![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
279 Cards in this Set
- Front
- Back
|
This is difficult or labored breathing.
|
Dyspnea |
|
|
What are the 4 categories of dyspnea? |
Severe dyspnea -Use of accessory muscles of respiration Dyspnea on exertion -shortness of breath with activity Platypnea -Dysnea when lying down Paraxymal nocturnal dyspnea -Awaking at night and gasping for air; must sit up or stand up. |
|
|
This is a protective reflex that helps clear the airway. |
Cough Acute-resolves within 2-3 weeks Chronic-Lasts longer than 3 weeks |
|
|
Define hemoptysis |
Hemoptysis is the coughing up of blood or bloody sputum from the lungs or airway.
|
|
|
This is a normal breathing pattern. |
Eupnea |
|
|
What are abnormal breathing patterns? |
-Adjustments to minimize the work of the respiratory muscles -Kussumal respirations -deep and labored breathing pattern often associated with severe metabolic acidosis, particularly diabetic ketoacidosis (DKA) but also kidney failure -labored breathing (work hard to breath) -restricted breathing -disorders that stiffen the lungs or chest wall and decrease compliance) -Cheye-strokes respirations -progressively deeper and sometimes breathing, followed by a gradual decrease that results in a temporary stop in breathing (apnea) before repeating. |
|
|
describe the difference between hypoventilation and hyperventilation |
Hypoventilation -Alveolar ventilation is adequate in relationship to the metabolic demands. -Leads to respiratory acidosis from hypercapnia -Is caused by airway obstruction, chest wall restriction, or altered neurlogic control of breathing. Hyperventilation -Alveolar ventilation exceeds the metabolic demands -Leads to respiratory alkalosis from hypocapnia -Caused by anxiety, head injury, or severe hypoxemia |
|
|
Whats the difference between central and peripheral cyanosis? |
Peripheral cyanosis -Most often caused by poor circulation -Best observed in nail beds Central Cyanosis -Caused by decreased arterial oxygenation -Best observed in buccal mucous membranes and lips |
|
|
Whats the difference between pleural pain and chest wall pain? |
Pleural pain -Is the most common pain caused by pulmonary diseases. -Is usually sharp or stabbing in character. -Infection and inflammation of the parietal pleura (pleuritis or pleurisy) causes pleura stretching or a friction rub Chest wall pain -May be from the airway -May be from muscle or rib pain |
|
|
This is excessive carbon dioxide in the bloodstream, typically caused by inadequate respiration.
|
Hypercapnia |
|
|
This is an abnormally low concentration of oxygen in the blood.
|
Hypoxemia caused by -Low arterial oxygen or -Ventilation-perfusion abnormalities: Most common causes -Shunting -Alveolar dead space: Area where alveoli are ventilated but not perfused |
|
|
This occurs when fluid builds up in the air sacs in your lungs. When that happens, your lungs can’t release oxygen into your blood. In turn, your organs can’t get enough oxygen-rich blood to function. You can also develop acute respiratory failure if your lungs can’t remove carbon dioxide from your blood (hypercapnia).
|
Acute respiratory failure -ph _<7.25 -Requires ventilatory support, oxygen, or both |
|
|
What is chest wall restriction? |
-Chest wall deformed, traumatized, immobilized, or made heavy by fat; work of breathing is increased, and ventilation may be compromised because of a decease in tidal volume. -Impaired respiratory muscle function is caused by neuromuclular disease. |
|
|
The presence of air or gas in the cavity between the lungs and the chest wall, causing collapse of the lung.
|
pnumothorax |
|
|
What are the 3 different categories of pneumothorax? |
Primary (spontaneous) pneumothorax -Occurs unexpectedly in healthy individuals Secondary pneumothorax -Is caused by disease, trauma, injury, or condition Iatrogenic pnuemothorx -Is caused by medical treatments, especially transthoracic needle aspiration. |
|
|
What are the clinical manifestations and treatments for pneumothorax? |
Clinical manifestations -Sudden pleural pain, tachypnea, and possible mild dyspnea Treatment -chest tube -If persistent air leak: Surgery, pleurodosis (instillation of a caustic substance, such as taic, into the pleural space) |
|
|
This is the build-up of excess fluid between the layers of the pleura outside the lungs.
|
Pleural effusion |
|
|
What are the 3 different categories of plerual effusion? |
Transudative effusion -Is watery and diffuses out of the capillaries Exudative effusion -Is less watery and contains high concentrations of white blood cells and plasma protiens Hemothorax -Blood effusion |
|
|
What are the clinical manifestations and treatments for Pleural effusion? |
Clinical manifestations -Dyspnea Pleural pain Treatment -Thoracentesis -Chest tube -Surgery |
|
|
Define aspiration, its clinical manifestations and treatment. |
Aspiration occurs when there is a passage of fluids and solid particles into the lungs (right lower lung is the most frequent site). Clinical manifestations -Both chocking and intractable cough have a sudden onset. Treatment -Supplemental oxygen -Restrict fluids to decrease blood volume and minimize pulmonary edema. -Administer steroids during the first 72 hours after aspiration -May need broad-spectrum antibiotics |
|
|
Partial or complete collapse of the lung.
|
Atelectasis |
|
|
What are the 2 categories of atelectasis? |
Compression atelectasis -External compression of the lungs Surfactant impairment -Decreased production or inactivation of surfactant |
|
|
What are the clinical manifestations and treatment for atelectasis? |
Clinical manifestation -Dyspnea -Cough -Fever -Leukocytosis Treatment: Prevention -Deep breathing |
|
|
Define bronchiolitis and who is susceptible? |
The inflammation of small airways or bronchioles -Most common in children -Occurs in adults with chronic bronchitis or those with a viral infection or who have inhaled toxic gases. |
|
|
What are the clinical manifestations and treatments of bronchiolitis? |
Clinical manifestations -Rapid ventilatory rate -significant use of accessory muscles -low-grade fever -dry, nonproductive cough -Hyperinflated chest Treatment -Antibiotics -Steroids -Chest physical therapy (Humidified air, coughing and deep breathing, postural drainage) |
|
|
This is a disease in which tissue deep in your lungs becomes thick and stiff, or scarred, over time. |
Pulmonary fibrosis |
|
|
What are the different types of pulmonary fibrosis and the clinical manifestations associated and treatments associated with them with them? |
Idiopathic pulmonary fibrosis (no specific cause) -Clinical manifestations: increasing dyspnea on exertion -Treatment: Corticosteriods, antibiotic drugs, interferon, and anticoagulant agents; lung transplants. Pulmonary fibrosis due to Exposure to toxic gases (e.g. ammonia, hydrogen chloride, sulfur dioxide) -Clinical manifestations: Burning of the eyes, nose, and throat; coughing; chest tightness; dyspnea; hypoxemia. -Treatment -Supplemental oxygen, mechanical ventilation -Steroid administration; effectiveness has not been well documented |
|
|
Explain oxygen toxicity? |
Oxygen toxicity is a condition resulting from the harmful effects of breathing molecular oxygen (O. 2) at increased partial pressures. It is also known as oxygen toxicity syndrome, oxygen intoxication, and oxygen poisoning. -Prolonged exposure to high concentrations of supplemental oxygen. -Severe inflammatory response mediated primarily by oxygen radicals -Causes damage to alveolocapillary membranes, disruption of surfacant production, interstitial and alveolar edema, and decrease in compliance. |
|
|
Whats the treatment for oxygen toxicity? |
-Ventilatory support and reduction of inspired oxygen concentration to less than 60% as soon as tolerated. |
|
|
Define pneumoconiosis |
Any changes in the lungs caused by the inhalation of inorganic dust particles, usually from the workplace. |
|
|
What are the clinical manifestations and treatment(s) for pneumoconiosis? |
Clinical manifestations -Cough -sputum production -Dysnea -Decreased lung volumes -Hypoxemia Treatment -Palliative and prevention of further exposure -Improve working conditions -Pulmonary rehabilitation and management of hypoxemia |
|
|
What are the common causes for pneumoconisis? |
-Silicosis: is caused by the inhalation of free silica (silicon dioxide) and silica-containing compounds as occurs in mining (no cure) -Coal worker pneumoconiosis (Coal miner's lung, black lung): is caused by coal dust deposits in the lung (no specific cure). -Asbestosis: Asbestos exposure affects not only factory workers but it affects individuals who live in areas of asbestos emission (supportive treatment) |
|
|
This refers to the antigen-antibody reaction and inflammation of the tiny air sacs in the lungs where oxygen and CO2 are exchanged, the alveoli.
|
Allergic alveolitis -can be either acute, subacute and chronic Treatment -Avoidance of the offending agent -Corticosteroid administration |
|
|
This is a condition caused by excess fluid in the lungs. This fluid collects in the numerous air sacs in the lungs, making it difficult to breathe. In most cases, heart problems cause this.
