![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
104 Cards in this Set
- Front
- Back
|
Phenomology |
The study of someones lived experience |
|
|
Disease |
State of ill heath |
|
|
Illness |
subjective experience of loss of health |
|
|
Health |
an objective process of functional stability, balance & integrity |
|
|
Wellness |
the subjective experience |
|
|
3 Classifications of Health |
1. Health as Stability 2. Health as Actualization 3. Health as Stability & Actualization |
|
|
3 Historical Approaches to Health |
Medical, Behavioural, Socioenviromental |
|
|
Prereqs for Health (WHO 1986) (9) |
Peace, Shelter, Education, Food, Income, Stable Ecosystem, Sustainable Resources, Social Justice, Equality |
|
|
Empowerment |
a person's ability to define, analyze & solve problems |
|
|
What were added to the prereqs for health in the Jakarta Declaration 1997 |
Empowerment of women, social security, respect for human rights, social relations. Declared poverty to be the greatest threat to health |
|
|
What does working 'downstream' mean? |
Assisting people experiencing the negative health effects |
|
|
What does working 'upstream' mean? |
Working with people before problems come up. What could have been done? |
|
|
Health Disarities Task Group Said: |
Socioeconomic status, aboringinal identity, gender & geographic location most important factors related to health disparities |
|
|
Major Determinant of Health (12) |
1. Income and Status 2. Social Support Networks 3. Education and Literacy 4. Employment and Working conditions 5. Physical Environment 6. Biological and Genetic Endowment 7. Individual Health Practices and Coping Skills 8. Healthy Child Development 9. Health Services 10. Gender 11. Culture 12. Social Environments |
|
|
What are the three levels of disease prevention? |
Primary prevention (against disease), Secondary prevention (early detection) , tertiary prevention (minimizing disability from disease, maximizing productivity with limitations) |
|
|
5 Health Promotion Strategies |
1. Build Healthy Public Policy 2. Create Supportive Enviroments 3. Strengthen Community Action 4. Develop Personal Skills 5. Reorient Health Services |
|
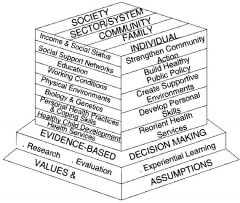
What is this? |
It s the population health promotion model. Who: with whom can we act (society), What: on what can we take action (health-areas), How: How can we take action to improve health (Ottawa Charter Action Strategies), Why: Why take action? (use before available information) |
|

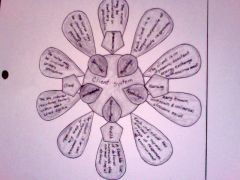
what does this diagram mean? |
PHC model focuses on collaboration among health professionals, community members, and others working intersectorally , emphasizing health promotion, development of health policies, and prevention of disease for all. |
|
|
population
|
collection of individuals who have in common one or more personal or environmental characteristic. |
|
|
community
|
a group of people that share a geographic dimension and a social dimension.
|
|
|
primary health care |
focuses on education, rehab, support services, health promotion, disease prevention
|
|
|
public health |
safeguards & improves the health of populations in the community
|
|
|
Social Justice |
Rooted in the notions of social responsibility and fairness |
|
|
What is the 'Chain of Infection'? At each stage give an example of a way to break the chain. |
Infectious Agent (Diagnosis/Teatment)->Source (Education/policy, Enviromental Sanitation, Disinfection)->Exit (Handwashing, Control of Excretion & Secretions)->Means of Transmission (Isolation, Food Handling, Enviromental Sanitation, Disinfection, Handwashing)->Portal of Entry (First Aid, Personal Hygiene, Handwashing)->Susceptible Host (Treatment of underlying Diseases, immunization) |
|
|
Categories of Vulnerable Populations |
Poor and Homeless People, People in Precarious Circumstances, People with Chronic Conditions and Disabilities, People who Engage in Stigmatizing Risk Behaviour |
|
|
Values of Community Health Nurse (6) |
Caring, Public Health Care, Multiple Ways of Knowing, Individual & Community, Partnership, Social Justice, Empowerment |
|
|
Different modes of Transmission (5 ways) |
Contract Transmission (Direct Contact, Indirect Contact), Droplet Transmission, Airborne Transmission, Vehicle Transmission, Vectorborne Transmission |
|
|
Stigma |
a mark of disgrace associated with a particular circumstance, quality, or person. |
|
|
Medical Approach to Health |
emphasized that medical intervention restores health. New technological and scientific medical advances facilitated medical approach. National health insurance was created... (illness care) |
|
|
Behavioural Approach to Health |
1974 Lalonde Report shifted from medical approach to behavioural approach. Four broad health determinants: lifestyle, environment, human bilogy and organization of health care. Lifestyle received the most attention. Improvements mades primarily by well-educated, well-employed, and higher income canadians. |
|
|
Socioenviromental Approach to Health |
Closely tied to social structures... emphasizes the social context of health and the relationship between personal health behaviours and social and physical environments. Emphasizes connectedness, self efficacy and capacity to engage in meaningful activities. |
|
|
Achieving Health for All (1986)
|
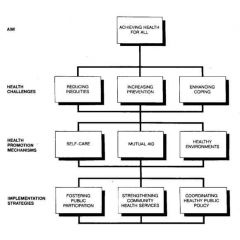
Canada's blueprint for achieving the WHO goal of 'health for All 2000'. Identified three major health challenges - reducing inequities, increasing prevention, and enhancing coping mechanisms.
