Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
43 Cards in this Set
- Front
- Back
|
Multiple ovarian follicular cysts due to hormone imbalance
|
Polycystic ovarian disease characterized by increased LH and low FSH.
|
|
|
How does it polycystic ovarian disease present?
|

Usually obese young woman with infertility, oligomenorrhea and hirsutism( LH increase). Some pts have insulin resistance and may develop DM2 10-15 yrs later. bilaterally enlarged ovaries with sclerotic cortex, numerous follicle cysts (“oyster ovaries”)
|
|
|
Endometrial carcinoma risk increases with PCOD because
|
androgen conversion to estrone in adipose tissue leads to high levels of estrone which increases risk
|
|
|
the 2 most common subtypes of surface epithelial tumor are
|
serous (full of watery fluid) and mucinous (full of mucous like fluid), both are cystic. Both can be bening, borderline or malignant
|
|
|
surface epithelial benign tumor in a premenopausal women 30-40 yrs is usually
|
cystadenoma composed of a single cyst with a simple lining.
|
|
|
A malignant surface epithelial tumor in a postmenopausal women 60-70 yrs old is usually
|
Cystadenocarcinoma and it's composed of complex cysts with a thick, shaggy lining.
|
|
|
Whats the surface epithelial cell tumor with characteristics of both benign and malignant tumors?
|
Borderline, which have a better prognosis than malignant tumors but still have metastatic potential.
|
|
|
Serous low grade tumor characteristics
|
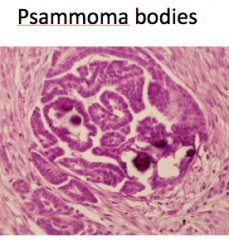
Well-defined papillary structures and many psammoma bodies
Low grade cytologic atypia Probably arise via borderline tumors Better prognosis |
|
|
Serous high grade tumor characteristics
|
Solid and papillary growth with fewer psammoma bodies
High grade cytologic atypia with hobnailing Probably arise de novo May orginate from tubal fimbriae Worse prognosis |
|
|
Serous low grade tumor markers
|
KRAS, BRAF
|
|
|
Serous High grade characteristics
|
p53, BRCA
|
|
|
May arise in endometriosis; contain viscous brown fluid (“chocolate”)
|
ENDOMETRIOID. Benign and borderline variants are rare
May be associated with synchronous primary endometrioid adenocarcinoma of the uterus P 53 mutation. |
|
|
Endometrioid carcinoma characterisitcs
|
Less common than serous carcinoma, more common than mucinous carcinoma;
less often bilateral than serous, more often bilateral than mucinous |
|
|
Clear cell carcinoma also may arise from endometriosis and it is rarely bilateral, and where there is bilateral then
|
rule out metastatic clear cell carcinoma, such as metastatic renal cell carcinoma.
|
|
|
Malignant mucinous surface epithelial tumor marker is
|
KRAS
|
|
|
Malignant mucinous tumors are rarely bilateral, and when they are it indicates
|
metastases to ovaries, usually GI source, especially appendix
|
|
|
Solid, unilateral, often incidental finding in ovary of postmenopausal woman.
|
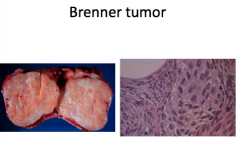
BRENNER TUMOR. Most are benign; rare borderline and malignant variants
|
|
|
Germ cell tumors benign are
|
“Dermoid”-Mature Cystic Teratoma
|
|
|
Malignant Germ cell tumors are
|
-Immature Teratoma,
-Carcinoma arising in Mature Cystic Teratoma, -Dysgerminoma, - Endodermal Sinus Tumor, -Choriocarcinoma, -Mixed |
|
|
germ cell tumors mimic tissues normally produced by germ cells, which tissues correspond to
Cystic teratoma and embryomal carcinoma: Dysgerminoma Endodermal sinus tumor Choriocarcinoma |
Cystic teratoma and embryomal carcinoma: fetal tissue
Dysgerminoma: oocytes Endodermal sinus tumor: yolk sac Choriocarcinoma: placental tissue |
|
|
benign teratoma are usually
|
(Mature Cystic Teratoma, aka “Dermoid”). Most are unilateral with Complex cystic structure containing cheesy sebaceous material, hair, teeth (!)