|
Pulmonary edema -Common cause: Left sided heart disease |
|
|
What are the clinical manifestations of pulmonary edema? |
Clinical manifestations -Dyspnea -Orthopnea (dyspnea when lying down) -Hypoxemia -Increased work of breathing |
|
|
What is acute lung injury (ALI) or acute respiratory distress syndrome (ARDS)? |
-Forms of respiratory failure characterized by acute lung inflammation and diffuse alveolocapillary. -Injury to the pulmonary capillary edothelium -Increased capillary permeability -Surfactant inactivation -Edema and atelectasis |
|
|
What are the 3 phases of acute lung injury? |
Exdudative or inflammatory -within 72 hours -Alveolocapillary membrane damage -Increased capillary membrane permeability -Pulmonary edema -Surfactant inactivated Proliferation -4 to 21 days -Resolution of the pulmonary edema and proliferation of type II pneumocytes, fibroplasts, and myofibroblasts -Hyaline membranes -Hypoxia Fibrotic -14 to 21 days -Remodeling and fibrosis -Alveoli destruction -Severe destruction right-to-left shunting -Acute respiratory failure |
|
|
What are the clinical manifestations and treatment(s) for acute lung injury (ALI)? |
Clinical manifestations -Dypnea and hypoxemia with poor response to oxygen supplementation then.. -Hyperventilation and respiratory alkalosis then... -Decreased tissue purfusion, metabolic acidosis, and organ dysfunction then... -Increased work of breathing, decreased tidal volume, and hypoventaliation then... -Hypercapnia, respiratory acidosis, and worsening hyoixemia then... -Decreased cardiac output, hypotension, death Treatment -Mechanical ventilation with high oxygen concentrations -Low-dose steroids administration |
|
|
What are the clinical manifestations o obstructive pulmonary disease? |
-Increased work of breathing -Ventilation-perfusion mismatching -Decreased forced expiratory volume |
|
|
This is a respiratory condition marked by spasms in the bronchi of the lungs, causing difficulty in breathing. It usually results from an allergic reaction or other forms of hypersensitivity.
|
Asthma |
|
|
Explain the patho of early and late asthmatic responses |
Early asthmatic response -Immunoglobulin (IgE) causes the mast cells to degranulate, releasing a large number of inflammatory mediators -Vasodilation causing inflammation -Increased capillary permeability -Mucosal edema -Bronchial smooth muscle contraction (bronchospasm) -Mucous secretion Late asthmatic response -Begins 4-8 hours after the early response -Chemotatic recruitment of lymphocytes, eosinophils, and neutrophiles occurs -Prolonged smooth muscle contraction -Airways scarring -Impaired mucociliary function with accumulation of mucous cellular debris, forming plugs in the airways -Leads to airway remodeling if left untreated -Airway trapping -Hyperinflation distal to obstructions -Increased work of breathing -Hypoxemia |
|
|
What are the clinical manifestations and treatments for asthma? |
Clinical manifestations -Asymptomatic between attacks -Chest contrsutions, expiratory wheezing, dyspnea, nonproductive coughing, prolonged expiration, tachycardia, tachypnea -Status asthmaticus Treatment -Immediate administration of oxygen and inhaled beta-agonist bronchodilators -Oral corticosteroids adminisretation early -Education over allergens and irritants |
|
|
Define chronic obstructive pulmonary disease |
Its a lung disease characterized by chronic obstruction of lung airflow that interferes with normal breathing and is not fully reversible. The more familiar terms 'chronic bronchitis' and 'emphysema' are no longer used, but are now included within the COPD diagnosis.
-not reversible -usually progressive ans associated with an abnormal inflammatory response of teh lung to noxious -chronic bronchitis + emphysema |
|
|
What are the risk factors for COPD? |
-Tobacco smoke -Occupational dusts and chemicals -Indoor air pollution from cooking and heating -Outdoor air pollution -Any factor that affects lung growth during gestation and childhood -Genetic susceptibilities -Inherited mutations in the alpha-1antrypsin gene results in the development of emphysema even in nonsmokers |
|
|
This is a chronic inflammatory condition in the lungs that causes the respiratory passages to be swollen and irritated, increases the mucus production and damages the lungs. The symptoms are coughing and breathlessness, which will get worse over the years
|
Chronic bronchitis |
|
|
Describe the patho of chronic bronchitis |
-Inspired irritants increase mucous production, size, and number of mucous glands, and bronchial edema (mucous is thicker that normal) -Hypertrophied bronchial smooth muscle -Hpoxemia and hypercapnia -Airway collapse early in expiration, trapping gas in the lung |
|
|
What are the clinical manifestations and treatment for chronic bronchitis? |
Clinical manifestations -Decreased exercise tolerance and shortness -Productive cough ("smoker's cough) becomes copious -Polycythemia Treatment -Smoking cessation -Bronchodilators, expectorants -Chest physical therapy -Antibiotics, steroids -Mechanical ventilation, oxygen therapy |
|
|
This is abnormal permanent enlargement of the gas-exchange airways accompanied by the destruction of the alveolar walls without obvious fibrosis. Also causes loss of emphysema. |
Emphysema |
|
|
Whats the difference between primary and secondary emphysema? |
Primary -Inherited deficiency of the enzyme alpha 1-antitrypsin Secondary -Cigarette smoking (main cause) -Air pollution, occupational exposures, and childhood respiratory infections (possible contributors) |
|
|
Explain the pathophysiology of emphysema |
-Destruction of alveoli occurs through the breakdown of elastin in the septa -Alveolar destruction also produces large air spaces within the lungs parenchyma (bullae) and air spaces ajacent to pleurae (blebs). https://www.youtube.com/watch?v=OiSTT4z4zJI |
|
|
What are the clinical manifestations and treatments for emphysema? |
Clinical manifestations -Dyspnea on exertion progressing to constant dyspnea -Little coughing and very little sputum -Tachypnea with prolonged expiration; use of accessory muscles for ventiliation; pursed lips -increased anteroposterior diameter of the chest (barrel chest) -Leans forward with arms extended and braced on knees when sitting to increase lung capacity Treatment -Oxygen; may require mechanical ventilation -Inhaled bronchodilators-anticholinergic agents and beta agonists -Corticosteroids and antibiotics -Smoking cessation -Pulmonary rehabilitation -breathing techniques |
|
|
Define pnemonia |
lung inflammation caused by bacterial or viral infection, in which the air sacs fill with pus and may become solid.
|
|
|
What are the different types of pneumonia? |
Community-acquired pneumonia -Streptococcus pneumonia (most common) -Mycoplasma (walking pneumonia), Legionella Hospital acquired (nosocomial) pneumonia Ventilator-associated pneumonia -Pseudomonas, Staph aureus, Klebsiella Viral pneumonia -is seasonal; usually mild and self-limiting -Can set the stage for secondary bacterial infection -Damages ciliated epithelial cells, which normally prevent pathogens from reaching the lower airways -Most common form: Influenza |
|
|
What are the clinical manifestations and treatment(s) for pneumonia? |
Clinical manifestations -Preceded by an upper respiratory infection -Cough, dyspnea, and fever -Chills, malaise, and pleuritic chest infections Treatment -Prevention -Prevention of aspiration -Vaccination for appropriate populations -Adequate ventilation and oxygenation -Bacterial pneumonia;antibiotics -Viral pneumonia: supportive therapy -severe cases: antiviral medications |
|
|
What is tuberculosis? |
an infectious bacterial disease characterized by the growth of nodules (tubercles) in the tissues, especially the lungs.
-Infection caused by Mycobacterium tuberculosis, an acid-fast bacillus -Leading cause of death from a curable infectious disease throughout the world |
|
|
Describe the pathophysiology of tuberculosis |
-Airborne droplet transmisson -Tubercle formation: Granulomatous lesion -Caseous necrosis: cheese-like material -May remain dormant for life or cause active disease -Isolation of bacili by enclosing them in tubercles and surrounding the tubercles with scar tissue |
|
|
How is tuberculosis diagnosed? |
-Postive TB skin test -Sputum culture, immunoassays -Chest radiographs |
|
|
What are the clinical manifestations and treatments for tuberculosis? |
Clinical manifestations -Latent tuberculosis infection: asymptomatic -Fatigue, weight loss, lethargy, anorexia (loss of appetite), a low-grade fever that usually occurs in the afternoon, and night sweats; purulent cough Treatment -Isoniazid, rifampin, pyrazinamide, and ethambutol -Use in combination for drug-resistance bacilli |
|
|
What is abscess in the lungs? |
Lung abscess is a type of liquefactive necrosis of the lung tissue and formation of cavities (more than 2 cm) containing necrotic debris or fluid caused by microbial infection. This pus-filled cavity is often caused by aspiration, which may occur during altered consciousness.
|
|
|
What are the clinical manifestations and treatments for lung abscess? |
Clinical manifestations -Fever, cough, chills, sputum production, and pleural pain -Bronchus involvement; Severe cough, copious amounts of often foul-smelling sputum, and occasionally hemoptysis Treatment -Antibiotics -Chest therapy, including chest percussion and postural drainage -Bronchoscopy: To drain the abscess |
|
|
What is acute bronchitis? |
-Its an acute infection or inflammation of airways or bronchi; commonly follows a viral illness -Causes symptoms similar to pneumonia but does not demonstrate pulmonary consolidation and chest infiltrates. |
|
|
What are the clinical manifestations and treatment(s) of acute bronchitis? |
Clinical manifestations -Nonproductive cough occurs in paroxysms and is aggravated by cold, dry, or dusty air Treatment -Rest -Aspirin -Humidity -Cough suppressant (codeine) |
|
|
This is a blockage in one of the pulmonary arteries in your lungs. In most cases, pulmonary embolism is caused by blood clots that travel to the lungs from the legs or, rarely, other parts of the body (deep vein thrombosis).
