![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
82 Cards in this Set
- Front
- Back
|
Objectives |
|
|
|
Review: primary hemostasis, 2ndary hemostasis, and resolution |
|
|
|
review: 3 steps of platelet plug formation |
adhesion: platelets stick to injured endothelium
aggregation: platelets attract each other activation: procoagulatn stimulation of clotting cascade |
|
|
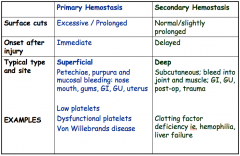
review : disorders in 1º vs. 2º hemostasis and how they present 1. pattern of bleeding 2. site 3. onset 4. example conditions |
|
|
|
Screening for bleeding disorder? 2 components |
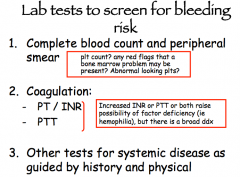
1. take the history 2. simple lab tests: CBC/diff, PBS, INR, PTT |
|
|
questions to ask in the bleeding history.. 8 |
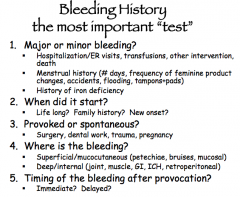
+ PMHx (liver, renal disease, CT disease) + Meds (ASA, anticoags, NSAIDS) + FMHx bleeding problems |
|
|
Lab tests to screen for bleeding risk |
|
|
|
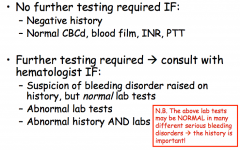
Note: when is no further testing required when is further testing required |
|
|
|
How is thrombocytopenia defined? |
<140x10^9 cells at the U of A NOT a diagnosis. IS a lab value that must be explained. |
|
|
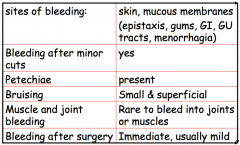
Thrombocytopenia: typical bleeding pattern |
|
|
|
note: threshold for minor spontaenous bleeds? threshold for life threatening bleed? wrt platelet counts |
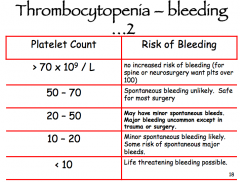
sx may not be evident until count drops below 30 or even 20 |
|
|
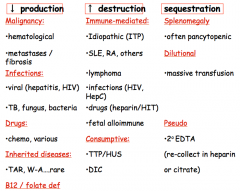
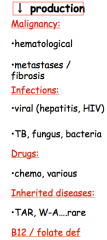
Can approach low platelets by pathologic category: dec. production, inc. destruction, sequestration |
|
|
|
dec. production: 5 to consider |
|
|
|
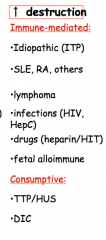
increased PLT destruction: immune mediated vs. consumptive |
|
|
|
PLT sequestration: 3 |

|
|
|
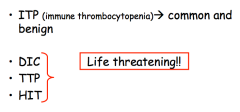
The 3 letter platelet conditions of thrombocytopenia. there are 4. 3 are emergencies.. |
|
|
|
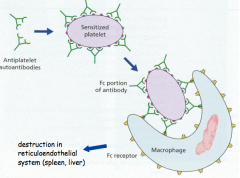
pathophys of ITP |
|
|
|
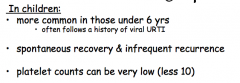
ITP in Kids: 1. age group 2. natural history 3. potential platelet counts |
|
|
|
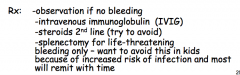
Rx of ITP in kids |
IVIG:flood system with ab’s, and it’s not as easy from immunesystem to attack platelets. Rituximab:wipes out b lymphs. This resets immune system andhopefully when it grows back, it is not autoimmune |
|
|
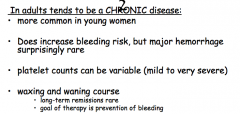
ITP IN ADULTS 1. M:F 2. bleeding risk 3. platelet counts 4. natural history |
|
|
|
ITP in adults: Tx |
|
|
|
ITP is a diagnosis of exclusion |
rule out the bad stuff... |
|
|
the 3 letter platelet emergencies.. 3 |