|
|
|
3 Levels of Critical Thinking |
Basic - learner trusts experts Complex - analyze and examine choices more independantly Commitment - anticipate the need to make choices without assistance from other professionals |
|
|
Pathogens |
a microorganism such as a virus, bacterium, prion, fungus or protozoan, that causes disease in its host. |
|
|
Immunocompromised |
a person who's immune system's ability to fight infectious disease is compromised or entirely absent. |
|
|
Pathogenicity |
the potential capacity of a certain species of microbes or viruses to causes a disease. |
|
|
Normal Defence Mechanisms Against Infection |
Skins, sweat, lungs, etc |
|
|
Epidemiology
|
the science that studies the patterns, causes, and effects of health and disease conditions in defined populations |
|
|
Growth |
Quantitative, measurable, aspect of an individual's increase in physical measurements. Height, weight, teeth, skeletal structures, sexual characteristics. physical Growth is not only genetic but also affected by other contextual factors such as socioeconomical status. |
|
|
Development |
Progressive and continuous process of change, leading to increased skill and capacity to function. Result of complex interactions between biological and environmental influences. |
|
|
Mechanisms of Deveopment |
Explanatory components of each developmental theory or the means by which the developmental tasks are achieved. |
|
|
Box 21-1 Cultural Aspects of Care |
Each cultural background needs to be work with in nursing so that is is congruent with the patients beliefs and values. Aboriginal Cultures -> Circle of Life (in harmony with cycle of life of nature) |
|
|
Genetic Factors/Natural Factors |
Heredity (genetic endowment) , Temperament (psychological mood with which the child is born.. influences interactions between an individual and environment) |
|
|
Environmental Factors |
Family; Peer Group; Health Environment; Nutrition; Rest, Sleep, Exercise; Living Environment; Political and Policy Environment |
|
|
Interacting Factors |
Life Experiences; Prenatal Health; Sate of Health |
|
|
Organicism (tradition) |
a theoretical focus on the organism itself. Development is a result of biologically driven behaviour and the person's adaption to the environment |
|
|
Psychoanalytic and Phychosocial Tradition |
Development of personality, thinking, behaviour, and emotions. Thought to occur with varying degrees of influence from internal biological forces and external societal and cultural forces. |
|
|
Mechanistic Tradition |
Organism is similar to a machine. Development depends on the level of stimulation, kind of stimulation and the history of stimulation from the environment. Behaviour is seen as responsive to environmental forces rather than driven only by internal causes such as maturation. |
|
|
Contextualism (tradition) |
focus on the relationship between the individual and his or her social context. The individual and environment are viewed as mutually influential, acting on one another in dynamic interaction. |
|
|
Dialecticism (tradition) |
All developmental theories are considered mutually interactive. Keys element is to incorporate multiple contexts. |
|
|
Population Health Approach |
Keating & Hertzman's model which considers human development a population phenomenon. Strong association between the health of populations, developmental outcomes, and the social and economic forces affecting the larger society. |
|
|
Developmental Health |
the physical and mental health, well being, coping, and competence of human populations. |
|
|
Resilience (theory) |
The maintenance of positive adjustment under challenging life conditions. |
|
|
Critical Thinking |
a process and a set of skills. Use of logic and reasoning to make accurate clinical judgements and decisions. |
|
|
Evidence-informed knowledge |
knowledge based on research or clinical expertise. Makes you an informed critical thinker |
|
|
Clinical Decision-making process (The Nursing Process) |
Skills: Interpretation, Analysis, Inference, Explanation, Self-Regulation Dispositions or Habits: Truth Seeking, Open-mindedness, Analyticity, Systematicity, Self-confidence, Inquisitiveness, Maturity
|
|
|
basic critical thinking |
a learner trusts that experts have the right answers for every problem |
|
|
complex critical thinking |
begin to separate your thinking processes from those of authorities and to analyze and examine choices more independently. |