|
Pulmonary embolism |
|
|
Explain the pathophysiology of a pulmonary enbolism |
-Release of neurohumoral (a process by which a presynaptic cell, on excitation, releases a specific chemical agent (a neurotransmitter) to cross a synapse to stimulate or inhibit the postsynaptic cell) substance and vasocontristion -Atelectasis of the affected lung segments and hypoxemia. -Pulmonary edema, pulmonary hypertention, shock, and even death |
|
|
What are the clinical manifestations, treatments, and preventions of a pulmonary embolism? |
Clinical manifestations -Sudden onset of pleuritic chest pain, dyspnea, tachypnea, tachycardia, and unexplained anxiety Treatment -Oxygen and hemodynamic stabilization with fluids -Anticiagulation and/or fibrinolytic agent (streptokinase) Percutaneous or surgical embolectomy Prevention -Bed exercises, frequent position changes, early ambulation, and pneumatic calf compression -Prophylactic anticoagulation -Filter in the inferior vena cava |
|
|
What is pulmonary artery hypertension (PAH) ? |
Pulmonary hypertension is a type of high blood pressure that affects the arteries in your lungs and the right side of your heart. In one form ofpulmonary hypertension, tiny arteries in your lungs, called pulmonaryarterioles, and capillaries become narrowed, blocked or destroyed
|
|
|
What are the causes, clinical manifestations and treatments for pulmonary artery hypertension (PAH)? |
Causes -Elevated left ventricular pressure -Increased blood flow through the pulmonary circulation -Obstruction of the vascular bed or constriction of the vascular bed produced by hypoxemia or acidosis Clinical manifestations -Masked by primary pulmonary or cardiovascular disease -First indication: Chest radiography (enlarged pulmonary arteries and right heart border) or an electrocardiogram that shows right ventricular hypertrophy Treatment -Oxygen, diuretics, anticoagulants -Lung transplantation -Secondary pulmonary hypertension -Treats the primary disorder -Once hypertrophy to develops, it is no longer reversible -Supplemental oxygen reverses hypoxic vasoconstriction |
|
|
This is an abnormal enlargement of the right side of the heart as a result of disease of the lungs or the pulmonary blood vessels.
|
Cor pulmonale -Pulmonary hypertension, creating chronic pressure overload in the right ventricle |
|
|
What are the clinical manifestations and treatments for cor pulmonale? |
Clinical manifestations -Heart appears normal at rest -With exercise: Decreased cardiac output, chest pain Treatment -Decreased workload of the right ventricle by lowering pulmonary artery pressure -Same as for PAH -Oxygen, diuretics, anticoagulants -Lung transplantation -Reversal of the underlying lung disease |
|
|
What are the risk factors, clinical manifestations and treatments for laryngeal cancer? |
Risk -Tobacco smoke -Heightened with smoking and alcohol consumption -Gastroesophageal reflux disease -HPV Clinical manifestations -Hoarseness -Dyspnea -Cough Treatment -Combined chemo and radiation -Photodynamic therapy -Partial or total laryngectomies |
|
|
What are the 3 major types of lung cancer? |
Non-small-cell lung cancer -about 85% of all lung cancers -Squamous cell carcinoma -Ademocarcinoma Neuroendocrine -Approximately 14% of all lung cancers -Small cell carcinoma: most common -Worst prognosis Mesotheliomas -Associated with asbestos -May take 20-40 years before cancer appears -Clinical manifestaions -Dyspnea and chest pain -Treatment -Pleuropneumonectomy, chemo, radiation and |
|
|
Kidney stones are also called what? |
Renal calcui or urolithiasis |
|
|
What are kidney stones? |
-Masses of crystals, proteins, or mineral salts that form in the urinary tract and may obstruct the urinary tract. -Composition of mineral salts -Calcium oxalate and calcium phosphate: 70% - 80% -Struvite (magnesium, ammonium, phosphate): 25% -Uric acid: 7% |
|
|
What are the risk factors, clinical manifestations and treatments of kidney stones? |
Risk factors -Male, most develop before 50 -Inadequate fluid intake: most prevalent -Diet -Genetic disorders of amino acid metabolism Clinical manifestations -Renal colic (pain) Treatment -Parenteral and/or oral analegesics for acute pain -Medical therapy that promotes stone passage (alpha-antagonists or calcium channel blockers) -High fluid intake -Alteration in urine pH -removal of stones using percutaneous nephroithotomy, ureterscopy, or ultrasonic or laser lithotripsy to fragment stones for excretion |
|
|
What are neurogenic bladder disorders? |
Neurogenic bladder is bladder dysfunction (flaccid or spastic) caused by neurologic damage. Symptoms can include overflow incontinence, frequency, urgency, urge incontinence, and retention. Risk of serious complications (eg, recurrent infection, vesicoureteral reflux, autonomic dysreflexia) is high.
|
|
|
Whats the difference between upper motor neuron and lower motor neuron neurogenic bladder disorders? |
Upper motor -Dyssynergic: overactive or hyperreflexive bladder function -Detrusor hyperreflexia: Uninhibited or reflex bladder -Both the bladder and the sphincter are contracting at the same time, causing a functional obstruction of the bladder outlet Lower motor neurons -Detrusor areflexia: Underactice, hypotonic, or atonic bladder |
|
|
What are the causes , clinical manifestations and treatment(s) of a neurogenic bladder disorder? |
Causes -Prostate enlargement -Urethral stricture -Severe pelvic organ prolapse -Low bladder wall compliance Clinical manifestations -Frequent daytime and night-time (nocturia) voiding -Urgency with intermittency of urinary stream -Dysuria -Feeling of incomplete bladder emptying Treatment -Detrusor sphincter -alpha-adrenergic blocking (antimuscarinic) medications or botulinum toxin -Intermittent catheterization -Obstruction -Medications -Bladder neck incision -Low bladder wall compliance -Antimuscarinic drugs and intermittent catheterization -Enlargement of bladder wall using a piece of small bowel -Urethral stricture -Urethral dilation with a steel instrument |
|
|
This is a chronic syndrome of the detrusor over-activity. People usually experience urgency, often associated with frequency and nocturia. |
Overactive bladder syndrome Treatment -Behavioral therapy, neuro-modulation -Pharmacotherapy (antimuscarinic agents); Botulium toxin therapy; surgery |
|
|
What are the 3 different types of renal tumors? |
-Renal adenomas :benign -Renal transitional cell carcinoma: Rare -Renal cell carcinoma: most common |
|
|
What are the clinical manifestations and treatment(s) for renal tumors? |
Clinical manifestations -Hematuria -Dull and aching flank pain Treatment -Surgical removal of the affected kidney (radical nephrectomy) or partial nephrectomy -Surgery, chemo & radiation |
|
|
What is the most common bladder tumor? |
Urothelial (transitional cell) carcinoma |
|
|
What are the clinical manifestations and treatment for bladder tumors? |
Clinical manifestations -Painless microscopic hematuria Treatment -Transurethral resection or laser ablation -Radical cystectomy with urinary diversion -Adjuvant chemo and radiation |
|
|
What are the risk factors for bladder tumors?
|
-Smoking -Exposure to dyes or other aromatic amines or chemicals -High arsenic in drinking water -Heavy consumption of phenacetin |
|
|
What is a UTI? |
A urinary tract infection (UTI) is an infection in any part of your urinary system — your kidneys, ureters, bladder and urethra. Most infections involve the lower urinary tract — the bladder and the urethra. Women are at greater risk of developing a UTI than men are. -Inflammation of the urinary epithelium after invasion and colonization by some pathogen in the urinary tract -Retrograde movement of bacteria into the urethra and bladder |
|
|
What are the classifications of UTIs? |
-Cystitis: Bladder inflammation
-Pyelonephritis: Inflammation of upper urinary tract |
|
|
What are the protective measures against UTIs? |
Protective urinary mechanisms
-Washed out of the urethra during micturition -Low pH and high osmolality of urea |
|
|
What are the common pathogens that cause a UTI? |
-Escherichia coli
-Staphylococcus saprophyticus |
|
|
What are the virulence factors of the following uropathogens -Fimbriae -Biofilms |
Fimbriae: Adherence to the uroepithelium
Biofilms: Resist host’s defense mechanisms |
|
|
This is a inflammation of the urinary bladder. It is often caused by infection and is usually accompanied by frequent, painful urination.
|
Cystits |
|
|
What are the clinical manifestations, evaluation characteristics, and treatment(s) for cystitis? |
Clinical manifestations
-Asymptomatic -Frequency, dysuria, urgency, and low back and/or suprapubic pain Evaluation -Urine culture of specific microorganisms with counts of 10,000/ml or more Treatment -Antimicrobial therapy |
|
|
This is an acute infection of the ureter, renal pelvis, and/or renal parenchyma
|
Acute pyelonephritis |
|
|
What are the clinical manifestations, evaluation characteristics and treatment(s) of pyelonephritis? |
Clinical manifestations
-Flank pain -Fever, chills -Costovertebral tenderness -Purulent urine Evaluation -White blood cell casts, indicating pyelonephritis Treatment -Antibiotic administration |
|
|
What happens when an individual has pyelonephritis foe a while? An how is chronic pyelonephritis treated? |
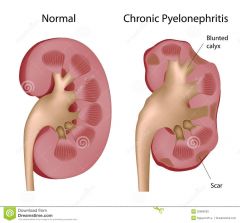
-Persistent or recurrent infection of the kidneys, leading to scarring of the kidneys
-Inflammation and fibrosis, located in the interstitial spaces between the tubules, leading to chronic kidney failure Treatment -Antibiotic administrationProlonged antibiotics with recurrent infections |
|
|
What is acute glomerulonephritis? |
-Formation of immune complexes (antigen/antibody) in the circulation that deposit in glomerulus
-Antibodies produced against the organism that cross-react with the glomerular endothelial cells -Activation of complement -Recruitment and activation of immune cells and mediators -Decreased glomerular filtration rate (GFR) -Decreased glomerular perfusion due to inflammation -Glomerular sclerosis (scarring) -Thickening of the glomerular basement membrane, but increased permeability to proteins and red blood cells |
|
|
What are the clinical manifestations and treatment(s) for acute glomerulonephritis? |
Clinical manifestations
-Hematuria with red blood cell casts -Proteinuria -Severe or progressive glomerular disease → Oliguria(oli=few or little) (urine output <400 ml/day) Treatment Antibiotics -Corticosteroids -Cytotoxic agents -Anticoagulants |
|
|
This is excretion of 3.0 g or more of protein in urine. Protein excretion is caused as a result of glomerular injury.
