![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back
|
indications for caesarean in twin delivery |
obstetric causes
foetal causes
|
|
|
indication of the urgent delivery of 2nd baby |
|
|
|
delivery of 2nd baby in a twn |
longitudinal lie
Transverse lie
|
|
|
occipito posterior VE findings |
sagital suture ant fontanelle is in anterioly |
|
|
breech VE findings |
complete breech
frank breech
|
|
|
face presentation VE findings |
mouth hard alviolar margins alviolar margins absence of meconium |
|
|
brow presentation VE findings |
supra orbital ridges and ant fontanelle |
|
|
indications for electronic fetal monitering (continuous) |
|
|
|
contraindications for dinoprostone induction |
|
|
|
Shoulder dystocia |
|
|
|
chorioamnionitis |
3 out of 6
|
|
|
atonic PPH |
|
|
|
delayed 3rd stage of labour |
placenta not delivered within 30 min
|
|
|
secondary PPH |
|
|
|
Cord prolapse |
|
|
|
Obstetric coholestasis |
|
|
|
mx obstetric choleostatis |
|
|
|
HELLP syndrome |
|
|
|
Breech delivary |
|
|
|
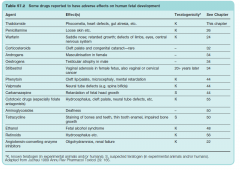
teratogens |
|
|
|
live and liver related enzymes in preganancy |
|
|
|
in preganacy causes of ALT AST elevation |
--------- 5. dengue marked elevation in 6. acute viral hepatitis 7. hypoxic hepatic injury 8. hepato toxic drugs |
|
|
serum bilirunin rise in preganacy |
mild elevartion
Marked elevation 5. Obstetic cholestatis 6. later stage of AFLP |