![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
35 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
1. What is the tandem versus coaxial methods of percutaneous pancreatic biopsy? 2. How is EUS FNA superior? 3. What is the most common complication of FNA of the pancreas and how common? 4. What is a specific complication of EUS guided FNA? |
1. tandem: placing a guide needle to serve as a reference point for a second biopsy needle, most useful in real time CT guided visualization coaxial: inserts a larger caliber needle to localize the lesion then a smaller one is inserted though it to sample the lesions, permits multiple sampling attempts without risk to local structures due to repeated needle passes 2. real time visualization of needle tip better visualization of smaller lesions ability to ID local mets or invasion (simultaneous staging and diagnosis) 3. pancreatitis 1-3% 4. perforation associated with a malignant luminal stenosis |
|
|
|
1. For what type of pancreatic lesion does ROSE offer little value? Why? 2. What portion of an FNA sample should not be smeared? 3. How are bile duct brushings best prepared? why? 4. What three findings support a mucinous cyst? and malignancy in the cyst? |
1. Cysts b/c a drop of cyst fluid for smear is paucicellular 2. "worms" of clotted tissue from the needle cast which should be removed from the slide and submitted in formalin for cell block 3. liquid based, cytocentrifuge or cell block; because these liquid based collection methods allows for less mechanical artifact then dislodging cells from the brush 4. grossly viscous white fluid, cytologic evidence of colloidlike extracellular mucin and elevated CEA; cytomorphologic evaluation is necessary to establish malignancy |
|
|
|
SEE TABLE 14.1 ON PAGE 400 FOR BIOCHEMICAL AND MOLECULAR TESTS ON PANCREATIC CYSTS |
SEE TABLE 14.1 ON PAGE 400 FOR BIOCHEMICAL AND MOLECULAR TESTS ON PANCREATIC CYSTS |
|
|
|
1. What are the two most useful chemistry tests on cyst fluid? Explain the results and subsequent testing. 2. How are KRAS and GNAS helpful once a mucinous neoplasm is identified? how do they help identify malignancy? 3. What is the sensitivity and specificity of EUS-FNA of the pancreas? 4. What is the diagnostic accuracy based on lesion characteristics? 5. What is the sensitivity and specificity of brush cytology? |
1. CEA: if low, do KRAS to identify a mucinous cyst (if CEA is high it suggests mucinous anyway so KRAS is not needed) Amylase: 2. GNAS supports IPMN to distinguish it from mucinous cystic neoplasm (MCN) which is resected irrespective of grade; KRAS and GNAS do NOT help identify malignant lesions!! 3. sensitivity 80% on average, but variable specificity 60-100% 4. 90% for solid pancreatic masses and less for cystic lesions 5. sensitivity only 50% b/c of false negatives Specificity almost 100% |
|
|
|
1. What precludes a non-diagnostic interpretation? 2. What is an additional diagnostic category in pancreatic lesions to the 5 normal ones? (neg, atypical, suspcious, positive, non-diagnotic) 3. What does the above definition mean? 4. What is evidence of pancreatic intraepithelial neoplasia? |
1. ANY atypia 2. neoplastic 3. any case that is clearly represents a neoplasm including premalignant neoplasms (IPMN, IPNB and MCN with dysplasia) and lesions whose metastatic potential is unpredictable on cytology (PanNET and Solid pseudopapillary neoplasm SPN) 4. mucinous differentiation because pancreatic ducts are lined by nonminous cells |
|
|
|
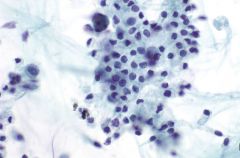
1. What is the cytomorphology of benign pancreatic acinar cells? 2. What is the cytomorphology of benign ductal cells? |
1. cohesive, grapelike aggregates, isolated and attached to a fibrovascular stroma scattered, stripped naked nuclei eccentrically placed, round nucleus evenly distributed, finely granular chromatin small nucleolus; larger in reactive acinar cells abundant granular cytoplasm (dense blue green on pap and punctate purple on romanowsky) indistinct cell borders in clusters 2. flat cohesive sheets (FEW isolated cells) even nuclear spacing in sheets (hoecomb, lattice like) round/oval nucleus evenly distributed fine granular chromatin inconcspicuous nucleoluls well defined cytoplasmic borders |