|
Nephrotic syndrome |
|
|
What are the clinical manifestations and treatment(s) of nephrotic syndrome? |
Clinical Manifestations
-Hypoalbuminemia -Peripheral edema -Prone to infection Treatment -Normal-protein (1 g/kg body weight/day) and low-fat diet, salt restriction, diuretics, immunosuppression -Immunosuppressive drugs and angiotensin-converting enzyme inhibitors used when steroid-resistant |
|
|
What is nephritic syndrome? |
Its a disorder of glomeruli (clusters of microscopic blood vessels in the kidneys with small pores through which blood is filtered). It is characterized by body tissue swelling (edema), high blood pressure, and the presence of red blood cells in the urine.
|
|
|
Less than _____% of renal function remains in end-stage renal failure. |
10% |
|
|
Decline of renal function to approximately ____% of normal is considered renal insufficiency. |
25% |
|
|
Whats the difference between uremia and azotemia? |
Uremia -Syndrome of renal failure -Elevated blood urea and creatinine levels -Fatigue, anorexia, nausea, vomiting, pruritius, and neurological changes -Retention of toxic wastes, electrolyte disorders, and pro-inflammatory state Azotemia -Increased serum urea levels and frequently increased creatine levels -Renal insufficiency or renal failure, causing azotemia Both -Accumulation of nitrogenous waste products in the blood. |
|
|
This is a sudden decline in kidney function with a decrease in glomerular filtration and accumulation of nitrogenous waste products in the blood. There is also an increase in serum creatine and blood urea nitrogen. |
Acute kidney injury -has replaced the term acute renal failure |
|
|
What is oliguria? |
the production of abnormally small amounts of urine.
Due to... -Alterations in renal blood flow -Efferent arteriolar vasoconstriction -Impaired autoregulation -Tubular obstruction -Backleak-tubular reabsorption is accelerated due to permeability |
|
|
How can acute kidney injuries be prevented? |
Maintenance of fluid volume before and after surgery or diagnostic procedures or when nephrotoxic drugs or contrasts agents are used. |
|
|
What are the treatments for acute kidney injury? |
-Correct fluid and electrolyte disturbances -Certain drugs can be toxic -Hyperkalemia -Restrict dietary sources of potasium -May need dialysis -Azotemia -Adopt a low-protein, high-carbohydrate diet -Recovery may take a year |
|
|
What are the factors that cause acute kidney injury to progress into chronic kidney disease? |
Factors that advance disease -Proteinuria -Promotes inflammation and progressive fibrosis -Angiotension II -Promotes glomerular hypertension, and participates in fibrosis and scaring Factors that contribute to progression of disease -Glomerular hypertension -Inflamation |
|
|
What are the clinical manifestations of chronic kidney disease? |
-Uremic syndrome (It occurs when urea and other waste products build up in the body because the kidneys are unable to eliminate them) -Affects every body system -Cardiovascular system -Anemia: lack of erythropoietetin -Hypertension:volume overload -Dyslipedemia -Pulmonary system -Dyspnea and Kussmaul respirations -Immune system -Immune suppression -Increased risk for infection -Neurologic system -Impaired concentration and judgment -Memory loss -Seizures, coma -Gastrointestinal system -Decrease in circulating sex steroids -Insulin resistance -Low thyroid hormone levels -Integumentary system -Anemia: pallor -Bleeding: hematomas and ecchymosis -Retained urochromes: sallow (yellowish) skin color -Hyperparathyroidism and uremic skin residues (uremic frost) irritation and pruritus |
|
|
What is the treatment for chronic kidney disease? |
-Management of protein intake -Supplemental vit D -Maintenance of sodium and fluid -Restriction of potassium -Maintenance of adequate caloric intake -Management of dyslipidemias -Erythropoiein as needed -ACE inhibitors or receptor blockers: control systemic hypertension and provide renoprotection, particularly in the presence of diabetes mellitus -Dialysis -Renal transplantation |
|
|
This is a lack of desire to eat, despite physiologic stimuli.
|
Anorexia |
|
|
What can prolonged vomiting lead to? |
Can lead to fluid, electrolyte, and acid-base disturbances, hyponatremia, hypokalemia, and metabolic alkalosis
|
|
|
What are the 3 different categories of constipation? |
-Normal transit (functional) constipation: Normal rate of stool passage, but difficulty with stool evacuation from low-residue, low-fluid diet
-Slow-transit constipation: Impaired colonic motor activity with infrequent bowel movements and straining -Secondary: From an actual disease process or condition |
|
|
Whats the treatment for constipation? |
-Moderate exercise
-Increased fluid and fiber intake -Enema (should not be habitually used) -Drugs -Colonic secretagogues -For opioid-induced constipation in individuals who are terminally ill -Stool softeners and laxatives |
|
|
What are the clinical manifestations and treatments for diarrhea? |
Clinical manifestations
-Dehydration, electrolyte imbalance (hyponatremia, hypokalemia) -Metabolic acidosis and weight loss Treatment -Restore fluid and electrolyte balance -Medications: Antimotility and/or water absorbent -Mild diarrhea: Natural bran and psyllium -Clostridium difficile–associated diarrhea: Probiotics -Fecal transplantation |
|
|
What are the systemic manifestations of diarrhea? |
Acute bacterial or viral infection
-Fever, with or without cramping pain Inflammatory bowel disease -Fever, cramping pain, bloody stools Malabsorption syndromes -Staltorrhea (fat in the stools) and diarrhea |
|
|
What are the 3 different types of diarrhea? |
Osmotic
Nonabsorbable substance in the intestine draws water into the lumen by osmosis, causing large-volume diarrhea Secretory Form of large-volume diarrhea caused by excessive mucosal secretion of chloride or bicarbonate-rich fluid or the inhibition of net sodium absorption Motility Excessive motility decreases transit time, mucosal surface contact, and opportunities for fluid absorption |
|
|
Whats the difference between upper GI and lower GI bleed? |
Upper GI bleeding
-From the esophagus, stomach, or duodenum -Frank, bright red bleeding in emesis or digested blood (“coffee grounds”) in stool Lower GI bleeding -From the jejunum, ileum, colon, or rectum |
|
|
What are the clinical manifestations and treatments of GI bleeds? |
Clinical manifestaions -Hematemesis: Bloody vomit -Hematochezia: Bloody stools -Melena: Black, tarry stools -Occult bleeding: Not visible -Blood products |
|
|
What are the clinical manifestations and treatments of dysphagia? |
Clinical manifestations
-Retrosternal pain -regurgitation of undigested food -unpleasant taste -vomiting -weight loss Treatment -Eating small meals with fluid -oral medications -tube feeding -Dilation or surgical myomotomy of the lower esophageal sphincter |
|
|
This is a condition in which the muscles of the lower part of the esophagus fail to relax, preventing food from passing into the stomach.
|
Achalasia |
|
|
This is a chronic digestive disease. This occurs when stomach acid or, occasionally, stomach content, flows back into your food pipe (esophagus). The backwash (reflux) irritates the lining of your esophagus and causes this.
|
Gastroesophageal reflux disease (GERD) |
|
|
What causes GERD? And what are the evaluation prodecures done to diagnosis GERD? |
Causes -Conditions that increase abdominal pressure can contribute to GERD. -Vomiting, coughing, lifting, bending, or obesity. Evaluation -Biopsy testing for dysplastic changes |
|
|
What are the clinical manifestations and treatment(s) of GERD? |
Clinical manifestation -Heartburn from acid regurgitation, chronic cough, laryngitis -Upper abdominal pain within 1 hour of eating Treatment -Proton inhibitors: most effective -Histamine antagonists, prokinetic agents, and antacids -pain medication -Eleveate head of the bed -reduce weight -Stop smoking -Surgery: laproscopic funofercation |
|
|
What are the three different types of hiatus hernias? |
I -Most common -proximal stomach portion moves into the thoracic cavity through an opening in the diaphragm for the esophagus and vagus nerves II -Also called rolling hiatal hernia -Herniation of the greater curvature of the stomach is through a secondary opening in the diaphragm III -Combination of I and II |
|
|
What are the clinical manifestations and treatment(s) of hiatal hernias? |
Clinical manifestations -Asymptomatic -Heartburn, regurgitation, dysphagia, and epigastric pain (pain that is localized to the region of the upper abdomen immediately below the ribs) Treatment -Small, frequent meals -Avoidance of tight clothing -Weight control for obese individuals -Antacids to alleviate reflux esophagitis -Contraindicated agents (delay gastric emptying): drugs that relax the lower esophageal sphincter (anticholinergics, calcium channel blockers) -Paraesophageal: Laparoscopic surgery |
|
|
What is pyloric (gastric outlet) obstruction? |
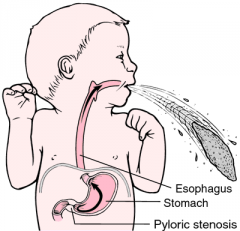
-Blocking or narrowing of the opening between the stomach and duodenum. -Acquired or congenital |
|
|
What are the clinical manifestations and treatment(s) of pyloric (gastric outlet) obstruction? |
Clinical manifestations -Epigastric pain and fullness -Nausea -Succussion splash (s a sloshing sound heard through the stethoscope during sudden movement of the patient on abdominal auscultation. It reflects the presence of gas and fluid in an obstructed organ, as in gastric outlet obstruction) -Vomiting -If prolonged: Malnutrition and dehydration Treatment -Gastric drainage; IV fluid and electrolytes -Proton pump inhibitors or histamine antagonists -Surgery or stenting |
|
|
This is obstruction or failure of normal intestinal motility. |
Intestinal obstruction and ileus |
|
|
What are the clinical manifestations and treatment(s) for intestinal obstruction and ileus? |
Clinical manifestations -SI obstruction: Colicky pains caused by intestinal distention, followed by nausea and vomiting. -LI obstruction: Hypogasteric pain and distention Treatment -Gastric or intestinal suction -Complete obstruction: immediate surgical intervention -Colonic pseudo-obstruction: Parasympathomimetic agent and colonoscopic decompression |
|
|
When talking about intestinal obstruction, what are simple and functional obstructions? |
Simple: Presence of a lesion, no impairment on the blood supply to but Functional: Failure of motility, especially after sugery |
|
|
Different types of vomitus can indicate the location of the obstruction. For the following locations, explain the type of vomitus... -Pylorus -Proximal small intestine -Lower in the small intestine |
Pylorus: Early, profuse vomiting of clear gasteric fluid. Proximal small intestine: Mild distention and vomiting of bile-stained fluid Lower in small intestine: More pronounced distention because of greater length of intestine is proximal to obstruction. Vomiting may not occur or may occur later and contain fecal material. |
|
|
Whats the most common cause of small intestinal obstruction? |
Fibrous obstruction |
|
|
Whats the most common causes of Large bowel obstruction? |
-Colorectal cancer -Volvulus (twisting of the stomach or intestines) -Strictures related to diverticulitis |
|
|
What is Acute colonic pseudo-obstruction (ogilvie syndrom)? |
Massive dilation of the large bowel; patient who are critically ill and older are immobilized. |
|
|
inflammation of the lining of the stomach.
