![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
310 Cards in this Set
- Front
- Back
|
World Health Organization definition of Community |
Groupof people often living in a confined geo area who may share a common culture,value or norms, and are arranged in a social structure according torelationships that the community has developed over a period of time. Membersget social and culture identity by beliefs of community. |
|
|
Most common definition of community |
Community of place or geographic boundaries. A cluster of people that share at least one common characteristic (i.e. geographic location, ethnicity) |
|
|
What is community health? |
The meeting of collective needs byidentifying problems and managing interactions within the community itself andbetween the community and the larger society. |
|
|
What are components of a healthy community? |
-Low crime rate -Quality schools Strong family life -Robust economy, with plenty of jobs available -High environmental quality (clean air,water) -Accessible and quality health services -Civic involvementGood transportation -Wide variety of leisure activities |
|
|
Aims of Healthy People 2020 |
1. Attain high-quality, longer lives free ofpreventable disease, disability, injury, and premature death2. Achieve health equity, eliminatedisparities, and improve the health of all groups3. Create social and physical environmentsthat promote good health for all4. Promote quality of life, healthydevelopment, and healthy behaviors across all life stages |
|
|
What is a community health assessment? |
Act of becoming acquainted with a community |
|
|
Goal of community healthy assessment |
To describe the needs of the community, and develop strategies to address the needs of the community Obtain health status, needs, and resources; identify where better information is needed |
|
|
Why are community health assessments performed? |
Required by community health law for every county every 3-4 years Under ACA, non-profit hospitals required to do an assessment every 3 years |
|
|
What is the principal challenge for nurses performing CHAs? |
Gaining entry and acceptance into a community |
|
|
What is subjective v. objective data at the community level? |
Subjective: windshield/observation Objective: statistics and numbers |
|
|
What are aspects of community core? |
History, demographics, ethnicity, values and beliefs |
|
|
Community subsystems |
Physical environment, education, safety and transportation, politic & government, health & social services, communication, economics, recreation |
|
|
Subjective examples of community core assessments |
Whatdo you see that illustrates thearea’shistory?Whatsorts of people do you see? Doyou see people that may be affected byyour project’s topic?Arethere churches, temples, mosquesorother religious adornments?Doesthe population lookhomogeneous? |
|
|
Objective examples of community core assessments |
Dataregarding…HouseholdTypesMaritalStatusReligiousdenominationsVitalStatistics (birth rates, morbidity & mortality rates, perinatal mortalityrates…) |
|
|
Subjective examples of physical environment assessments |
Howdoes the community look? Whatdoes the landscape look like? What doyou note about airquality,flora,housing, zoning,space, green areas,animals, people, humanmade structures,naturalbeauty,water, climate?Arethe houses old? What conditionare they in? What about sidewalks? |
|
|
Objective examples of physical environment assessments |
Dataregarding…Mapof the areaSizeand location within the regionWastedisposalWatersupplyTypeof housingAveragetemperatureAveragerain/snowfallPollution |
|
|
Subjective examples of education assessments |
Arethere schools in the area? Howdo they look?Whatis the reputation of theschools?Isthere a school health service? Howdoes that look?Whatare the major education issues? |
|
|
Objective examples of education assessments |
Dataregarding…GraduationratesDropout ratesLevelof educationNumberand types of schools includinghigher educationExtracurricularactivities |
|
|
Subjective examples of safety and transportation assessments |
Doyou see buses, taxis, bicycles?Arethere sidewalks, bike trails?Isgetting around the area possible forpeople with disabilities?Whatare the roads like?Dopeople feel safe?Doyou see protective service personnelaround (i.e., police, fire, EMS)? |
|
|
Objective examples of safety and transportation assessments |
Dataregarding…Useof transportationCommutetimesTypesof crimes committedCrimeratesWatersource and treatmentAirquality monitoring |
|
|
Subjective examples of politics and government assessments |