|
|
|
1. What is a well known artifact on liquid based preparations? 2. What normal cells may be inadvertently sampled in a pancreatic FNA? 3. What is the cytomorpholgy of GI contamination? |
1. crenated (notched/scallped) nuclei in ductal cells 2. mesothelial cells, hepatocytes, renal tubular cells, duodenum, stomac 3. duodenum: flat cohesive monolayer with honeycomb pattern, occasional papillary/intact villi, smaller groups or single cells nonmucinous glandular cells with brush border sporadically placed goblet cells "fried eggs" "sesame seeds" intraepithelial lymphocytess stomach: small sheets and strips, occasional isolated cells and gastric pits visible mucin (foveolar cells) grooved naked nuclei |
|
|
|
1. What type of epithelium lines branch duct IPMNs? 2. From what is the above impossible to differentiate? 3. In the US what is the most common cause of acute pancreatitis and what is the physiology and FNA appearance?? 4. Why is chronic pancreatitis more often seen on FNA? 5. What etiology of the above is important to recognized and why? |
1. gastric foveolar type cells (which are mucinous so helps ID this over duodenal contaminant which also has IELs) 2. normal stomach! if a low grade lesion 3. alcohol, enzymatic autodestruction; FNA shows necrotic debris with degenerating cells, foamy histiocytes, fat necrosis, calcifications and acute inflammation 4. b/c of mass forming fibrosis seen radiologically mimicing neoplasm 5. autoimmune (lymphoplasmacytic sclerosing) b/c it can be treated with corticosteroids not surgery!!! |
|
|
|
1. What is the cytomorphgology of chronic pancreataitis w/ reactive ductal atypia? 2. What clues suggest autimmune pancreatitis? |
1. low cellularity background inflammation, fat necrosis, calcific debris cellular stromal fragments (especially in autoimmune) flat, cohesive sheets with evenly spaced or slightly crowded nuclei absent or rare isolated atypical cells uniform enlarged nuclei (<4:1 diameter ratio in same sheet) round to oval nucleus and smooth nuclear membranes prominent nucleoli but NOT macronucleoli occasional mitoses low N:C ratio 2. hypocellularity, cellular stromal fragmentswith crush artifact, chronic inflammation with plasma cells |
|
|
|
1 In what situations should one have a high threshold for calling malignancy on brushings? 2. What stains may be helpful in identifying pancreatic ACA versus reactive atypia (e.g. in chronic pancreatitis)? 3. Describe the types of pancreatic intraepithelial neoplasia. |
1. PSC, PBC, stones or indwelling stents 2. SMAD4 is lost in half of pancreatic adenocarcinomas and p53 is positive in most 3. PanIN-1: low grade PanIN-2: moderate, with tufting, nuclear stratification but maintained polarity PanIN-3: malignant appearing cells confined to duct |
|
|
|
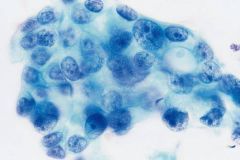
pancreatic ductal ACA 2. What is the patient population and presentation? explain. 3. What is a well known risk factor? 4. What is the cytomorphology? |
1. the most common one in the pancreas! 85-90% of all neoplasms 2. 60-80 year old patients with a pancreatic head mass (60-70%) causing a constriction that dilates the main and pancreatic bile ducts "double duct sign" 3. Smoking1 4. moderate/high cellularity irregular size and shaped clusters AND isolated malignant cells uneven distribution of ductal cells in a sheet "drunken honeycomb" irregular nuclear contours enlarged nuclei >4:1 diameter w/in a single sheet irregular chromatin with clumping and parachromatin clearing scant or abundant mucinous cytoplasm |
|
|
1. What two features of malignancy are highlighted on cell block? 2. What is the DDX of ductal ACA? 3. List two mimics of the above and describe what helps identify them. 4. What are the more reliable indicators of malignancy? 5. Besides possible differentiation of reactive versus malignant, for what is SMAD4 useful? |