|
Gastritis |
|
|
What are the clinical manifestations and treatment(s) for acute gastritis? |
Clinical manifestations -Abdominal discomfort -Epigastric tenderness -Bleeding Treatment -Healing usually occurs spontaneously -Discontinue injurious drugs -Administer antacids -Decrease acid secretion with a histamine antagonist and proton pump inhibitor **Acute gastritis is associate with helicobactor, NSAIDS, drugs, and chemical |
|
|
What are the clinical manifestations and treatment(s) for chronic gastritis? |
Clinical manifestations -Do not often correlate with the severity of the disease -Anorexia, fullness,nausea, vomiting, epigasteric pain, and gastric bleeding Treatment -Smaller meals; soft diet; avoidance of alcohol and NSAIDs -Administration of combination antibiotics -Vit B12: for pernicious anemia |
|
|
This is stomach inflammation caused by a reflux of bile and alkaline pancreatic secretions. |
Alkaline reflux gastritis |
|
|
What are the clinical manifestations and treatment(s) for alkaline gastritis? |
Clinical manifestations -Nausea, bilious vomiting (bile in vomit) -Sustained epigasteric pain that worsens after eating and is not relieved by antacids Treatment -Avoidance of aspirin and alcohol -Low-fat diet -Possible surgical correction |
|
|
What is peptic ulcer disease? |
-Breakdown or ulceration in the protective mucosal lining of the lower esophagus, stomach, or duodenum -Chronic vs. acute -superficial (erosion) vs. deep |
|
|
What are the risk factors for peptic ulcer disease? |
-Genetic predisposition -H. pylori infection -NSAIDs, alcohol, smoking, acute pancreatitis, COPD, pulmonary diseases, obesity, and over 65 years of age -Risks of duodenal ulcer may be reduced with a high in vit A fiber |
|
|
What are the developmental factors of duodenal ulcers? |
-Increased numbers of parietal (acid-secreting) cells -High gastrin levels -Rapid gastric emptying -Acid production caused by cigarette smoking |
|
|
What are the clinical manifestations and treatment of peptic ulcers? |
Clinical manifestations -Chronic intermittent pain in the epigasteric area -Pain begins 30 mins-2 hours after eating when the stomach is empty -Pain is relieved by food Treatment -Antacids: to neutralize gastric contents, elevate pH, inactive pepsin, and relieve pain -Proton pump inhibitors, anticholinergic drugs: To suppress acid secretion -Bismuth (pepto-bismol): To coat ulcer -Surgical resection |
|
|
What are gastric ulcers? |
Trends to develop in the antral region of the stomach, adjacent to the acid-secreting mucosa of the body. -Frequently caused by H. pylori -Primary defect: Increased mucosal permeability to H+ |
|
|
What are the clinical manifestations and treatment for gastric ulcers? |
Clinical manifestations -Pain occurs immediately after eating -Tends to be chronic -Anorexia, vomiting, and wait loss Treatment -Same as the treatment for duodenal ulcers |
|
|
What is a stress ulcer? |
A stress ulcer is a single or multiple mucosal defect during the physiologic stress of serious illness.
|
|
|
What are the two types of stress ulcers? |
-Ischemic ulcer -Develops within hours of an event -Chushing ulcer -Develops as a result of a head trauma or brain surgery from hypersecretion of hydrochloric acid from the vagal nuclei. |
|
|
What are the clinical manifestations and treatment of stress ulcers? |
Clinical manifestations -Bleeding (most common) Treatment -Prophylactic therapy |
|
|
This refers to a number of disorders in which the intestine can't adequately absorb certain nutrients into the bloodstream. It can impede the absorption of macronutrients (proteins, carbohydrates, and fats), micronutrients (vitamins and minerals), or both
|
Malabsorption syndrome |
|
|
Failure of the chemical processes of digestion. |
Maldigestion |
|
|
This is insufficient pancreatic enzyme production. |
Pancreatic insufficiency -Causes: Pancreatitis, pancreatic carcinoma, pancreatic resection, and cystic fibrosis -Fat maldigestion is the primary problem |
|
|
What are the most common signs and treatment for pancreatic inefficiency? |
Clinical insufficiency -Fatty stools (steatorrhea); weight loss Treatment -Lipase supplements |
|
|
This causes fermentation of lactose by bacteria, causing gas (cramping pain, flatulence) and osmotic diarrhea. |
Lactase gene -Treatment: Lactose-free, adequate calcium intake |
|
|
What is bile-salt deficiency? |
-The result of liver disease and bile obstructions. -Poor intestinal absorption of lipids causes fatty stools, diarrhea, and loss of fat-soluble vitamins (A,D,E,K) -Treatment -Increase medium-chain triglyclerides |
|
|
What are the symptoms associated with the following vitamin deficiencies? |
Vitamin A: Night blindness Vitamin D: Decreased calcium absorption (osteoporosis) Vitamin K: Decreased clotting (purpura, petechiae) Vitamin E: Neurologic defects in children |
|
|
This is rapid emptying hypertonic chyme from the stomach. |
Dumping syndrome -Usually occurs after meals in patients who have recently undergone gastric surgery |
|
|
What are the clinical manifestations and treatment(s) for dumping syndrome? |
Clinical manifestations -Diarrhea, cramping, nausea, and vomiting Treatment -Frequent small meals high in protein and low in carbohydrates -Drinking fluids between meals instead of at meal time -Reconstructing the pylorus and drugs to slow intestinal transit |
|
|
This involves chronic inflammation of all or part of your digestive tract caused by an unknown origin.
|
Inflammatory bowel Disease Possible causes -Genetics -Alterations of epithelial barrier functions -Immune reactions to intestinal flora -Abnormal T-cell Eg. Chron's, ulcerative colitis |
|
|
This is an inflammatory bowel disease (IBD) that causes long-lasting inflammation and ulcers (sores) in your digestive tract. Ulcerative colitis affects the innermost lining of your large intestine (colon) and rectum. Symptoms usually develop over time, rather than suddenly.
|
Ulcerative colitis
|
|
|
What are the suggested causes, clinical manifestations and treatment(s) for ulcertive colitis? |
Suggested causes -Infectious, immunologic (anti-colon antibodies), dietary, genetics Clinical manifestations -Diarrhea (10 to 20 bm/day), bloody stools, cramps -Remission Treatment -Anti-inflammatories, steroids, immunosuppressive agents -Brad-spectrum antibiotics -Surgery: resection of the colon or colostomy |
|
|
This is an inflammatory disorder that affects any part of the digestive tract, from mouth to anus and causes "skip" lesions. |
Crohn Diseases -Difficult to differentiate from ulcerative colitis -Strong genetic association -Ulcerations: longitudinal and transverse inflammatory fissures that extend into lymphoid tissue (produce a "cobblestone" appearance). |
|
|
What are the clinical manifestations and treatment(s) for crohn's disease? |
Clinical manifestations -Abdominal pain and diarrhea; >5 stools per day -Anemia may develop as a result of vit 12 malabsorption. Treatment -Similar to ulcerative colitis -Immunodulatory agents -surgery -Complications: short bowel syndrome with malabsorption, diarrhea, and nutritional deficiencies. |
|
|
Herniation of mucosa through the muscle layers of the colon wall. |
Diverticula |
|
|
Define diverticulosis |
-Asymptomatic diverticular diesase |
|
|
Inflammatory stage of diverticular disease. |
Diverticulitis |
|
|
This is a condition in which muscle spasm in the colon (lower intestine) in the presence of diverticula causes abdominal pain and disturbance of bowel function without inflammation.
