![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
96 Cards in this Set
- Front
- Back
|
Define parakeratosis |
Keratinisation characterised by retention of nuclei in stratum corneum |
|
|
What causes acanthosis? |
hyperplasia of stratum spinosum |
|
|
What causes elongated rete ridges? |
hyperplasia of basal cells |
|
|
Define atrophy |
Reduction in viable layers |
|
|
Define erosion |
partial thickness loss |
|
|
Histologically, what is ulceration? |
full thickness loss with fibrin on surface |
|
|
what is spongiosis? |
intercellular oedema (between cells) |
|
|
Define dysplasia |
disordered maturation (growth) in a tissue |
|
|
Give the known causes of oral keratoses (white patches) |
1. Hereditary 2. smoking/frictional 3. Lichen planus 4. Lupus erythematosus 5. candidal leukoplakia 6. carcinoma |
|
|
Define leukoplakia |
a white patch which cannot be scraped off or attributed to any other cause |
|
|
define erythroplakia |
red patch which cannot be rubbed off or attributed to any other cause atrophic/non-keratotic end of spectrum |
|
|
What is the difference between orthokeratosis and parakeratosis? |
Orthokeratosis - hyperkeratosis with no nuclei in the cells Parakeratosis - retention of nuclei in stratum corneum (keratin layer) |
|
|
Define atypia |
structural changes in a cell |
|
|
Give an example of hereditary keratosis |
1. White sponge naevus - intracellular oedema in keratin layer and prickle cell layer 2. Fordyce's spots - sebaceous glands |
|
|
Frictional / smoker's keratosis management |
1. remove cause 2. reassure 3. splint therapy (if parafunction) |
|
|
Management of a lesion with: 1. Mild dysplasia? 2. Moderate? 3. Severe? |
1. observe/re-biopsy 2. remove 3. remove |
|
|
what is the difference between lichen planus and a lichenoid reaction? |
lichen planus - chronic autoimmune disease Lichenoid reaction - known cause |
|
|
1. What is lupus erythematosus? 2. What are the oral and non-oral signs? |
1. Autoimmune CT disease 2. Oral: red with white striae - esp. palate Non-oral: skin rash - esp. on face |
|
|
Give the localised causes of pigmented lesions |
1. amalgam tattoo 2. malignant melanoma 3. macule / naevus 4. peutz-jehger's syndrome 5. pigmentary incompetence 6. kaposi's sarcoma |
|
|
Give the generalised causes of pigmented lesions |
1. Addison's disease 2. Drugs 3. Racial / familial 4. Smoking |
|
|
Give two exogenous sources of oral pigmentation |
1. Amalgam tattoo 2. heavy metal poisoning - lead |
|
|
Give two endogenous sources of oral pigmentation |
1. melanin 2. haemosiderin |
|
|
What stain is used for the identification of candida? |
Periodic Acid-Schiff (PAS) |
|
|
Give five sources of melanin pigmentation |
1. physiological - racial 2. melanotic macule 3. melanotic naevus - mole 4. secondary melanosis (reactive) - smoking, inflam. , drugs - Addison's disease 5. malignant melanoma |
|
|
What is a mucosal melanoma? |

- potentially malignant lesion - increase in number of melanocytes |
|
|
What is a haemangioma? |

- hamartoma - growth of endothelial cells - rapid growth during first few weeks of life - usually regress over first 10 years |
|
|
What is a vascular malformation? |

- congenital growth, made up of arteries, veins, capillaries, or lymphatic vessels - present at birth and persist during life - may become noticeable in elderly - intraosseous malformations may occur |
|
|
What are the types of vascular malformation? |
- capillary - cavernous - sturge-weber syndrome - port wine stain |
|
|
What is geographic tongue? |

- benign migratory glossitis - irregular, smooth red patches on parts of tongue - desquamation of filiform papillae 1-2% of population |
|
|
What is black hairy tongue? |