1. desmoplasia and cribriforming 2. chronic pancreatitis especially autoimmune radiation changes reactive/reparative atypia metastatic ACA 3. radiation and chronic pancreatitis which have background elements like fat necrosis, calcification, inflammatory debris 4. high N:C ratio, nuclear membrane irregularity, isolated atypical cells and >4 fold anisonucleosis 5. SMAD4 is lost in pancreatic ACA but NOT metastasis! (not lost in ovary, colon endometrium or lung) |
|
|
|
1. What mutation may be helpful in identifying malignancy? 2. What are the two most common variant of pancreatic ductal ACA? 3. What mutations are seen and in which variant? 4. List 4 other variants. |
1. KRAS sorta b/c it is found in about 50% of PanIN-1 and increases with increasing degree of dysplasia 2. adenosquamous (3-4%) and undifferentiated/anaplastic (0.3-10%) 3. KRAS is seen in 90% of the mononuclear component (also has giant cells) of anaplastic TP53 mutations seen in 50% 4. colloid, hepatoid, medullary and signet ring |
|
|
|
1. What are other names for pancreatic neuroendocrine tumors (PanNET)? 2. How common are they? 3. What is the definition of a high grade tumor (per WHO 2010)? 4. What do functional PanNETs secrete? |
1. islet cell tumor, pancreatic endocrine neoplasm, pancreatic endocrine tumor 2 UNcommon at 1-2% of all pancreatic neoplasms (less than the ACA variants) 3. >20 mitoses per 10 HPF 4. insulin, glucagon, somatostatin, vasoactive intestinal polypeptide, pancreatic polypeptide, serotonin, adrenocorticotropic hormone and calcitonin |
|
|
|
1. Which PanNETs usually follow a benign course? What material is seen in these? 2. What is the clinical course of the others? 3. What is the patient population? 4. What re the most reliable indicators of malignancy? 5. What is the reporting terminology on FNA? 6. Which kind of PanNET often form psammoma bodies? |
1. insulinomas, and <1cm often; somtimes have amyloid 2. aggressive 65-80% with uniquivocal features of malignancy 3. adults, average age 40, small circumscribed masses 4. mets or invasion of adjacent structures 5. neoplastic cells present with classification done on histology 6. somatostatinomas |
|
|
|
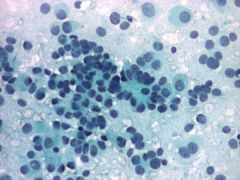
PanNET 1. What is the cytomorphology? 2. What can be seen in the cytoplasm on Romanowsky stain? 3. How is the mitotic rate/Ki67 index used to grade these tumors? 4. Which specimens are used for grading? |
1. highly cellular with solid-cellular smear pattern pedominantly isolated cells and bare nuclei pseudorosettes and small clusters uniform round/oval nuclei eccentric nuclei/plasmacytoid fine stippled "salt and pepper" chromatin moderate/abundant cytoplasm usually granular ill defined cell borders (can be oncocytic or vacuolated e.g. lipid rich) 2. red granules 3. low: <2/10 mits/HPF <3%Ki67 intermediate: 3-20/10 mits/HPF 3-20%Ki67 high: >20/10 mits/HPF >20%Ki67 4. core biopsies BUT with the caveat that higher grade focus may not have been sampled |
|
|
1. What is the DDX of well differentiated/low grade PanNET? 2. What are 2 relatively specific IHC markers for PanNET that can help distinguishe it from GI NET mets? |
1. Acenar cell carcinoma (ACC) Solid pseudopapillary neoplasm (SPN) metastatic neuroendocrine carcinoma non-Hodgkin lymphoma melanoma plasmacytoma metastatic renal cell carcinoma pancreatoblastoma 2. Islet 1 and PAX-8 |
|
|
|
SEE TABLE 14.2 ON PAGE 410 FOR IHC PROFILES OF PANCREATIC TUMORS |
SEE TABLE 14.2 ON PAGE 410 FOR IHC PROFILES OF PANCREATIC TUMORS |
|
|
|
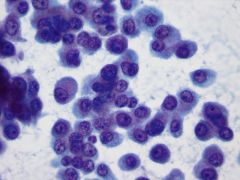
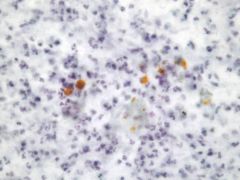
Acinar cell carcinoma 1. How common is this? Prognosis? 2. What is the cytomorphology? 3. What is a distinct background features that helps one identify ACC? |
1. < 2% of pancreatic exocrine tumors; poor with <10% 5 year survival 2. highly cellular solid-cellular pattern of monomorphic cells (numerous isolated, loose aggregates, naked nuclei, loose granules in background) round/oval nuclei smooth nuclear contour prominent nucleolus delicate granular cytoplasm 3. spilled zymogen granules (hence naked nuclei) |
|
|
1. What two stains highlight the cyctoplasmic granules in ACC? 2. What IHC is positive? name the most specific marker. 3. What is the DDX? |