|
Diverticular disease |
|
|
What are the clinical manifestations and treatment(s) of diverticular disease? |
Clinical manifestations -Low cramping abdominal pain, diarrhea, constipation, distention, flatulence -Diverticulitis: Fever, Leukocytosis Treatment -Increase of dietary fiber intake to improve transit times and relieve symptoms -Uncomplicated diverticular disease: Bowel rest and antibiotics administration -Surgical resection |
|
|
a serious medical condition in which the appendix becomes inflamed and painful.
|
Appendicitis -Possible causes -Obstruction, ischemia, infection, ulceration |
|
|
What are the clinical manifestations and treatment(s) of appendicitis? |
Clinical manifestations -Epigasteric and lower quadrant pain, rebound tenderness -Nausea, vomiting, fever, leukocytosis -Complications: Perforation (hole), peritonitis (inflammation of the peritoneum) Treatment -Antibiotics |
|
|
What is irritable bowel syndrome? |
Functional gastrointestinal disorder with no specific structural or biochemical alterations -Visceral hypersensitivity -Abnormal gastrointestinal permeability, motility, and secretion -Infectiousness irritable bowel syndrome -Overgrowth of intestinal flora -Food allergy or intolerance -Psychosocial factors |
|
|
What are the clinical manifestations and treatment(s) of irritable bowel syndrome? |
Clinical manifestations -Lower abdominal pain -Diarrhea-predominant, constipation-predominant, or alternating diarrhea and constipation -Gas, bloating -Nausea Treatment -No available cure -Administration of laxitaves and fiber, antispasmodics -Treat pain and/or diarrhea -Alternative therapies -Prebiotics, probiotics, herbal treatment, psychotherapies |
|
|
What are the molecules that inhibit eating? |
Anorexins |
|
|
A patient with anorexia nervosa has ___% of their normal body weight for their age and height. |
15% |
|
|
How long does a person have to be binge eating for them to be considered bulimic? |
-two-binge eating episodes per week for at least 3 months. |
|
|
Binge-eating disorder is associated with what symptoms? |
-Eating much more rapidly than normal -Eating until uncomfortably full -Eating large amounts of food when not physically hungry -Eating alone because of being embarrassed -Feeling disgust, depressed, or very guilty after overeating. |
|
|
Explain on a micro level, what happens during short-term starvation and long-term? |
Short-term -Glycogenolysis: splitting of glycogen into glucose. -Gluconeogenesis: Formation of glucose from noncarbohydrate molecules. -Leads to ketosis (a condition characterized by raised levels of ketone bodies in the body, associated with abnormal fat metabolism and diabetes mellitus)and acidosis (an excessively acid condition of the body fluids or tissues). Long-term -Marsamus (severe undernourishment causing an infant's or child's weight to be significantly low for their age). -Kwasiorkor (a form of malnutrition caused by protein deficiency in the diet, typically affecting young children in the tropics). -Cachexia is a general sign of starvation (weakness and wasting of the body due to severe chronic illness). |
|
|
This is severe impairment or necrosis and hepatic encephalopathy of liver cells without preexisting liver disease or cirrhosis. |
Acute liver failure Leading cause: Acetaminophen overdose |
|
|
What are the clinical manifestations and treatment(s) of acute liver failure? |
Clinical manifestations -Anorexia -Vomiting -Abdominal pain -Jaundice Treatment -N-acetylcysteine: for acetaminophen poisoning -Antiviral therapy: For viral hepatitis -Lowering blood ammonia levels |
|
|
What is portal hypertension? |
High blood pressure in the portal venous system primarily caused by resistance to portal blood flow. -Increase to at least 10 mm Hg (usually 3 mm Hg) |
|
|
What are the consequences of portal hypertension? |
-Varices -Distended, tortuous, collateral veins -Lower esophagus, stomach, rectum -If rupture: life threatening -Splenomegaly -Hepatopulmonary syndrome (In medicine, hepatopulmonary syndrome is a syndrome of shortness of breath and hypoxemia (low oxygen levels in the blood of the arteries) caused by vasodilation (broadening of the blood vessels) in the lungs of patients with liver disease) |
|
|
What are the clinical manifestations and treatments of portal hypertension? |
Clinical manifestations -Vomiting blood; ascites -May be fatal Treatment -No definite treatment -Beta-blockers: To prevent variceal bleeding |
|
|
The accumulation of fluid in the peritoneal cavity, causing abdominal swelling.
|
Ascites -Most common cause: Cirrhosis |
|
|
What are the clinical manifestations and treatment of ascites? |
Clinical manifestations -Abdominal distention and weight gain Treatment -Dietary salt restriction -Strong diuretics -Possible administration of albumin -Paracentesis: Removal of fluid and relief of respiratory -Removing too much fluid too fast relieves pressure on the blood vessels, causing arteriolar vasodilation and carries the risk of hypertension, shock, or death. -Liver transplant: best treatment option |
|
|
This is the accumulation of toxins related to liver failure, causing a disruption of neurotransmittion (Ammonia toxic to the brain). |
Hepatic encephalopathy |
|
|
What are the clinical manifestations and treatment of ascites? |
Clinical manifestations -Personality changes, confusion, memory loss -Flapping tremor (asterixis), stupor, coma, death Treatment -Correct fluid and electrolyte imbalances -Restrict dietary protein intake -Altering intestinal bacteria -Antibiotics, lactulose |
|
|
What causes jaundice? |
-Extra-hepatic obstruction to bile flow (gallstones) -Intrahepatic obstruction (hepatocellular diseases such as cirrhosis or hepatitis) -Excess production of bilirubin (excessive hemolysis) |
|
|
What are the clinical manifestations and treatment(s) for jaundice? |
Clinical Manifestation -Dark urine and clay-coloured stools -Yellow discolorations often starts in the sclera of the eye Treatment -Correct the cause: Jaundice is only a sign |
|
|
What are the 3 types of hepatitis and their descriptions? |
Hepatitis A (infectious hepatitis) -Fecal-oral transmission -Acute infections, vaccine available Hepatitis B -Transmitted via blood and bloody fluids -Causes chronic infections , vaccine available Hepatitis C -Post-transfusion hepatitis, also implicated in IV drug use -80% develop chronic liver disease, no vaccine available |
|
|
What is pancreatitis associated with and why? |
Pancreatitis is associated with alcohol intake and chilelithiasis (the formation of gall stones). Why -Damaged pancreatic cells and ducts leak pancreatic enzymes into the pancreatic tissue -Enzymes digest pancreatic tissue, leak into the bloodstream to cause injury to blood vessels and other organs. **Can be acute or chronic |
|
|
What are the clinical manifestations and treatment(s) of pancreatitis? |
Clinical manifestations -Epigasteric or mid-abdominal pain -Nausea and vomiting -Fever and leukocytosis -Repeated acute pancreatitis can lead to chronic changes -Destroys acinar cells and the islets of Langerhans -Pancreatic parenchyma replaced by fibrous tissues, calcification, actual obstruction, and pancreatic cysts Treatment -Cessation of alcohol use (as its the most common cause) -Analgesics and surgical drainage of cysts or partial resection of pancreas |
|
|
Where is esophagus cancer the most common? |
Gastroesophageal junction |
|
|
What causes esophageal cancer? |
Facilitated by chronic inflammation and dysplasia caused by gastroesphageal reflux and long-term exposure to irritants (tobacco and alcohol) |
|
|
What are the clinical manifestations and treatment(s) of esophageal cancer? |
Clinical Manifestations -Chest pain and dysphagia -Occurs in individuals older than 60 years of age Treatment -Surgical removal -Chemo and radiation -Stents |
|
|
What are the risk factors of stomach cancer? |
-Infection with a Helicobacter pylori strain (80% of cases) -Dietary factors -Food additives (nitrates) in pickled or salted foods (bacon) -Low intake of fruits and vegetables -Atrophic gastritis -Lifestyle, alcohol consumption, cigarette smoking |
|
|
Where does stomach cancer generally start? |
Begins in the glands of the stomach mucosa |
|
|
What are the clinical manifestations and treatment(s) of stomach cancer? |
Clinical manifestations -Symptoms usually do not occur until the tumor has metastasized -Weight loss, upper abdominal pain, vomiting, hematemesis (vomiting of blood), anemia Treatment -Surgical removal -Chemo and radiation |
|
|
What is the most common cancer of the small intestine? |
Adenocarcinoma |
|
|
What is the most common cause of colon and rectal cancers? |
adenomatous polyps (a mass or projection arising from the mucosal epithelium). |
|
|
What are the clinical manifestations and treatments of colon and rectal cancers? |
Clinical manifestations -Ascending colon: 25% -Pain, mass, change in bowel habits, anemia -Transverse colon: 15% -Pain, obstruction, change in bowel habits, anemia -Descending colon: 5% -Pain, change in bowel habits, bright red blood in stool, obstruction -Rectum: 10% -Blood in stool, changes in bowel habits, rectal discomfort Treatment -Surgery, possibly a colostomy -Radiation -Adjuvant chemoradiotherapy |
|
|
Rectal carcinomas are located where and tend to spread where? |
-Located up to 15 cm from the opening of the anus -Tumor spreads transmurally(passing through an atomical wall) to the vagina in woman or to the prostate in men |
|
|
What are the clinical manifestations and treatment of pancreatic cancer? |
Clinical manifestations -Initial symptom: vague abdominal or mid-back pain -Jaundice Treatment -Surgery-reconstruction or total removal -Chemotherapy |
|
|
After a fracture, how does bone heal? |
heals with normal tissue, not scar tissue |
|
|
What are the different fracture classifications? |