- hyperplasia of filiform papillae - ineffective desquamation of papillae - bacterial pigment |
|
|
What is the difference between a hemangioma and a vascular malformation?
|
- Most hemangiomas are not usually present at birth or are very faint red marks. Shortly after birth they grow rapidly - often faster than the child's growth. Over time, they become smaller (involute) and lighter in color. The process of involution may take several years.
- Vascular malformations are present at birth and enlarge proportionately with the growth of the child. They do not involute spontaneously and may become more apparent as the child grows. |
|
|
What can the origins of an acquired lesion be? |
Vascular Infective Inflammatory Traumatic Autoimmune Metabolic Idiopathic Iatrogenic Neoplastic |
|
|
What does pedunculated mean? |
The mucosal swelling has a 'stalk' |
|
|
What does sessile mean? |
The swelling has a flat, long base |
|
|
what is the origin of fibrous lesions? |
collagen |
|
|
What is a fibrous epulis? |

- fibrous overgrowth of gingiva - localised gingival hyperplasia - usually due to sub-gingival calculus |
|
|
What causes pregnancy gingivitis? |
- HORMONAL - Exaggerated response to plaque |
|
|
Which drugs can cause gingival hyperplasia? |
1. antihypertensives - Ca channel blockers 2. Antiepileptics - phenytoin 3. Immunosuppressants - cyclosporin |
|
|
What is a 'leaf fibroma'? |

- Fibrous overgrowth caused by denture trauma - becomes squashed under denture - flat with stalk |
|
|
What is papillary hyperplasia of the palate? |
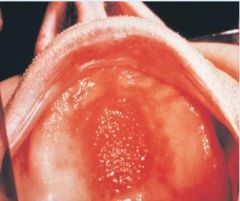
- pseudo-epitheliomatous hyperplasia - ?candida infection - ?denture trauma - ? wearing denture at night - lumpy palate |
|
|
What is a fibro-epithelial polyp? |

- fibrous overgrowth on lip/cheek/tongue - quite pale - covered in keratinised epithelium |
|
|
What is a pyogenic granuloma? |

- exaggerated trauma response - granulation tissue - any mucosal site - lots of BVs |
|
|
What are the other names for a pyogenic granuloma? |
1. vascular epulis 2. pregnancy epulis (if during pregnancy) |
|
|
In the case of giant cell lesions what must be excluded? |
Systemic disease: Raised parathyroid hormone - low vit D in diet - malabsorption - renal disease |
|
|
What are the causes of giant cell lesions? |

- local chronic irritation - infective agents eg TB - difficult to get rid of, need giant cells - hormonal stimulation of cells - osteoclasts |
|
|
Difference between tori and osteomas? |
tori - developmental abnormalities - palate or lingual premolar region - ususally summetrical osteomas - acquired in reaction to something - other sites to tori |
|
|
how does orofacial granulomatosis cause swelling? |
inflammatory change -> granulomas -> block off lymphatic drainage -> oedema |
|
|
What type of hypersensitivity is OFG related to? |
Type IV - slow build |
|
|
What are the oral signs of crohn's disease? |
1. lip fissure 2. apthous ulceration 3. mucosal tags 4. fistula formation 5. tissue swellings 6. Full thickness ulceration 7. Buccal cobblestoning Angular cheilitis |
|
|
Name some of the dietary allergens related to OFG |
- benzoates - cinnamonaldehyde - sorbic acid - chocolate |
|
|
How would you diagnose a dietary allergy? |
Patch testing Trial exclusion diet for 12 wks |
|
|
Management of OFG |
- dietary avoidance - Abx - macrolides - erythromycin - topical tacrolimus ointment to lips - intra-lesional steroid injections - oral steroids - biologics eg adalimumab |
|
|
If the apparent source of a traumatic ulcer has been removed but the ulcer is still present after 3 weeks what is the next step? |
REFER |
|
|
What drug can cause recurrent oral ulceration? |