1. PAS and toludine blue 2. pancreatic enzymes: trypsin (most specific), lipase chymotrypsin and phospholipase A2 3. benign acinar cells PanNET solid peudopapillary neoplasm (SPN) |
|
|
|
1. How is SPN differentiated from ACC? 2. What is a main difference in how SPN stains ? 3. What is the distinguishing marker of SPN? |
1. SPN has small chromocenters not large nucleoli and scant ill defined cytoplasm (versus abundant in ACC) 2. SPN are cytokeratin negative! whereas ACC and PanNET are CK+ 3. nuclear positivity for beta catenin |
|
|
|
Solid Pseudopapillary Neoplasmm (SPN) 1. How common is this tumor? 2. What is the patient population? 3. What is the prognosis? 4. On imaging, how is this tumor differentiated from MCN? |
1. NOT only 1-2% of pancreatic exocrine neoplasms 2. 90% in young women mean age 28! 3. good, most treated successfully with conservative surgical resections having low malignant potential 4. MCN has septations in its cysts and SPN does not (but both cystic pancreatic lesions in young women!!!) |
|
|
1. What is the cytomorphology of SPN? 2. What is the IHC profile? 3. What is the molecular alteration that leads to what characteristic staining pattern? |
1. monomorphic highly cellular aspirate with solid-cellular pattern mycoid or hyalinized vascular stalks liked by neoplastic cells delicate finely vacuolated cytoplasm with indistincct cell borders (perinuclear vacuoles, PASD + hyaline globules) round/oval with nuclear grooves inconspicuous nucleoli foam cells and necrotic debris 2. + alpha1 antitrypsin, progesterone receptor, CD56, CD10 and CD117 (CKIT) 3. alteration in APC/beta catenin pathway causing cytoplasmic AND nuclear accumulation of this protein in 95% of SPN causing nuclear + beta-catenin |
|
|
|
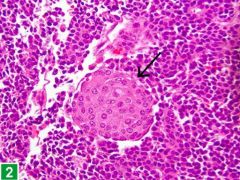
Pancreatoblastoma 1. What is the patient population? how common? 2. What is the cytomorphology? 3. What is the diagnostic feature? it's staining pattern? |
1. young children, rare tumor but the most common malignant pancreatic neoplasm of childhood 2. epithelial: syncitial groups and isolated cells monomorphic cell with moderate cytoplasm squamoid corpuscle stromal: primitive spindle-shaped cells +/- heterologous elements (e.g. cartilage) 3. the squamoid corpuscle! often NOT immunoreactive but may show focal CK/endocrine or CEA |
|
|
1. What is the DDX of pancreatoblastoma? 2. How common are pancreatic cysts? 3. What causes pseudocysts? |
1. ACC PanNET SPN Wils tumor neuroblastoma 2. 1-2% of general population and up to 8% of elderly have them 3. autodigestion of pancreatic parenchyma (often in acute pancreatitis) |
|
|
|
Pseudocyst 1. What does the cyst fluid analysis show? 2. What is the cytomorphology? 3. What cells may be present and should not be confused as cyst lining cells? |
1. very high amylase (in the thousands) and CEA NOT elevated 2. thin, non mucinous cyst fluid mixed inflammatory cells and histiocytes yellow hematoidin-like pigment no epithelial cells 3. normal pancreas ductal and/or acinar cells, fibroblasts, mesothelial cells, gastric cells or duodenal cells |
|
|
serous cystadenoma 1. How common is this? 2. What are the subtypes? 3. What is the patient population and location? 4. What is commonly seen on imaging? |
1. NOT, accounts for 1-2% of pancreatic tumors 2. microcystic: numerous small cysts (more common) oligocystic: few large cysts 3. W>M average 66 yrs, body and tail of pancreas; oligocystic can be seen in kids 4. a central stellate scar in 30-40% |
|
|
1. What is the cytomorphology of serous cystadenoma? 2. What stain is positive? 3. What does cyst fluid analysis reveal? 4. What is the DDX? |
1. sparse cellularity clean or bloody background flat sheets and loose clusters cuboidal cells clear finely vacuolated or granular cytoplasm with indistinct borders bare nuclei small round nucleus fine chromatin inconcpicuous nucleolus +/- hemosiderin laden macrophages 2. PAS + diastase sensitive b/c the cytoplasm is filled with glycogen 3. low amylase and low CEA 4. benign pancreatic ductal and acinar cells lymphangioma and hemangioma mucinous cystic neoplasm with low grade dysplsia cystic PanNET multicystic mesothelioma metastatic RCC |