-Complete: Bone is broken all the way through -Incomplete: Bone is damaged but still in one piece -Closed or simple: (complete or incomplete): skin is intact -Open or Compound (complete or incomplete):skin is broken -Comminuted: Bone breaks in more than two fragments -Linear: Fracture runs parallel to the long axis of the bone -Oblique: Fracture of the bone is slanted -Spiral: Encircles the bone -Transverse: occurs straight across the bone -Green-stick: Perforates one cortex and splinters the spongy bone. -Pathologic: Breaks occur at the site of a pre-existing abnormality (CIC LOST GP) |
|
|
What are the phases of bone fracture healing? |
Inflammatory phase -Lasts 3-4 days -Bone tissue destruction triggers an inflammatory response -hematoma formation Repair phase -Lasts several days -Capillary in growth, mono-cellular cells, and fibroblasts transforms hematoma into granulation tissue -Osteoblasts within the procallus synthesize collagen and matrix to the callus Remodeling phase -Lasts months to years -Unnecessary callus is reabsorbed, and trabeculae, bone can withstand normal stresses |
|
|
What are the clinical manifestations and treatment(s) of a bone fracture? |
Clinical manifestations -Unnatural alignment, swelling, muscle spasms, tenderness, pain, impaired sensation Treatment -Closed manipulation, traction (skeletal or skin), open reduction, internal fixation, external fixation -Splints and casts |
|
|
Temporary displacement of bone from its joint. |
Dislocation |
|
|
Contact between the bones in the joint is only partially lost. |
Subluxation |
|
|
What are the clinical manifestations and treatment(s) of bone dislocation and subluxation? |
Clinical manifestations -Pain -Swelling -Limitation of ROM -Joint deformity Treatment -Reduction and immobilization fro 2-6 weeks -Exercise |
|
|
Whats the difference between a strain, sprain, and avulsion? |
Strain -Tear or injury to a tendon (fibrous connective tissue that attaches skeletal muscle to the bone) Sprain -Tear or injury to a ligament (Fibrous connective tissue that connects bones) Avulsion -Complete separation of a tendon or ligament from its bony attachment site |
|
|
Explain the patho process of support structure trauma healing? |
-Inflammatory exudate develops between the torn ends -Granulation tissue grows inward, and then collagen formation begins 3-4 days after injury -Vascular fibrous tissue fuses the new and surrounding tissues into a single mass. |
|
|
What are the clinical manifestations and treatment(s) for support structure trauma? |
Clinical manifestations -Painful and usually accompanied by soft-tissue swelling and changes in tendon or ligament contour Treatment -Splinting, early motion, and rehabilitation -Suturing: to treat a complete rupture -If suturing is not possible: tendon or ligament grafting -Prolonged rehabilitation exercises |
|
|
This is the inflammation of a tendon |
Tendinitis |
|
|
What is tendinosis? |
The painful degradation of collagen fibers |
|
|
What is bursitis? |
Inflammation of the bursa (synovial sacs lined with synovial membrane and filled with synovial fluid) and is caused by repeated trauma. -Septic bursa: Is caused by a wound infection. |
|
|
What is epicondylitis? |

The painful inflammation of tendons surrounding an epicondyle. -Tennis elbow: Lateral epicondylitis -Golfer's elbow: Medial epicondylitis |
|
|
What is the treatment for tendiopathy and bursitis? |
-Systemic analgesics, ice or heat applications, or local injection of an anesthetic and a corticosteriod to reduce inflammation -Bursitis: Aspirations to drain excess fluid -Physical therapy |
|
|
What is a muscle strain? |
A muscle strain is a sudden, forced motion, causing the muscle to become stretched beyond its normal capacity. -Causes local muscle damage -Can involve the tendons -Muscle cells can usually regenerate (may take up to 6 weeks) |
|
|
If a bad muscle strain or contusion is neglected then it is possible that this can occur. It is usually as a result of impact which causes damage to the sheath that surrounds a bone called the periostium as well as to the muscle. Bone will grow within the muscle, called calcification which is painful. |
myositis ossificans-"Rider's bone" in equestrians-Thigh muscles in football players
|
|
|
What is rhabdomyolysis? |
-Life-threatening complication of severe muscle trauma with muscle cell loss -Rapid breakdown of muscle that causes the release of intracellular contents (myoglobin enters extracellular space and bloodstream) |
|
|
What are the clinical manifestations and treatment(s) of rhabdomyolysis? |
Clinical manifestations -Classic triad -Muscle pain, weakness, dark urine (from myoglobin) Treatment -Rapid intravenous hydration: to maintain adequate kidney flow -Hyperkalemia: May require temporary hemodialysis |
|
|
What are the potential causes of osteoporosis? |
-Decreased levels of estrogen and testosterone -Decreased activity level -Inadequate levels of vit D and calcium or magnesium -Postmenopausal osteoporosis -Increased osteoclast activity and family history -Glucocorticoids inhibit osteoblasts function |
|
|
What are the clinical manifestations and treatment(s) of osteoporosis? |
Clinical manifestations -Pain -Bone deformity -Fractures -Kyphosis (hunchback) -Diminished height Treatment -Estrogen -Biphosphonates, parathyroid hormone (PTH)1-84.... |
|
|
How can osteoporosis be prevented? |
-Regular moderate weight-bearing exercises -Calcium intake sufficient to maintain normal calcium balance during adolescence -Sufficient intake of magnesium |
|
|
The softening of the bones, typically through a deficiency of vitamin D or calcium.
|
Osteomalacia -Deficiency of vit D lowers the absorption of calcium from the intestines -Bone formation progresses to osteoid (protein matrix), but calcification does not occur causing soft bones. |
|
|
Rickets is the name for ______ in kids. |
Osteomalacia
|
|
|
What are the clinical manifestations and treatment(s) for osteomalcia? |
Clinical manifestations -Pain -Bone fractures -Vertebral collapse -Bone malformation waddling gait Treatment -Adjust serum calcium and phosphate levels to normal -Administer dietary supplements of vit D |
|
|
inflammation of bone or bone marrow, usually due to infection.
|
Osteomyelitis -Usually caused by a staphylococcal infection -Original infection can be exogenous or bloodborne (endogenous) -Infection spreads under the periosteum and along the bone shaft or into the bone marrow |
|
|
What are the clinical manifestations and treatment(s) for osteomyelitis? |
Clinical manifestations -Acute and chronic inflammation -Fever -Pain -Necrotic bone Treatment -Antibiotics -Debridment -Surgery -Hyperbaric oxygen therapy |
|
|
What is osteosarcoma? |
a malignant tumor of bone in which there is a proliferation of osteoblasts (which osteoids which are bone forming tumors).
-33% of bone tumors -Predominant in adolescents and young adults; occurs in seniors with a history of radiation therapy -Location: In the metaphyses of the long bones -50% occur around the knees |
|
|
What are the clinical manifestations and treatment(s) of osteosarcoma? |
Clinical manifestations -Pain -Swelling Treatment -Systemic chemotherapy and surgery |
|
|
What is chondrosarcoma? |
Chondrosarcoma is a cancer composed of cells derived from transformed cells that produce cartilage. Chondrosarcoma is a member of a category of tumors of bone and soft tissue known as sarcomas.
-Is a tumor of middle-age and older adults -Is frequently in the metaphyses or diaphysis of long bones. -Can expand into the neighboring soft tissues |
|
|
What are the clinical manifestations and treatment(s) of chondrosarcoma? |
Clinical manifestations -Pain and swelling Treatment(s) -Wide surgical excision |
|
|
This is a sarcoma in which the predominant cell type is a malignant fibroblast.
|
Fibrosarcoma -Fiborous masses of collagen, malignant fibroblasts, and osteoclast-like cells -Usually affects the metaphyses of the femur or tibia |
|
|
What are the clinical manifestations and treatment(s) of fibrosarcoma? |
Clinical manifestations -Pain -Swelling -Local tenderness -Palpable mass and limitation of movement -Pathologic fracture Treatment -Radical surgery and amputation |
|
|
What are myelogenic tumors? |
-Develop from various bone marrow cells -Giant cell tumors -Causes extensive bone resorption -Is located in the epiphyses of femur, tibia, radius, or humerus. -Has slow and relentless growth rate; metastasis is rare |
|
|
What are the clinical manifestations and treatment(s) for myelogenic tumors? |
Clinical manifestations -Pain -Local swelling -limitations of movement Treatment -Bone graft |
|
|
This means disease of the joints |
arthropathies |
|
|
What is the difference between osteoarthritis and rheumatoid arthritis? |
Osteoarthritis -Common age-related disorder of the synovial joint -Inflammation of the joint (both) -loss of articular cartilage, sclerosis of underlying bone, and formation of bone spurs (osteophytes) Rheumatoid Arthritis -Inflammatory joint disease (both) -Autoimmune destruction of the synovial membrane and joints |
|
|
What are the clinical manifestations and treatment(s) of osteoarthritis? |
Clinical manifestations -Pain, stiffness, enlargement of the joint, tenderness, limited motion, and deformity -Joint swelling in the fingers -Joint effusion: Exudate or blood entering the joint Treatment -Rest of involved joint until inflammation subsides -Aerobic exercise and range-of-motion exercise -Analgesics and antiinflammatory drugs -Surgery: joint replacement |
|
|
What are the clinical manifestations and treatment(s) of rheumatoid arthritis? |
Clinical manifestations -Symmetric joint swelling -Joint deformities Treatment -Anti-rheumatic drugs, monoclonal antibodies -NSAIDS, glucocorticoids, intra-articular steroid injections -Physical and occupational therapy -Surgery: synovectomy or joint replacement |
|
|
This is a chronic, progressive, painful form of inflammatory arthritis, which affects mainly the spine and sacroiliac joints (the joints where the spine attaches to the pelvis).