NICORANDIL - anti-anginal - < dose, < ulceration **LIASE WITH CARDIOLOGIST** |
|
|
Minor apthae: -shape -size -number -mucosa affected -duration -outcome |

- shape: oval/round, regular red 'halo' border, yellow slough in centre - size: <10mm - number: 1-20 per crop - Affects: chiefly non-keratonising mucosa - Duration: heal 1-2 wks - outcome: heal without scarring |
|
|
Major apthae:
-shape -size -number -mucosa affected -duration -outcome |

-shape: oval/irregular
-size: >10mm -number: <5 at a time (esp soft palate) -mucosa affected: keratinising OR non-keratinising -duration: heal 6-12 wks -outcome: Heal with/without scarring |
|
|
Herpetiform apthae:
-shape -size -number -mucosa affected -duration -outcome |

-shape: round/oval, often coalesce into large ulcerated areas
-size: <5mm -number: 1-200 per crop -mucosa affected: non-keratinising -duration: heal 1-2 weeks -outcome: heal without scarring *NOTHING TO DO WITH HERPES - NON-VIRAL* |
|
|
Describe the signs of behçet's syndrome |
- oral ulcers - genital ulcers - skin pustules - eye disease - arthritis - neurologic disease - GI disease |
|
|
If recurrent ulceration is self-healing and affecting only the non-keratinised mucosa what must it be? |
Apthae |
|
|
Give the host aetiological factors of recurrent apthae |
- genetic - nutritional deficiencies - iron, folate, B12 - systemic disease- blood loss, malabsorption, ulcerative collitis - endocrine- remission in pregnancy - immunodeficient |
|
|
Give the environmental aetological factors of recurrent apthae |
- trauma- LA site may ulcerate in predisposed - allergy- dietary, SLS - infection? - stress? |
|
|
What habit suppresses recurrent apthae and why? |
Smoking Suppresses immune surveillance |
|
|
Treatment for recurrent apthae |
- correct deficiency - correct systemic disease - remove trauma - remove allergens/SLS |
|
|
Medication for recurrent apthae |
topical immune modulation - betamethasone m/w (0.5mg 2-3x daily) - beclometasone inhaler (50micrograms 2-3x daily) Systemic immune modulation - systemic steroids - azathioprine |
|
|
How does lichen planus appear on skin? |

