upper airway obstruction, respiratory distress and exercise intolerance.
|
|
|
What breed of dog is most predisposed to tracheal collapse |
Toy Poodles (and other toy breeds) |
|
|
What is Feline Asthma, what are its clinical signs and how can you diagnose it? |
• Clinical syndrome characterised by recurrent episodes of bronchoconstriction, coughing or dyspnoea. • Most likely to be the result of a chronic allergic response (type I hypersensitivity)
Clinical signs – coughing, wheezing, severe expiratory dyspnoea Diagnosis • Broncho alveolar washes- eosinophils tend to be the predominant cell type |
|
|
What are the 4 types of pleural disease in cats? |
1- Feline Infectious Peritonitis 2- Pyothorax 3- Hydrothorax 4- Chylothorax |
|
|
What is a Ethmoid Haematoma? What kinds of horses are usually affected |
• Slow growing tissue proliferation that arises from the ethmoid turbinate region• More common in older horses (Thoroughbred and Arabians)
|
|
|
What are some potential sequelae of a fungal infection of the guttural pouches |
- Guttural Pouch Empyema - Epistaxis - Dysphagie - Horner's Syndrome (roaring) - Fatal Haemorrhage (carotid artery) |
|
|
What are the clinical signs of Strangles? |
Purulent nasal discharge, swollen submandibular and retropharyngeal lymph nodes, depression and fever
|
|
|
Serious complications occur in 20% of horses affected by Streptococcus Equi (strangles), what are they? |
o Pneumonia or pleuropneumoniao Myocarditiso Mesenteric lymph node abscesses (Bastard Strangles)o Pupura Haemorrhagica (1-2% of the cases)
|
|
|
What lesions does Rhodococcus Equi cause in foals? |
• Causes ulcerative enterocolitis, arthritis and osteomyelitis in addition to pyogranulomatous bronchopneumonia and infection of other organs
|
|
|
What lesions (gross and histological) do you find in Chronic Obstructive Pulmonary Disease (Heaves) |
Gross Lesions Heave line (hypertrophy of the external abdominaloblique), lungs fail to collapse, may have rib impressionsand appear overinflated and pale. Hypersensitivity-mediated neutrophilic airway inflammation and lower airway obstruction. In some cases, emphysema and bronchiectasis maybe present. Histological Lesions o Intraluminal neutrophilso Bronchiolar Epithelial Hyperplasiao Goblet cell Metaplasiao Mucus hypersecretiono Peribronchiolar lymphoid cell infiltrationo Peribronchiolar fibrosis |
|
|
What is the pathogenesis of exercise induced pulmonary haemorrhage in horses? |
o Stress failure of the pulmonary capillaries caused by excessive transmural pressure created by very high intracapillary pressure (predominantly caused by high blood pressure) and low intraalveolar pressure (generated by a negative intrapleural pressures associated with inspiration) produced during exercise
|