Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
25 Cards in this Set
- Front
- Back
|
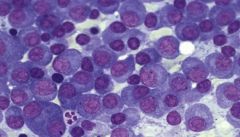
- multiple myeloma
- Lots and lots of plasma cells – hard to find normal precursors (not many neutrophils, or RBCs, why anemic) |
a
|
|
|
- Monoclonal lambda staining pattern associated with multiple myeloma in BM
- in situ hybridization |

a
|
|
|
- Monoclonal lambda staining pattern associated with multiple myeloma in BM
- in situ hybridization |
a
|
|
|
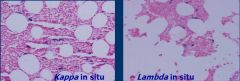
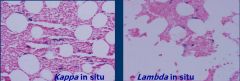
- Both the kappa and lambda in situ hybridization in BM studies show positive staining (blue cells)
- This is indicative of a polyclonal staining pattern |
a
|
|
|
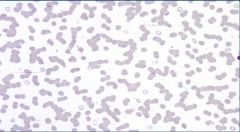
Rouleaux common in hyperviscoscity syndrome
|
a
|
|
|
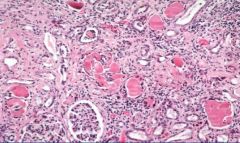
- Light chain cast nephropathy - (Myeloma kidney)
- Way too much space b/t tubules and glomeruli b/c you have so many plasma cells – not the actualy problem, its b/c Ig is despositing in the tubules - giant cells often seen |
a
|
|
|
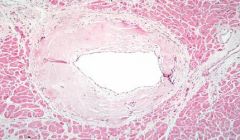
- HandE stain of heart
- amyloid fibrosis |
a
|
|
|
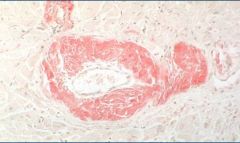
- AF
- congo red stain |
a
|
|
|
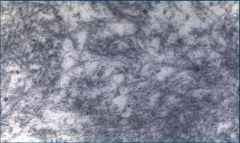
- AF
- EM of fibrils |
a
|
|
|
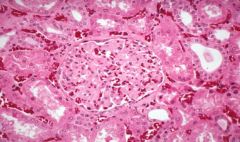
Amyloidosis Involving glomerulus
|
a
|
|
|
Amyloidosis - Liver
|

a
|
|
|
Amyloidosis-Heart
|

a
|
|
|
- Marrow is hypercellular. Waldenström's Macroglobulinemia - No fat is seen. Higher power view shows a mix of plasma cells and lymphocytes.
|

a
|
|
|
- Marrow is hypercellular. Waldenström's Macroglobulinemia - No fat is seen. Higher power view shows a mix of plasma cells and lymphocytes.
|

a
|
|
|
Multiple myeloma - pathophys
|
- clonal, neoplastic prolif of plasma cells – mainly in BM - they live longer than they should so accumulation
- path happens after class switch - need IL-6 to antagonize apop |
|
|
Multiple myeloma - genetics
|
- aneuploid in up to 80%
- Hyperdiploidy most common - abnormal karyotype in 50% - chrom 1 and 13 have poor prognosis) - 14 (heavy chain gene) - cyclin D1 -> cell division - c-myc -> gene rearrange - inc Bcl-2 - if p53 mutant, chemo resistant |
|
|
Multiple myeloma - Epi and Sx
|
- disease of old (avg 65)
- Weight loss or other B sxs (but much less pronounced) - Sxs of anemia, and bone pain - blacks twice as likely |
|
|
Multiple myeloma - Lab stuff
|
- Rouleaux on the blood smears -> lots of circulating IG
- protein/albumin discordance - Hypercalcemia from bone degradation - Creatinine due to renal failure - SPEP – lets us know if there’s a monoclonal protein (G id 60%, A is 20%) |
|
|
Amyloidosis
|
- AL associated with MMy and abnormal light chains
- will stain + with Congo red stain by light microscopy (peach color) - kidney and heart most likely to be involved - dx w/ congo red, SC fat asp, renal or rectal biopsy - treat like MP - can do transplant |
|
|
Waldenström's Macroglobulinemia
|
- Disease of older adults
- low grade lymphoma involving BM and spleen - Lymphoplasmacytic, mature B-cell, w/ monoclonal IgM - sx are cold agglut, blurred vision and hypervis, can have amyloidosis - Dx - BM, spleen showing IgM - treat w/ plasmapherisis to remove IgM - can do chemo w/ alks and steriods, analougs, or rituximab |
|
|
Multiple Myeloma - major criteria
|
1) Plasmacytoma on tissue biopsy
2) BM plasmacytosis >30% 3) Monoclonal serum protein |
|
|
Multiple Myeloma - minor criteria
|
- BM plasmacytosis 10-30% w/ a smaller monoclonal spike
- Lytic bony lesions - Depressed normal Igs |
|
|
Multiple Myeloma - treatment
|
- chemo immediately
- Melphan + prednisone (MP) - VAD via IV if advanced - Thalidomid if refractory - can combine w/ Dexamthasone - Autologous stem cell transplant in younger - Bortezomib (VELCADE) – proteosome inhibitors - modulate w/ IFN-a - maintain w/ steriods |
|
|
Multiple Myeloma - adjuvant care
|
- Bisphosphonates - Pamidronate and Zoledronate - decrease Ca2+, prevent pathologic fractures –
- EPO - G-CSFs raises neutrophils, may prevent infections and prophylactic may decrease infections too - both controversial |
|
|
Monoclonal Gammopathy
|
- precursor for MMy - 1/4 progress
- serum M protein < 3 g/dL; < 5% marrow plasma cells - no urine M, lytic lesions, anemia, hypercalcemia, or renal failure - protein/albumin is normal!! ~2 |