itchy papules with white lacy appearance on flexor surfaces |
|
|
How does lichen planus appear on the mucosa? |
White on cheek (most often), tongue, gingiva |
|
|
What are the 7 varieties of oral lichen planus? |
1. Reticular- webby 2. papular - papules - spotty 3. Plaque - big patch, tends to occur on tongue 4. Atrophic 5. Erosive (ulcerative) 6. Bullous 7. Desquamative gingivitis |
|
|
What is the aetiology of lichen planus? |
- autoimmune - idiopathic - hep C (not uk) - drugs - ß-blockers, diuretics - amalgam - plaque - SLS |
|
|
Lichen planus histological characteristics |
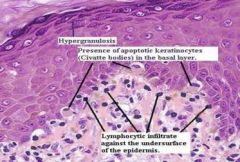
- keratinisation - atrophy/hyperplasia - band of chronic inflammatory cells - lymphoctes and macrophages - basal cell liquefaction - Apoptosis - saw tooth rete ridges |
|
|
Drugs in lichenoid tissue reactions |
- NSAIDs - Antihypertensives eg beta blockers - Hopoglycaemics - diuretics eg bendroflumethiazide |
|
|
Lichen planus management |
Asymptomatic - observe and CHX Symptomatic - remove cause - SLS free tp -topical steroids - systemic steroids - systemic immune modulation - azathioprine *SMOKING MUST STOP* |
|
|
what percentage of lichen planus may become malignant, what sites are often involved and which patient groups are most at risk? |
- 1% - tongue, gingivae - severe LP, immunosuppressed, smokers, erosive LP |
|
|
When should you biopsy lichen planus? |
- biopsy all types in smokers - symptomatic/erosive types in everyone |
|
|
what does multiforme mean? |
Various presentations |
|
|
What are the features of erythema multiforme? |
- skin - target lesions - mucosa - ulcers - recurrent within short period - lips + ant. mouth - crops, heal 2 wks - unable to eat/drink - dehydration |
|
|
Histology of erythema multiforme |
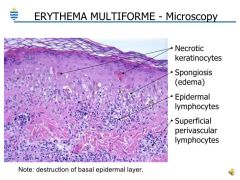
- intracellular oedema and necrosis = intraepithelial vesicle - inflammation |
|
|
Erythema multiforme management |
- high dose systemic steroids - systemic acicilovir - encourage fluid intake - possibly IV - analgesia - allergy testing/daily aciclovir if recurrent |
|
|
How does a blister form? |
- auto-antibody attack on skin components - loss of cell-cell adhesion (desmosomes/hemidesmosomes) - split forms in skin - fills with inflammatory exudate - forms vesicle/blister |
|
|
Describe pemphigoid |
- sub-basal antibody attack - thick-walled blisters (full epidermis lifted from CT) - blood filled blisters - can occur mouth, eyes, genitals - may scar (cicatritial) - WATCH EYES |
|
|
Pemphigoid management |
- immunosuppression - steroids/immune-modulation |
|
|
Describe pemphigus |
- intra-epithelial bullae - clear fluid filled blisters which burst and spread - supra-basal split - rarely see intact bullae - surface easily lost - FATAL without tx if full body - fluid loss |
|
|
Difference between pemphigus and pemphigoid? |
- Pemphigus affects desmasomes
- Pemphigoid affects hemi-desmasomes - basal cell layer remains attached to CT - attached side are hemi-desmasomes which remain unnafected in pemphigus |
|
|
Describe angina bullosa haemorrhagica and management |
- blood blisters in absence of trauma - affect palate but any oral site - advise pts to de-roof blisters |
|
|
What are the virulence factors of candida? |
- adherence - switching mechanisms - germ tube formation - extracellular enzymes - acidic metabolites - push tissues out of way - tissue destructive enzymes bury deep into tissues - underlying immunosuppression? |
|
|
What are the local predisposing factors for fungal infections? |
- Abx - dentures - local corticosteroids - xerostomia |
|
|
general predisposing factors for fungal infections? |
- extremes of age - endocrine disease - diabetes - immunodeficiency - nutritional deficiency - iron - smoking - local immunosuppression, mouth dryness |
|
|
describe pseudomembranous candidosis |

white plaques, can be removed easily to leave red bleeding patches underneath |
|
|
describe erythematous candiosis and possible causes |

- red - abx stomatitis - denture stomatitis - think diabetes/HIV/ immunosuppression in young and otherwise healthy pt |
|
|
Describe median rhomboid glossitis and the 3 causes |
- area of depappillation caused by erythematous candiosis in middle of tongue towards back
- Causes: diabetes, smoking, HIV |
|
|
Describe angular cheilitis and causes |
- inflammation and cracking at corners of mouth - reduction in OVD - often mix of candida and S. aureus |
|
|
Describe hyperplastic candidosis and management |
- found only at commissures of lips - found in smokers, diabetics - may be dysplastic changes - potentially malignant - STOP SMOKING - BIOPSY |
|
|
Treatment of oral fungal infections |
- OH measures - denture hygiene, rinse after inhaler - Diet esp carbs - Trauma - antifungals - bloods - deficiency states - smoking cessation |
|
|
Which common drug can miconazole interact with if used topically? |
Warfarin |
|
|
How long does topical antifungal therapy take and which drugs can be prescribed? |
- 28 days - Miconazole cream/gel - Nystatin drops |
|
|
Which drugs are used for systemic antifungal therapy? |
- Fluconazole - Itraconazole |
|
|
what is the drug of choice for the treatment of angular cheilitis and why? |
- Miconazole - active against candida and S. aureus |