Arethere signs of political activity?Whatparty affiliation predominates?Doyou see evidence of people protesting?Whatdo the billboards tell you intermsof politics and gov’t?Arethere flags flying? |
|
|
Objective examples of politics and government assessments |
Dataregarding…Politicalparties (who predominates and how are they split?)Toppolitical issuesGovernmentaljurisdiction of the community (i.e., elected mayor, city council with singlemember districts) |
|
|
Subjective assessments of health and social services |
Whathealth care servicesarevisible?Arethese services overusedand/orbusy?Whatdo the emergency departmentslook like?Evidenceof acute or chronicconditions? |
|
|
Objective assessments of health and social services |
Statsregarding your project’s health-related topic…Statsabout who is affected by your project’s topic:Whois affected?Whatare those stats?Hospitalsand other health care services |
|
|
Types of communication to consider in community health assessments |
Formalcommunication-->newspapers, radio, TV, mail delivery, cable TV Informalcommunication-->bulletin boards, posters, billboards, newsletters |
|
|
Subjective examples of communication assessments |
Arethere “common areas” where peoplegather?Whatnewspapers do you see in the stands?Doyou see billboards, posters, etc. around? What do they display in termsof your topic? |
|
|
Objective examples of communication assessments |
Dataregarding…Numberand types of communication availableHowdoes the area communicate the types of resources available? |
|
|
Subjective assessments of economics |
Is ita “thriving” or “seedy” community?Whoare the major employers?Wheredo people shop?Arethere signs that foodstampsare accepted/used? |
|
|
Objective assessments of economics |
Dataregarding…UnemploymentratesIncome# ofhouseholds below the federal poverty levelOccupations |
|
|
Subjective assessments of recreation |
Wheredo children play?Whatare the major forms of recreation? Are they costly? Are theywell maintained?Whatrecreational facilities do you see?Arethere natural resources for recreation(trails, etc.) |
|
|
Objective assessments of recreation |
Dataregarding…Drugand alcohol useNumberand types of recreational facilities availableFundingOrganizationof recreational activities |
|
|
Four parts of a community diagnosis |
1. Diagnosis 2. Among [inserted affected group and location] 3. Related to [insert etiology] 4. As manifested by [inserted s/s] |
|
|
Aspects of objectives |
SMART: Specific, measurable, attainable, relevant (to the dx), time bound |
|
|
What is definition of disability? |
Inability to perform one or more of following: talking, walking, hearing, seeing, climbing stairs, lifting, performing ADLs,, doing school work, working at a job; or requiring assistive devices, or needing others to accomplish these tasks |
|
|
What is the 3rd largest minority in the United States? |
3rd largest minority |
|
|
How does prevalence of disability change with age? |
Increases; 50% for persons age 75+ |
|
|
Categories of disability with examples |
1. Developmental: from birth or early age (spina bifida, Down's, muscular dystrophy, cerebral palsy) 2. Acquired: at any age (TBI, spinal cord injury, progressive--COPD, arthritis, diabetic retionpathy, MS) 3. Age-associated: osteoarthritis, osteoporosis, and hearing loss |
|
|
What defines a chronic illness? |
3 months or more, without cure, long-lasting effects |
|
|
Causes of chronic illnesses |
-Genetics: asthma, cancer, cardiacdisease, dementia - Injury: paraplegia, blindness,mesothelioma -Behavior: lung cancer, COPD, diabetes,cardiac disease |
|
|
Prevalence of chronic disease |
50% of adults have one or more. 25% have two or more chronic health conditions. |
|
|
Predictions about chronic disease |
Was predicted by 2050, 50% would have more than one chronic illness--> however, we are already there in 2016 |
|
|
Implications of chronic disease |
Increased health care cost (4/5 healthcare dollars, 84% healthcare spending) |
|
|
Characteristics of chronic illness |
Phases of disease (remissions, relapses), psychological impact, social impact, financial impact, therapeutic regimen (may be time-consuming, costly, or have side-effects), individual responsibility, Domino effect (one or more chronic illness leads to another), collaboration, uncertainty |
|
|
What comprises the trajectory model of chronic illness? |
Medical model + nursing wellness and self care models = trajectory model of chronic illness |
|
|
Trajectory Model Phases |
1. Pretrajectory 2. Trajectory 3. Stable 4. Unstable 5. Acute 6. Crisis 7. Comeback 8. Downward 9. Dying |
|
|
Steps in nursing process |