|
|
|
note: DIC is a syndrome 2ndary to severe systemic illness |
k |
|
|
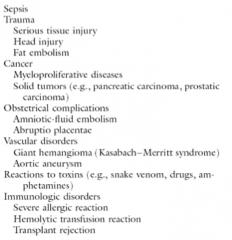
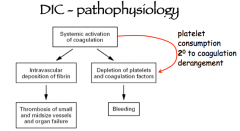
pathophys of DIC |
|
|
|
Clinical Features of DIC |
1. Low PLT count on CBC with occasional red cell fragments 2. bleeding! 3. thrombosis: digital infarcts, stroke/neuro/end organ damage 4. other labs: anemia, prolonged PT, PTT, depleted clotting factors 5. low fibrinogen |
|
|
lab findings in DIC 5 |
1. anemic 2. prolonged PT, PTT 3. depleted clotting factors 4. low fibrinogen 5. low platelet count |
|
|
Therapy of DIC? |
1. treat underlying disease 2. replace clotting factors (plasma) and fibrinogen (cryoprecipitate) if bleeding 3. low dose heparin if thrombosis dominates |
|
|
two types of MAHA (microangiopathic hemolytic anemia) |
TTP: thrombotic thrombocytopenic purpura HUS: hemolytic uremic syndrome |
|
|
TTP and HUS: clinnical features? 2 |
|
|
|
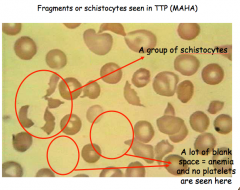
what is required to diagnose MAHA? 2 |
1. low platelets with hemolytic anemia 2. red cell fragmentation on blood film if you have these 2, the diagnosis is made |
|
|
Classical pentad of TTP? |
only need first 2 for dx 1. hemolytic anemia 2. red cell fragmentation ---- 3. Fever 4. renal failure 5. neuro symptoms THE ABSENCE OF FULL PENTAD DOES NOT MAKE TTP LESS LIKELY |
|
|
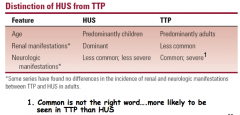
How to diff't HUS from TTP on basis of age neuro manifestations renal manifestations |
|
|
|
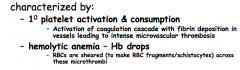
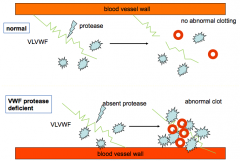
pathophys of TTP/HUS |
depletion of vWF cleaving metalloprotease (ADAMTS13) is responsible for the syndrome |
|
|
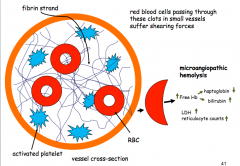
diagram: pathophys TTP/HUS |
|
|
|
mech of red cell shearing in MAHA |
|
|
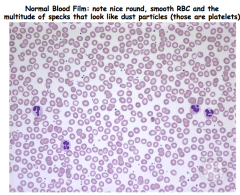
normal vs. TTP blood film |
|
|
|
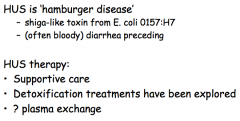
HUS; 1. etiology 2. prodrome.. 3. Rx |
|
|
Causes of TTP |
d |
|
|
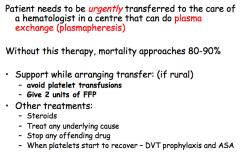
TTP: 1. definitive care 2. supportive care to do while arranging transfer? 3. Other Treatments |
|
|
|
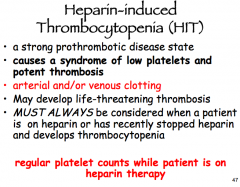
HIT: 1. clinical syndrome? 2. manifestations 3. when to consider 4. how to monitor... |
|
|
|
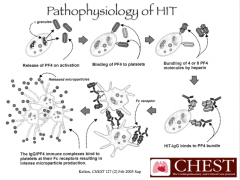
HIT pathophysiology |
|
|
|
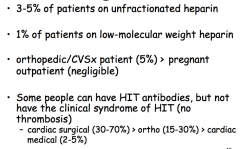
Who gets HIT/HIT antibodies? 4 |
|
|
|
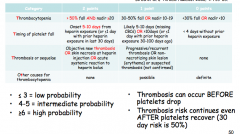
4T score gives a pretest probability for HIT. DNM |
|
|
|
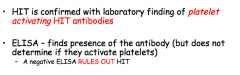
Diagnosis of HIT? what rules in HIT? what rules out? |
|
|
|
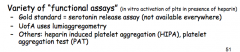
functional assays in HIT .. |
|
|
|
Rx HIT: |
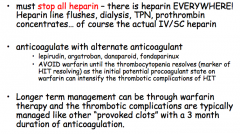