|
|
commitment (to critical thinking) |
anticipate the need to make choices without assistance from other professionals, then you assume responsibility and accountability for those choices. |
|
|
Five Components of critical thinking |
1. Specific Knowledge Base 2. Experience in Nursing 3. Critical Thinking Competencies 4. Attitudes for critical thinking 5. Standards for critical thinking a. intellectual standards b. professional standards |
|
|
Box 11-4: Decision making by Baccalaureate Nursing Students |
Students at all levels of program decribed five key kinds of decisions: Assessment, Intervention, Resource, Communication and Action. |
|
|
Family Nursing |
based on the assumption that every person, regardless of age, is a member of some type of family form and carrier family experiences that have profound influences on their lives and approach to health care. The goal is to help the family and its individual members achieve and maintain optimal health throughout and beyond the illness experience. |
|
|
family |
a set of relationships that each patient identifies as family or as a network of individuals who influence each other's lives, regardless of whether actual biological or legal ties exist. |
|
|
Family forms (8) |
Patterns of people considered by family members to be included in the family. (Traditional Nuclear, Extended, Step-Family, Blended Family, Lone-Parent Family, Married & Common Law Couples, Intergenerational, Same Sex couples) |
|
|
Blended Families |
Formed when both parents bring children from previous relationships into a new, joint living situation or when children from the current union and children from previous unions are living together. |
|
|
Married Persons/Common Law |
without children |
|
|
Same Sex Couples |
Same Sex couples with or without children |
|
|
Traditional Nuclear Family |
Consists of a mother and father and their children |
|
|
Step-Families |
Formed when at least one child in a household is from a previous relationship of one of the parents |
|
|
Lone Person Families |
Consists of one parent and one or more children. The lone-parent family is formed when one parent leaves the nuclear family because of death, divorce, or desertion or when a single person decides to have or adopt a child. |
|
|
Extended Families |
Includes the nuclear family and other relatives (perhaps grandparents, aunts, uncles, cousins) |
|
|
Intergenerational Families |
Grandparents taking care of Grandchild |
|
|
Hardiness |
internal strengths and durability of the family unit and is characterized by a sense of control over the outcome of life, perceiving change as beneficial and growth producing, and active rather than passive approaches to stressful events. |
|
|
Resiliency |
ability to cope with expected and unexpected stressors. roles changes, developmental milestones and crises. |
|
|
Family as Context |
focus either on the individual patient within the context of his or her family or on the family with the individual as context. |
|
|
Family as Client |
focus on entire family; its processes and relationships,. Family patterns and interactions among family members are the focus, rather than individual characteristics. |
|
|
Relational Inquiry |
an approach that asks nurses to expand their contextual knowledge of families, developing a more in-depth and comprehensive consideration of the historical, economic, political, social, environmental and geographical influences at play when families encounter illness or other difficulties related to life transitions. |
|
|
Calgary Family Assessment Model |
a relational, strengths-focused practice model that guides nurses in the completion of comprehensive family assessment. Focuses on three major categories of family life: structure, developmental and functional dimensions. |
|
|
Structural Assessment |
Assessment: Internal Structure (people who are included in family and relationships) External Structure: relationships family shares with peopel and institutions outside family unit Context: whole situation or backgroud relevant to the family
|
|
|
Developmental Assessment |
Assessing the development of the family. Can help nurses to promote health during expected family life-cycle transitions and experiences of illness. |
|
|
Functional Assessment |
focuses on how family members interact and behave toward each other |
|
|
Genogram (basic index) |
