Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
27 Cards in this Set
- Front
- Back
|
The diagnosis and classification (and ultimately management) of hematopoietic neoplasms is dependent on: (5)
Which is most important? |
Clinical manifestations
Morphology of biopsied tissue Special stains (immunohistochemistry/cytochemistry) Flow cytometry Molecular studies* Cytogenetics* Clinical manifestations |
|
|
Pattern of gene _____ vary as cells mature and differentiate.
Can these help classify disease? How about disease progression? Point/type of origin? |
expression
yes Yes. Yes. |
|
|
CD =
All normal leukocytes display CD___ to varying degrees. |
cluster of differentiation
CD45 |
|
|
Flow cytometry is trying to line up cells.....
What is being measured? |
...single file.
emissions post-laser excitation. |
|
|
What is immunophenotyping?
What does FACS stand for? |
identifying the pheynotype using fluorescently labeled antibodies (probe) in Flow cytometry.
FACS = fluorescence activated cell sorting |
|
|
Low numbers correspond to ____-cell phenotypes?
Midteens? Nineteen & Early twenties? (Army help to remember) CD34? CD33? |
T-cells
Myelomonocytic B-cell stem cell, myeloid |
|
|
CD4 = ?
CD13 = ? CD14 = ? CD15 = ? |
T-cells
13 = granulocyte 14 = monocytic 15 = granulocyte |
|
|
Leukemias are Dx according to...
What are the two major categories? |
...the prominent cell type involved.
Acute Chronic |
|
|
Characterize the two major categories of leukemias.
|
Acute: rapid onset, aggressive, usually poorly differentiated (blasts)
Chronic: insidious onset, usually less aggressive and more mature appearing |
|
|
Can chronic leukemias transform into something worse?
|
Yes, they can.
|
|
|
ALL is most common in adults or children?
|
Children.
|
|
|
Philadelphia chromosome shows up more frequently in children or adults?
Where does it have the worse prognosis? |
adults.
adults. |
|
|
FACS stands for...
|
...fluorescence activated cell sorting.
|
|
|
What are the two types of ALL?
Which has a better prognosis? |
B-ALL, T-ALL
B-ALL, though it is better for children than adults. |
|
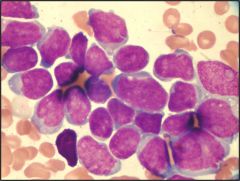
What class of leukemia (acute or chronic) is seen here? What type of cells evidence this?
|
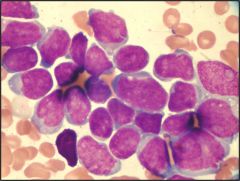
Acute leukemia. These are blasts in the peripheral blood.
|
|
|
In the context of ALL prognosis, list the following as favorable, intermediate, or unfavorable:
hyperdiploid hypodiploid t(1,19) t(9,22) t(12,21) abn(11q23) Why does this make sense, given which age range has the better overall prog? |
Favorable: hyper, t(12, 21)
Inter: t(1,19) Bad: t(9.22), hypo, abn(11q23) Kids have the better prog, and they also are more likely to have these favorable characteristics. |
|
|
What is the name of the product of the t(12,21) translocation?
|
TEL-AML1
|
|
|
On the FAB subtypes, the only one we need to know is Promyelocytic = APL, a type of AML... what is the M#?
Which translocation is associated with APL? What percent evidence this? What do the others show? |
M3
t(15,17) 95% RARa rearrangement with other genes. |
|
|
What could help us differentiate b/t a BM biopsy of AML and that of ALL?
|
The AML one might have an abundance of pink cytoplasm (it's a disease of myeloid lineage, after all)
this isn't necessarily the case tho', so be careful. |
|
|
How does ATRA work?
|
Overcomes the avidity of RARa binding to the corepressor complex... since this is what's blocking differentiation, ATRA administration allows differentiation to occur again.
|
|
|
50% of AMLs have _____ clonal cytogenetic abnormality.
Are they devoid of genetic mutations? What is the most frequent molecular abnormality in AML? Is it associated with good or bad prog? |
No.
No, their mutations are just at the genetic lvl, rather than the cytogenetic lvl. FLT3 Bad. |
|
|
Differentiate between Benign Neutrophilia and CML based on the: a) peripheral smear and b) lab values
|
Left shift isn't as marked in BN as it is in CML.
BN = normal or increased LAP CML = Decreased LAP |
|
|
What is LAP?
|
Leukocyte Alkaline Phosphatase
only important re: telling Benign neutropenia apart from CML. |
|
|
What is the most common length of the BCR-ABL transcript produced in CML?
|
p210
|
|
|
+ Coombs
ITP AIHA white pulp in the spleen recurrant URI/LRI - all are associated with which leukemia? |
CLL, a mature B-cell lymphoma/leukemia.
|
|
|
Cells expressing CD23, CD5, and exhibiting light-chain restriction suggest which type of diz?
Deletion of 13q14 is found in >50% of cases.... is it a a good or bad prognostic marker? |
CLL / SLL
Good. |
|
|
Which diz can BCR-ABL drive independently? Which other diz is it associated with in which it is just a bad prognostic marker?
|
CML
ALL |