Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
Autocrine
Paracrine Endocrine cell cell communication examples |
- Signaling chemicals coming from a cell act on their own
receptors (e.g., norepinephrine acting on the presynaptic receptors and cytokines acting on lymphocytes). -Signaling chemicals influence the function of neighboring cells and cells present in the close vicinity (e.g., histamine, serotonin). -Signaling chemicals are carried to the distant sites and act on discrete organs (insulin, estrogen, testosterone, etc.). -Direct communication occurs through interaction of signaling molecules anchored on the cell membranes CTcell-B cell interaction, HIV [gp120J-T cell [CD4J interaction). |
|
|
receptors?
throxine, hydrothyronine? estrogen? loose receptor example |
- extracellular, plasma bound, intracellular
- binds all receptors - only bind intracellular - TBG, ANP-C, IgG |
|
|
affinity
intrinsic activity agonist antagonist partial agonist |
- persistent ability with which the
drug binds to the specific receptors on the cell membrane - The intrinsic activity of a drug is the inherent property of the drug to impart biological signals -drugs that can produce the maximal response in any given tissue are termed full agonists -antagonists can have full (1.0) affinity, but their intrinsic activity is Always zero (0). -can bind with full affinity, the same as a full agonist, but can produce only a partial effect |
|
|
differential effects of epinephrine
receptor and function lungs ateries heart eye hair viens |

blocker B2 - methoxanine ?
|
|
|
agonist and antagonist
adrenergic alpha |
alpha 1
phenylephrine antag Phentolamine Tolazoline Prazosin alpha 2 clonidine antag Phentolamine• Tolazoline Yohimbine |
|
|
agonist and antagonist
adrenergic beta |
beta1
isoproterenol dobutamine antag Propranolol Timolol Metoprolol Atenolol beta 2 isoproterenol terbutaline antag Propranolol Timolol Butoxamine |
|
|
bradycardia
tachycardia |
- constricted
- dialated, isoproterenol, B1 |
|
|
heteroreceptors!
potentiate adrenergic stim ? blocker? control diaherria? |
angiotensin II
neuro peptide y diphenoxylate binds adropine? |
|
|
flow chart
acetylcholine lung gentitals heart GI tract bladder lacrimal eye ateries sweating |

|
|
|
dry mouth, dry skin, tachycardia- meds
|
adropine
|
|
|
know different receptors, second messengers w/ Alpha, beta, M1, M2, M3
|
a
|
|
|
direct acting cholinomimetics
indirect acting block |
bind to receptors,
- acetylcholine esterase |
|
|
cholinergic Muscarinic ag antag
|
M1
carbachol antag atropine pirenzepine M2 carbachol antag atropine M3 antag atropine |
|
|
cholinergic nicotinic ag antag
|
Nn
antag HexaMethonium Nm antag Tubercurarine succinylcholine |
|
|
atropine effects
diphenoxylate binds atropine diphenoxynate |
dilate pupil-> not completely artopine and phenylephrine
M1 opiate receptor , block acetylcholine release thro M1 |
|
|
phenoxylbenzamine
|
permanent bind alpha 1
dilate pupil |
|
|
Atropine effects
|
• (Mydriasis): temporary pupil dilation
• GI tract: decreased muscle actions and secretions • Bronchiolar smooth muscle: decreased muscle actions and secretions (asthma) • Brain: Blockage of CNS receptors (Parkinson’s, motion sickness) • Urinary bladder: Relaxation of detrusor muscle and constriction of spincter (urinary incontinence) • Heart: Tachycardia (M2 blocker SA node) • Salivary glands: decreased saliva secretion • Sweat glands: decreased sweating |
|
|
inhibitors?
cooperatively req? |
competitive, un, non inhibition(allosteric)
multiple subunits |
|
|
acetylcholineesterase inhibitors
myestinia gravis treating glacoma |
- edrophonium for diagnosis, neostigmine, physostigmine
-important acute or chronic (C- timinol, A- vilocarpine, physostigmine) indirect cholinomamatics |
|
|
condition pupil dialated
aqueous humor release -treat with |
timinol and another one (pupil hint)
|
|
|
Prevent organophospahte bond
|
-PAM, pralidoxime
|
|
|
nerve gas
first thing then |
-atropine
- physostigmine, neostigmine |
|
|
Penicillins
which enzyme inhibited |
- transpeptidase
-cuz 2 B alanines |
|
|
which kill gram -ve
|
-amox, ampi
|
|
|
penicilinase resistant
|
-methi
-nafi -oxa -cloxa -dicloxa |
|
|
know combos
Augmentin Unasyn |
-amox + clavulanic acid
-ampi + sulbactum timentin? |
|
|
which enzyme produce 6-aminopenicillinic acid (6-APA)
beta-lactamase produce |
- bacterial penicillin amidase
-penicilloic acid |
|
|
5-florouracil inhibiting thymidine synthase
|
for rectal cancer
-fDUMP |
|
|
xanthine oxidase inhibitor
|
treat gout
-allopurinol, suicide |
|
|
receptor theories
clarks assumptions are |
-stimulus is elicited when receptor molecule occupied by agonist
-drug-receptor complex formed readily and is rapidly reversible -maximal stim occurs when all sites occupied -occupation of one does not affect the tendency of others to be occupied |
|
|
PD2 value-
|
-affinity of ligand for receptor
- log Kd conc |
|
|
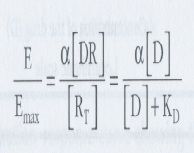
calc intrinsic activity aka alpha
|
|
|
|
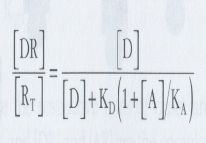
Gaddum eq.
|
|
|
|
rate theory
antagonist agonist partial?? |
by Paton
rate 0 rate max acybutanol, betalol?? |
|
|
dose response curve if shift right?
|
-antagonist present, need more conc for same effect, Kd value increase w/ comped. antag
|
|
|
pA2 vs pA10 which smaller
comp. antag |
-PA10
-change .95 |
|