Assessent, nursing dx, goals, interventions, evaluation |
|
|
What is involved in pre-trajectory phase? |
No chronic illness yet (no s/s), but they are headed there based on risk factors (stress, lifestyle, genetics) Ex. Pre-diabetic with elevated hemoglobin A1C |
|
|
The pretrajectory phase is all about what level of prevention? |
Secondary prevention |
|
|
Nursing process within the pre-trajectory phase |
1. Testing 2. Counseling 3. Education |
|
|
What is the trajectory phase? |
Individual develops s/s of chronic illness; receives workup and is diagnosed with chronic illness |
|
|
Nursing process within the trajectory phase |
1. Explanation/educate 2. Emotional support |
|
|
What is the stable phase of the trajectory model? |
S/s of chronic illness under control because of medicine, behavioral changes, etc. Illness management usually takes place in the home |
|
|
Nursing process of the stable phase of the trajectory model |
1. Positive behaviors 2. Health promotion 3. Health promoting behaviors |
|
|
What is the unstable phase of the trajectory model? |
Ptexperiences a setback when the CI exacerbates; inability to keep sympmtoms undercontrol,difficulty carrying ADLS, may require diagnostic testing and changes inmedication/treatmentUsuallystill an outpatient process, but more cocntact with healthcare providers |
|
|
Nursing process in the unstable phase of the trajectory model |
Guidance and support Education |
|
|
What is the acute phase of the trajectory model? |
Sudden, severe onset of symptoms ,individual likely to be in hospital, ADLs disrupted (like unstable stage but worse). Caregiver role strain in this stage |
|
|
Nursing process of acute phase in trajectory model |
1. Direct care 2. Support |
|
|
What is the crisis phase of the trajectory model? |
A critical, life-threatening event has occurred, requiring immediate and emergent treatment. ADLs completely suspended. Family also in crisis mode. |
|
|
Nursing process in the crisis phase |
1. Direct phase 2. Collaboration with healthcare team 3. Stabilize |
|
|
What is the comeback phase of the trajectory model? |
Gradual recover from crisis or acute phase. May have new or worsened disability. Pt may need rehabilitation. Caregiver role strain may persist. |
|
|
Nursing process for comeback phase of the trajectory model |
1. Coordination of care 2. Adaptation |
|
|
What is the downward phase of the trajectory model? |
Sadphase, rapid or generally worsening of illness, physical decline, and increasein disability. ADL decline depends on each decrease in ability. PT can lingerin this stage for a long time. If death is imminent, hospice may be utilized.Familygrieving and reminiscing common. |
|
|
What is the nursing process in the downward phase of the trajectory model? |
1. Home care 2. New treatment plan 3. End of life planning |
|
|
What is the dying phase of the trajectory model? |
Death is imminent--weeks or days. Gradual loss of function, loss of ADLs. Family grieving. |
|
|
Nursing process in the dying phase of the trajectory model |
Direct care, comfort, support |
|
|
Factors affecting nutrition |
Insufficient intake of nutrients, altered ability to use ingested nutrients, increased metabolic demand |
|
|
Nursing interventions for altered nutrition |
¨Assessfor signs & symptoms of malnutrition¨Monitororal intake/calorie count¨Dietaryconsult¨Speechconsult: Swallowing evaluation¨Small,frequent meals¨Encouragesignificant other to bring in favorite foods and be present during meals¨Manageenteral and parenteral nutrition |
|
|
Enteral v. parenteral nutrition |
Enteral nutrition: food is directly put in stomach Parenteral: food is supplied into viens of Pt |
|
|
Diets in the hospital setting |
NPO, clear liquid no residue--apple juice, broth, tea; full liquid--ice cream, creamed soup, pudding; thickened liquid--prevent choking/aspiration, soft or pureed--easier to chew, restrictive diets (NAS, Cardiac, Renal), nutritional supplements (Ensure, Boost), Enteral feedings (osmolite, Jevity), parenteral feeding (PPN, TPN) |
|
|
Definition of GI intubation |
Refersto insertion ofrubber or plastic tube that goes directly into intestine or stomach: may beplaced via mouth, nose, or directly into stomach |
|
|
Why is GI intubation used? |
-Decompression: remove gas and fluid buildup (most common)—may be for obstruction, GIbleeding, to prevent N/V post-op--needs to be attached to wall suction (low) -Aspiration: removal of substance by suction, or to obtain substance fortesting - Lavage: wash out or cleanse the stomach with water or other substances - Administer: medications or feedings (no larger than 12 French) - Diagnose: disorders of the GI tract (mobility disorders) |
