Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back

|
Restrictive lung disease.: Normal pt the slope is very steep because they are exhaling very quickly. In a pt with restrictive disease the relationship is the same as in the healthy pt and the slope is steep but the volumes are diminished maybe half as much
|
|

|
Restrictive lung disease. No normal alveolar septa. Diminished compliance to expand when inspie but elastic recoil is increased.
|
|

|
Sarcoidosis: Bilateral hilar lymphadenopathy and interstitial lung infiltrates
|
|

|
Sarcoidosis: Asteroid bodies and schauman bodies (calcium concentrations.
|
|

|
Obstructive disease: Pt with obstructive disease there is resitance to outflow of air from the lungs, so addition to volumes themselves being diminished the slope of the curve it is consideraly flattened.
|
|

|
Emphysema: Lung are hyperinflated due to air caputrued within the lung.
|
|

|
Emphysema: Outer lung, Pigment on plural surface. Air trapped makes it inflammed.
|
|

|
Centriacinar emphysema. Damage is significant in upper lobes with pigment deposition
|
|

|
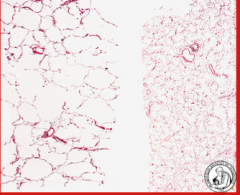
Lung with panacinar disease, very diffuse in distribution and orderly with cystic spaces as opposed to centracinar dz which is more localized with distribution
|
|
|
Normal lung on the right, and pancinar lung on left, multifocal cyst formation diffusely
|
|

|
Portion of lung, parenchyma is normal but there subplural air spaces and if pressure gets high enough and expands at some point it will pop and if it ruptures through the normal septa the air gets out into the plural cavity and causes pneumothorax
|
|

|
Paraseptal emphysema: huge cystic spaces underneath plura
|
|

|
Cross section of proximal airway of a pt with chronic bronchitis, mucuous glands are so hyperplastic that they comprise most of what we see…and all that mucous goes to the lumen of the airways
|
|

|
Mucuous cast and inflammation of airways
Chronic bronchitis. |
|

|
Pt with long standing asthma, conducting airway with globet cell hyperplasia and inflammatory cells
|
|

|
Mucus plug with crystals which is a breakdown product from eosinophil granules and these are seen in patients with chronic ashtma and they indicate hypereosinophilia.
|
|
|
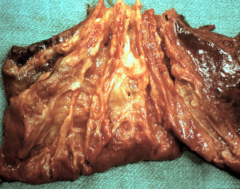
Lobe of lung from a patient with localized BRONCHIECTASIS, conducting airways are almost touching the visceral pleura, which wouldn’t be seen in normal lungs. This fusiform bronchiectasis which is involving multiple conducting airways
|
|

|
This is a patient with a carcinoid tumor, which has completely obstructed the lobar bronchus, and there is infection distal or behind the obstruction with accumulation of mucus and all sort of materials and the airways can be traced all the way to the pleural surface which is not normal.
|
|

|
Big dilated airspace, we cant see cartilage so we know this is the bronchiolar level because this is an airway with no cartilage and It is dilated. This image is characteristic of bronchiectasis along with mucus plugging and secondary inflammation
|