kind of inhibtor
difference of low conc vs high |
w/ non comp. antag
shifting right at low, Kd increaing Emax decreasing high doses, |
|
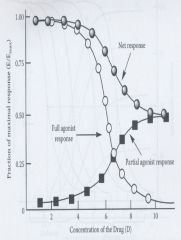
what the hell is this what does it tell us
|
partial + full agonist/ partial effect at full conc.
dose relation Kd (sumthin bout this) |
|
|
select preferred drug from graphs
|
max efficicacy, max potency
|
|
|
therapeutic index
first dose producing max effect |
- calc ratio Ld50/Ed50
- ceiling dose |
|
|
conc drug 1/3 of Kd effect is total # receptors?
|
D / Kd +D
|
|
|
tolerance
tachyphylaxis |
-gradual decrease in effectiveness of drug over long time period
-loss of response on repeated administration -ex angiotensin II |
|
|
how fast is each type response
ion channels steriods DNA second messenger kinases |
-ion channels- milliseconds
-second messengers- seconds -kinases -minutes -steriods and DNA- hours |
|
|
know secondary messengers
2nd messengers good for |
-cAMP, cGMP, Ca++,
arachidonic acid, 4,5-phosphoinositol, 4,5-biphosphate (PIP2), Inositol 1, 4, 5-triphosphate, 1, 2-diacylglycerol -amplifying |
|
|
heat shock protein 90
|
inactivates steroid receptor until ligand binds- then transcription
|
|
|
phosphorlation and consequences
|
- activate, inhibit
-ex. glycogen synthesis controlled by both, (lots Ca degradation) |
|
|
EGF receptor
|
-dimerization triggered by EGF
-autophos happens -phosphorlates other crap |
|
|
phos or nonphos--> Beta arrestin binds which
|
-phos
-phos kick off Gs -Gs protein inhibited until unphos |
|
|
activating guanylate cyclase activity
|
-GC activated by ANP binding ANP receptor
-on inside GC, make cGMP from GTP then dilate -this how NO works |
|
|
3 units of G protein, where bind
|
-alpha, beta, gamma
-bind alpha -if alpha s, make cAMP, if alpha i inhibit AC |
|
|
Na, K gating, potential range for gates
|
Na- inactive -90mV inside open
-activated (-90- +35mV) both open -inactivated (-90 - +35mV) inside closed, out open K- same as Na but... -open just as Na is closing |
|
|
nicotine bind ______open Na channel, where bind
|
-nicotinic receptor
-subunits 5 -2 alpha, beta, gamma, delta -binds alpha |
|
|
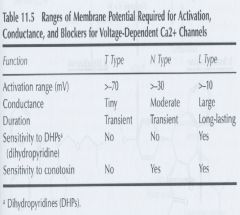
channel typpes, potential ranges, tests to determine channel
|
|
|
|
GABA complex
|
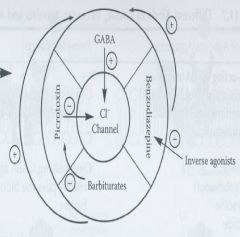
-open Cl- channel, hyperpolarize
|
|
|
GABA complex
benzodiaziphone Barbituate |
-potentiate effect
-open channel more freq, - long last current -both +ve allosteric, coop |
|
|
GABA antagonist
inverse agonist |
-bicululline (comp),
-picrotoxin (noncomp), directly inhibit channel bind benzodiaphine decreasing opening |
|
|
Barbituates
|
-potentiate GABA effect
-allosterically relieve picrotoxin inhibited channel |