1. stop heparin 2. anticoagulate with alternate drug |
|
|
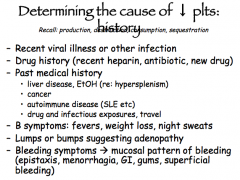
Hx to take in thrombocytopenia |
|
|
|
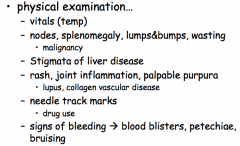
PE in thrombocytopenia |
|
|
|
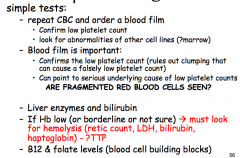
investigations in thrombocytopenia |
|
|
|
LOW PLT: what do we do if HB is low? |
MUST LOOK FOR HEMOLYSIS: (retic count, LDH, Bilirubin, Haptoglobin) consider TTP... |
|
|
Investigation of low PLT.. coag tests? HIT suspected? Serologic tests? |
|
|
|
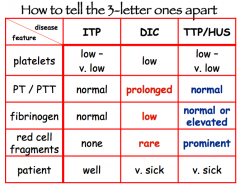
features that separate ITP, DIC, and TTP/HUS 1. PLT levels 2. PT/PTT 3. Fibrinogen 4. red cell fragments 5. patient Gen. appearance... |
|
|
|
Objectives: VTE |
|
|
|
why does the Superficial femoral vein have the stupidest name in the world |
because it is actually a DEEP vein |
|
|
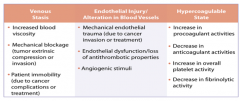
review: virchow's triad |
1. stasis 2. vessel wall injury 3. hypercoagulability |
|
|
example causes of venous stasis 5 |
|
|
|
example causes of hypercoagulability 6 |
|
|
|
causes of vascular injury |
|
|
|
VTE risk factors explain importance of additive risk factors, and age |
|
|
|
VTE: importance of provoked vs. unprovoked |
|
|
|
where do blood clots form? note: weird clot sites may require workup.. |
|
|
|
relationship between DVT and PE... |
|
|
|
Dx of VTE: clinical findings are neither sensitive nor specific .. |
|
|
|
Sx DVT/PE |
|
|
|
|
|
|
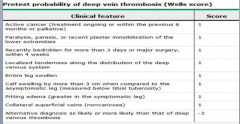
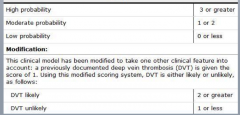
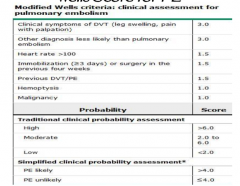
Modified wells 7 |
|
|
|
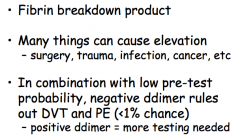
review: D dimer is sensitive but not specific for VTE |
|
|
|
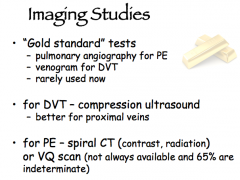
Imaging studies in VTE |
|
|
|
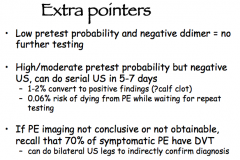
Extra imaging pointers |
|
|
|
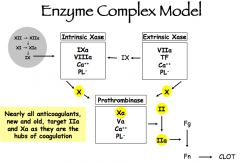
Clotting cascade review |
|
|
|
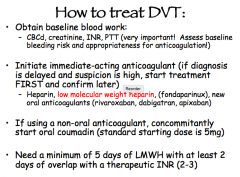
How to treat DVT? (drug, dosages, etc) |
|
|
|
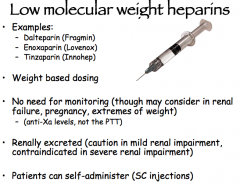
LMWH: |
|
|
|
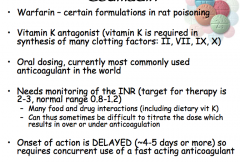
Coumadin: dosing, monitoring, target INR, timing of onset |
|
|
|
Note: INR reflects the dose of coumadin given ___ hr earlier |
48 hours |
|
|
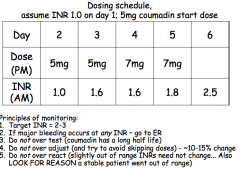
example coumadin dosing schedule |
|
|
|
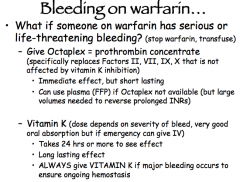
how to manage bleeding on warfarin? |
|
|
|
minimum duration of anticoagulation? |
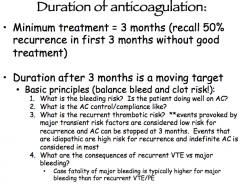
|
|
|
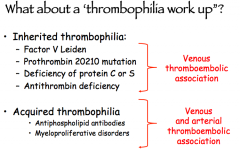
thrombophilia workup// |
|
|
|
note: hypercoagulable workup should NOT be routinely ordered on all patients with clot |
d |
|
|
mechanisms of increased clot risk in cancer |
|
|
|
VTE treatment in cancer... |
|