|
|
|
lymphoepithelial cyst 1. What is the patient population in this rare benign lesion? 2. What is the cytomorphology? 3. What is the DDX? |
1. middle aged men 4:1 M to F ratio 2. anucleate squames and abundant keratinaceous debris mature superficial squamous cells lymphocytes +/- cholesterol crystals 3. complicated pseudocyst dermoid and epidermoid cyst |
|
|
Mucnous cystic neoplasm 1. How common is this? 2. What is the patient population? 3. What is the defining histologic feature and stains? 4. How is this cytologically differentiated from IPMN? |
1. 5% of pancreatic neoplasms 2. almost exclusively in women, average age 49in the body or tail of pancreas 3. ovaian type stroma that is ER/PR positive 4. it is NOT, the distinction between the two is not possible on cytology alone |
|
|
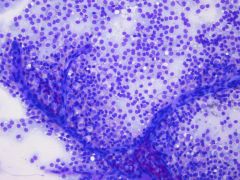
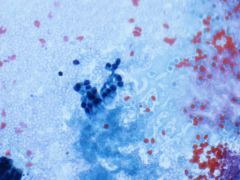
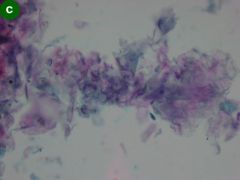
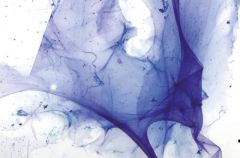
Thick colloid like mucin from MCN 1. What is the cytomorphology of IPMN and MCN? |
1. hypocellular
variable extracellular mucin thick colloid like mucin +/- cyst lining (diagnostic of mucinous cyst!) low grade dysplasia (benign appearing mucinous epithelium in sheets and groups, often indistinguishable from gastric epithelium) high grade dysplasia (small tight bud like clusters or isolated cells with increased N:C ratios irregular nuclear membranes and variably vacuolated cytoplasm) malignant (3D groups with marked anisonucleosis, irregular nuclear membranes prominent nucleoli, parachromatin clearing and necrosis) cellular debris/necrosis |
|
|
1. How common is intraductal papillary mucinous neoplasm (IPMN)? 2. How do these different in their growth pattern from MCN and ACA? 3. What is the patient population and location? 4. What are the 3 types? |
1. 3-5% of pancreatic tumors 2. IPMN are "open ended" neoplasms that grow intraluminally in the pancreatic ducts (MCN does not communicate with ductal system at all) 3. M=W, 70% in head of pancreas 4. involving main pancreatic duct only involving branch ducts only involving both |
|
|
|
1. What imaging finding is pathognomonic for IPMN? 2. What type of lining is seen in main and branch duct IPMNs and why is this important? 3. What is the main task for the cytologist? |
1. copious mucin spilling from ampulla 2. main: intestinal type, carries higher risk of malignancy! branch: gastric does not have same risk as intestinal 3. to identify high grade dysplasia or carcinoma b/c low grade dysplasia versus GI contamination cannot be determined on cytology in most cases (small branch duct with no high grade can be followed instead of surgery) |
|
|
|
1. What preparation makes identification of mucin difficult? 2. What can help the above? 3. What terminology is used to denote a high grade lesion and why? 4. What data is essential to diagnosis of mucinous cysts? Explain. 5. How is GNAS useful? |
1. Liquid based preparation 2. make cytospin slides to do an Alcian blue pH2.5 or mucicarmine on (but negative does not exclude a mucinous neoplasm!!) 3. high grade atypia which encompasses high grade dysplasia and carcinoma because its difficult do distinguishe between the two on cytology. 4. cyst fluid analysis CEA: best at detecting mucinous cyst but cannot determine malignancy (need cytology) KRAS point mutation or LOH: helps diagnose mucinous cyst if CEA is low, also does not detect malignancy 5. it's positive in IPMN but not in MCN, which directs management because all MCN are resected (regardless of grade) but NOT all IPMNs are resectedd |
|
|
|
1. Which neoplasms most often metastasize to the pancreas? 2. Which malignancy is the most common mimic of primary pancreatic neoplasm? What is the DDX? 3. What ectopic tisue is encountered in pancreas that mimics PanNET on imaging?What is the cytomorphology? 4. What is very helpful to identify the above? |
1. lung, breast, kidney and lymphoma 2. renal cell carcinoma; lipid rich PanNET 3. spleen! should be considered when nnumerous lymphocytes are seen 4. cell block sections showing characteristic thin walled blood vessels that are CD8+ |
|