|
|
|
Teratoma with almost exclusively of one type of tissue: struma ovarii=thyroid tissue
|
Monodermal teratoma
|
|
|
Malignancy arising in Mature Cystic Teratoma; rare occurrence in older women; usually
|
squamous cell carcinoma
|
|
|
Immature teratoma who gets it and what is it?
|
Occurs in younger women (average age=18)
cystic and solid tumor with all 3 germ layers appearing IMMATURE Can be very aggressive, especially if contain a lot of immature neural tissue |
|
|
The most common germ cell tumor is
|
Teratoma
|
|
|
The most common malignant germ cell tumor is
|
dysgerminoma
|
|
|
Usually unilateral, occurs in 2nd and 3rd decades, solid.
-May occur in the setting of gonadal dysgenesis. |
DYSGERMINOMA. Good prognosis responds to radiotherapy
|
|
|
Testicular counterpart of dysgerminoma is
|
Seminoma
|
|
|
What type of receptor does dysgerminoma produce?
|
Receptor tyrosine kinase c-Kit
|
|
|
pediatric tumor, usually unilateral with papillary structures (“Schiller-Duval bodies) and hyaline globules are characteristic
|
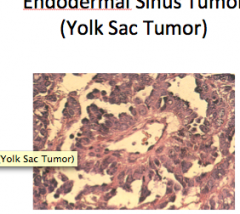
ENDODERMAL SINUS TUMOR
|
|
|
ENDODERMAL SINUS TUMOR produces
|
alpha-fetoprotein and alpha-one-antitrypsin
- Can be aggressive, but chemotherapy can be effective |
|
|
Malignant tumor composed of trophoblast and syncyntiotrophoblasts; mimics placental tissue but villi is abscent
|
---CHORIOCARCINOMA very bad prognosis. Produces B-hCG and it is characteristic.
|
|
|
In general: tumors of adults, unilateral, solid, benign sex cord stromal tumor
|
Pure fibroma: fibroblastic, no hormone production
|
|
|
Fibromas are associated with what syndrome?
|
Meigs syndrome: pleural effusions and ascites which resolves after removal of tumor
|
|
|
Germ cell tumor associated with production of androgen leading to hirsutism and virilization
|
Sertoli-Leydig cell tumor which is unilateral and benign
|
|
|
GRANULOSA-theca CELL TUMOR is proliferation of
|
Theca cells and granulosa cells. These are unilateral and considered benign with low malignant potential
|
|
|
Granulosa-theca tumors produce estrogen with causes different signs at different stages
Prior to puberty- Reproductive age- Postmenopause |
-Precocious puberty
-Menorrhagia or metrorrhagia -Endometrial hyperplasia with postmenopausal bleeding most common |
|
|
Most frequent primary sites of metastatic carcinoma
|
Mullerian sites, breast, GI tract
|
|
|
bilateral clear cell carcinoma could represent
|
metastatic renal cancer
|
|
|
bilateral mucinous borderline/carcinoma with pseudomyxoma peritoneii (mucin deposits often with neoplastic cells in peritoneum) could represent
|
metastatic appendiceal cancer
|
|
|
most famous metastatic carcinoma to the ovary:
|
KRUKENBERG TUMOR=metastatic signet ring cell carcinoma to the ovaries; usually gastric primary
|
|
|
-suppurative salpingitis may be caused by
|
gonococcus, Chlamydiae; may lead to chronic salpingitis
|
|
|
ADENOCARCINOMA OF THE FALLOPIAN TUBE
|
dominant tubal mass with mucosal involvement; may be associated with BRCA mutations;
|