|
Ankylosing spondylitis -Unknown cause but strong association with certain HLA antigens -Begins with inflammation of the fibrocartilage, particularly in the vertebrae and sacroiliac joint -Inflammatory cells infiltrate and erode the fibrocartilage -As repair begins, scar tissue ossifies and calcifies; the joint eventually fuses |
|
|
What are the clinical manifestations and treatment(s) for ankylosing spondylitis? |
Clinical manifestations -Low back pain -Stiffness -Pain -Restricted motion -"bamboo" spine -Loss of normal lumbar curvature Treatment -Physical therapy: Maintenance of skeletal mobility -NSAIDS, analgesic medications -Corticosteriods injections to locally inflamed joints |
|
|
In this disease, uric acid crystallizes and the crystals are deposited in connective tissue throughout the body. |

Gout Causes -Purine synthesis or breakdown is accelerated -Poor uric acid secretion in the kidneys |
|
|
What are the clinical manifestations and treatment(s) of gout? |
Clinical manifestations -Increase in serum urate concentration: Hyperuricemia -Monoarticular arthritis: Usually the great toe -Deposits or urate crystals (tophi) in and around the joints -Formations of renal stones Treatment -NSAIDS, hydrocortisone: May be injected into the joint -Low-fat dairy products and vegable source of protien |
|
|
This causes chronic widespread joint and muscle pain, fatigue, and tender points. The CNS dysfunctions to cause amplified pain transmission and interpretation. |
Fibromyalgia Possible factors -Flu-like viral illness, chronic fatigue syndrome, Lyme disease, medications, physical or emotional trauma |
|
|
What are the clinical manifestations and treatment(s) of fibromyalgia? |
Clinical manifestations -Diffuse, chronic pain -Nine pairs (18) of tender points -Must have tenderness in 11 of these tender points -Vague symptoms -Increased sensitivity to touch, absence of inflammation, fatigue, sleep disturbances Treatment -Education, medication, exercise |
|
|
What is chronic fatigue syndrome? |
a medical condition of unknown cause, with fever, aching, and prolonged tiredness and depression, typically occurring after a viral infection.
-Also known as myalgic encephalomyelitis -Possible causes -CNS dysregulation, immune system abnormalities, dysfunction of cellular energy metabolism, dysfunction of ion transport |
|
|
What are the clinical manifestations and treatment(s) of chronic fatigue syndrome? |
Clinical manifestations -Unrestful sleep -Debilitating fatigue, noninflammatory joint pain, headaches, flu-like symptoms, and memory or concentration problems Treatment -Consideration of psychosocial factors, and symptomatic and supportive care (massage ect.) |
|
|
This is a muscular atrophy that results from lack of muscle use.
|
Disuse atrophy |
|
|
What is myotonia? |
inability to relax voluntary muscle after vigorous effort.
-Cause: Lack of chloride -Treatment: Medication to reduce muscle fiber excitability |
|
|
This term is used in reference to primary muscle disorders |
Myopathy |
|
|
This is the name given to muscle inflammation and weakness caused by drugs and toxins.
|
Toxic myopathy
-Alcohol is the most common cause -Associated with myogloinuria (myoglobin in urine) and renal failure -Necrosis of the individual muscle fibers -Gene dysregulation, and initiation of apoptosis -Benign cramps and pain, resolving in a matter of hours to severe weakness -Treatment -Abstinence of alcohol -Improved nurtition |
|
|
What are the functions of the skin? |
-Primary function: To protect the body -To provide a barrier against microorganisms, ultraviolet radiation, loss of body fluids, and the stress of mechanical forces -Regulates the body temperature, involved in the production of vit D and immune surveillance, sensory function |
|
|
a condition in which the pigment is lost from areas of the skin, causing whitish patches, often with no clear cause.
|
vitiligo |
|
|
What are aging changes of the skin? |
-Becomes thinner, drier, wrinkled, and demonstrates changes in pigmentation -Number of capillary loops shorten and decrease -Melanocytes and Langerhans cells are fewer -Sebaceous, eccrine, and apocrine glands atrophy -Temperature regulation is compromised -Sensory receptors decrease -Many of the protective functions of the skin decrease -Infection increase, and wound healing is delayed |
|
|
a small, raised, solid pimple or swelling, often forming part of a rash on the skin and typically inflamed but not producing pus.
|
papule -Primary lesion |
|
|
define macule |
a distinct, flat spot, such as a discolored spot on the skin. (primary lesion)
|
|
|
An elevated, firm, and circumscribed lesion. Its deeper in the dermis than a papule and measures about 1-2 cm in diameter.
|
Nodule -Primary lesion |
|
|
define tumor |
a swelling of a part of the body, generally without inflammation, caused by an abnormal growth of tissue, whether benign or malignant.
(primary lesion) |
|
|
An elevated, circumscribed, and superficial lesion that does not extend into the dermis, and is filled with a serous fluid (< 1 cm in diameter). |
vesicle -Primary lesion |
|
|
define pustule |
a small blister or pimple on the skin containing pus. (primary lesion)
|
|
|
in the body, a membranous sac or cavity of abnormal character containing fluid or semisolid material.
|
Cyst -Primary lesion |
|
|
Define telangieclasia |

a condition characterized by dilation of the capillaries, which causes them to appear as small red or purple clusters, often spidery in appearance, on the skin or the surface of an organ. (primary lesion)
|
|
|
They represent a thin heaping up of the outermost layer of the skin (the stratum corneum) and can be due to a variety of skin conditions, most frequently excessive dryness.
|
Scale -Secondary lesion |
|
|
define keloid |
an area of elevated, irregular fibrous tissue formed at the site of a scar or injury, it progressively enlarges.
-Secondary lesion |
|
|
This is localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear.
|
Pressure ulcer -occlude capillary blood flow with resulting ischemia and necrosis |
|
|
describe the stages of a pressure ulcer |
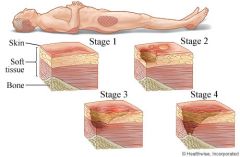
Stage I - Erythema of intact skin (reddening of the skin) Stage II - Partial-thickness skin loss, involving the epidermis or dermis Stage III - Full-thickness skin loss, involving damage or loss of the subcutaneous tissue Stage IV - Full-thickness skin loss with damage to muscle, bone, or supporting structures. |
|
|
How are pressure ulcers treated? |
-Skin assessment with re-positioning and turning -Use of pressure reduction surfaces and specialty beds -Maintenance of fluid, protein, and caloric intakes -Superficial ulcers: Flat, moister-retaining dressings -Negative pressure would healing: for stage II & IV -Infection: Antibiotics and pain control |
|
|
What is pruritus? |
severe itching of the skin, as a symptom of various ailments.
-Most common symptom of primary skin disorders -Itch: specific unmyelinated C-nerve fibers |
|
|
This is a red, itchy rash caused by a substance that comes into contact with your skin. The rash isn't contagious or life-threatening, but it can be very uncomfortable.
|
Contact dermatitis -Allergic contact dermatits: when allergens come into contact with the skin -Irritant contact dermatitis: Chemical irritation exposure to irritating substances |
|
|
What is stasis dermatitis? |
-Occurs in the legs as a result of venous stasis, edema, and vascular trauma -Sequence of events edema, erythema, pruritus, scaling, petechiae, hyperpigmentation, and ulceration -Treatment -Elevate legs -Avoid standing for long periods -Infections: Administer antibiotics -Chronic lesions with ulceration: apply moist dressing, external compression garments, and vein ablation surgery |
|
|
This is an inflammatory skin disorder affecting the scalp, face, and torso. It causes greasy, scaly, white, or yellowish plaques.
|
Seborrheic dermatitis, also known as seborrhea, sebopsoriasis,seborrheic eczema, dandruff and pityriasis capitis, is a chronic, relapsing and usually mild dermatitis. In infants seborrheic dermatitis is called cradle cap.
Treatment -Mild cases: Shampoos containing sulfer, salicylic acid, or tar -Ketoconazole with topical T cell inhibitors -Corticosteriod applications: To treat severe symptoms |
|
|
What is psoriasis? |
-a skin disease marked by red, itchy, scaly, thick, elevated patches.
-A T-cell autoimmune-mediated skin disease. |
|
|
a severe abscess or multiple boil in the skin, typically infected with staphylococcus bacteria.
|
carbuncles -Clinical manifestations -Chills, fever, Malaise |
|
|
Whats the difference between Erysipelas and Impedigo? |
Ersipelas -Acute superficial infection of the upper dermis -Superficial form of cellulitis -Treatment: Cold compresses and systemic antibiotic Impetigo -Common in children -Superficial lesion of the skin -Caused staphylococcus or GRP A Streptococci |
|
|
inflammation of subcutaneous connective tissue.
|
Cellulitis |
|
|
Fungi causing superficial skin lesions |
Dermatophytes |
|
|
Urticaria |
a rash of round, red welts on the skin that itch intensely, sometimes with dangerous swelling, caused by an allergic reaction, typically to specific foods. (HIVES)
|
|
|
This is a birthmark or a mole on the skin, especially a birthmark in the form of a raised red patch.
|
Nevus -Nevi plural |
|
|
Whats the difference between paronychia and onychomycosis? |
Paronychia -Bacterial (acute or chronic) infection of the cuticle -Clinical manifestations: Painful; abscess may develop -Treatment -Hands: keep dry -Abscesses: infection and drainage -Severe bacterial cases: systemic antibiotic Onychomycosis -Fungal or dermatophyte infection of the nail plate -Clinical manifestations: Turns yellow or white -Treatment -Debridment -Systemic antifungal therapy |