a sketch of the family structure and relevant information about family members. Square - Male Circle - Female Square or circle inside - Index person X inside - Death (give date) |
|
|
Ecomap |
sketch of family's relationship with persons and groups outside the family. Family members who share the household are depicted in the center of the ecomap and various important extended family members or larger systems are sketched in to show their relationship to the family. |
|
|
Commendation |
a conversational statement emphasizing family strengths and abilities. Could include: clear communication, adaptability, health boundaries, support and nurturing among family members, and the use of crisis for growth. |
|
|
Reciprocity |
Giving and Receiving |
|
|
Respite |
Having someone come in to give a break so that burnout is reduced. |
|
|
Attributes of Health Families |
able to integrate the need for stability with the need for growth and change. The family can be viewed as context, in which you focus on either the individual patient within the context of his or her family or on the family with the individual as context, or the family can be viewed as patient, in which you focus on family interactions. |
|
|
How is stress conceptualized? |
Physiological conceptualizations (SAM, Fight or Flight) and psychological conceptualizations (cognitive) |
|
|
Define Biological Systems involved in stress responses |
Focused Mental Activity, Dialated Pupils, Bronchiolar Dialation, Increased Respiratory Rate, Increased Heart Rate, Increased Cardiac Output, Increased Glucose, Increased Fatty Acids, Increased Arterial Blood Pressure, Increased blood flow to skeletal muscles. |
|
|
How can overwhelming stress or chronic stress affect health? |
1. serious or long-standing physical and mental health problems 2. choosing coping strategies that are unhealthy 3. Ignoring warning signs or illness 4. Neglecting to take prescribed medications or treatments |
|
|
Acute Stress Disorder |
limited to the month after experiencing, witnessing or being confronted with a traumatic event. A reaction of intense far, hopelessness, or horror. 1. Dissociative Symptoms 2. Reaccuring Symptoms (i.e.Flashbacks) 3. Marked avoidance of stimuli 4. hyperarousal 5. symptoms emerge between two days and four weeks after traumatic event |
|
|
Post-traumatic stress disorder |
symptoms persistent, and have endured for month than one month.Clusters are similar to those of acute stress disorder with less emphasis on dissociative symptoms. |
|
|
How do stress theories integrate into nursing theories? |
They can be implement to a individual, family or community. |
|
|
Stress Management Techniques for coping? |
Regular Exercise, Support Systems, Time Management, Guided Imagery and Visualization, Progressive Muscle Relaxation, Assertiveness Training, Journal Writing |
|
|
How can stress in the workplace affect health care providers? |
Burnout |
|
|
Sleep |
a universal, dynamic, highly organized, physiological, and behavioural state required by most living organisms to maintain health and well-being. |
|
|
Sleep Vs. Rest |
a |
|
|
Stages of sleep cycle |
Stage 1: Nonrapid Eye Movement (light level) Stage 2. Nonrapid Eye Movement (period of sound sleep) Stage 3: Nonrapid Eye Movement (initial period of deep sleep) Stage 4: Nonrapid Eye Movement (deepest period of sleep) Stage 5: Rapid Eye Movement (dreaming... usually beins about 90mins after sleep has begun) |
|
|
Sleep Disorders |
Insomnias, Sleep Apnea, Excessive Sleeping (Narcolepsy), Parasomnias (Sleep Walking, Terrors) |
|
|
Normal Sleep Requirements, Patterns |
NeoNates: about 16hours Infants (3 months): 12-14hrs Toddlers: 12 to 14hrs Preschoolers: 13hrs School-aged: 9-10hrs Adolescents: not enough Young Adults: 6-8.5hrs Middle Adults: Time begins to decline Older Adults: can be change in patterns |
|
|
Factors that affect sleep |
Drugs, Lifestyle, Usual sleep patterns, Emotional Stress, Environment, Exercise & Fatigue, Food and Caloric Intake |
|
|
Process of 'assessing' sleep patterns |
Ask Patients. Write good sleep at one end of stick, worst sleep at other and get them to mark. |
|
|
Betty Neuman's Systems Model |
|
|
|
How does Neuman's systems model promote optimal wellness through use of primary, secondary and tertiary prevention strategies? |
goal of primary to promote patient wellness by stress prevention and reduction of stress factors. Secondary occurs after symptoms appear. Tertiary prevention begins when the patients becoming more stable and recovering. |