|
|
Types of gastric tubes |
Orogastric, nasogastric--> both sit in stomach |
|
|
When are orogastric tubes most commonly used? |
ER, ICU to quickly decompress the stomach |
|
|
What is a Levin tube? |
SIngle-lumen nasogastric tube |
|
|
What is gastric or salem pump? |
NG tube, double lumen: relatively stiff (can be irritating) but is very commonly used. Blue sump port to allow atmospheric air to enter stomach to prevent adherence of the tube to the gastric mucosa. Can be used for decompression, feeding, med adminisration |
|
|
What is Dobhoff tube? |
Soft NG tube, smaller French size, pump friendly |
|
|
Types of enteric tubes |
Nasoduodenal tubes, nasojejunal tubes--> sit in intestines |
|
|
When are enteric tubes used? |
Tubes are rare, but used when the stomach needs to be bypassed temporarily (4-6 weeks) |
|
|
Long-term options for nutrient supply |
Gastrostomy, jejunostomy, percutaneous endoscopic gastrotomy (PEG), percutaneous endoscopic jejunostomy (PEJ) |
|
|
How are gastrostomy and jejunostomy created? |
Created via intrabdominal surgery--> stomach wall is brought to surface to create a stoma (jejunostomy may be elected if stomach needs to be bypassed); balloon on tubes anchor the tube in place within the stoma |
|
|
How are percutaneous endoscopic gastrotomy (PEG) and percutaneous endoscopic jejunostomy (PEJ)? |
Connection is made through wall via endoscopic approach (feeding button) |
|
|
Why is tube removal with PEG or PEJ an emergency? |
Hole can close within 4 hours |
|
|
Indications for parenteral nutrition |
Nutrients via IV when GI system is not working, indicated for inability to ingest fluids or foods for 7 days |
|
|
Typically formulas for parenteral nutrition |
1-3 L fluid over 24 hours-- can include fat emulsions that can be infused simultaneously |
|
|
How long can peripheral parenteral nutrition be used? What must be done after this? |
TPN can be run peripherally for 5-7 days, longer than this typically requires central line or PICC |
|
|
Potential complications of central lines |
Infection, pneumothorax, clotted or displaced catheter, hyperglycemia, rebound hypoglycemia |
|
|
Parenteral nutrition nursing process |
1.Useinfusion pump2.Donot change rate rapidly3.Monitorblood glucose levels (q4 hours) 4.Inabsence of PN, use D105.Catheterand site care6.Monitorelectrolyte levels 7. Monitor indicators of fluid balance (strict I+O, weigh patient daily, S/s of dehydration or fluid overload), 8. patient teaching and support |
|
|
Nursing management for nasogastric (NG) tubes |
¨Preppatient¨Inserttube ¨ConfirmPlacement¨Cleartube obstruction¨Monitorpatient¨Provideoral and nasal hygiene¨Monitorand manage complications¨Removethe tubei |
|
|
What is involved in prepping patient for NG tube? |
Purpose, procedure |
|
|
Steps in NG tube insertion |
1. Confirm provider's order and identify patient 2. Measure (distance from nostril to tip of earlobe, distance from earlobe to tip of xiphoid process, then add 6-10 cm) 3. Upright with protective barrier 4. Numb nares (inhale lidocaine) 5. Lubricate (water-soluble) 6. Tilt head up then head down (insert into nasopharynx until feel resistance, then have patient lower head down and instruct pt to swallow) 7. Swallow 8. Inspect 9. Attach |
|
|
Methods for assessing NG tube placement |
X-ray, measure exposed tube, aspirate color, pH of aspirate |
|
|
Advantages and disadvantages of X-ray to check NG tube placement |
Most accurate Costly, increased radiation exposure |
|
|
How does color of aspirate determine NG tube placement? |
Examine color of aspirate (firstinject 10-30 mL of air to clear tube, and then pull back)—gastric aspirateshould be cloudy, grassy green, tan, off-white, or brown (intestinal aspirateshould be totally clear, yellow, or bile color), respiratory aspirate should beclear or cloudy |
|
|
pH measurement for determining NG tube placement |
1-4or 5 (gastric) ≥ 6 (intestinal) ≥ 7 (respiratory) |
|
|
Air auscultation method for determining NG tube placement |
injectinto tube and hear puff with stethoscope |
|
|
Advantages and disadvantages of using measurement of exposed tube to determine NG tube placement |
Easy and cheap Does not r/o migration to respiratory system |
|
|
Advantages and disadvantages of using aspirate color to determine NG tube placement |
Easy and cheap; good to distinguish between gastric and intestinal Does not completely r/o respiratory placement (resp and intestinal secretions can be clear); not appropriate for continuous feedings |
|
|
Advantages and disadvantages of using pH of aspirate to determine NG tube placement |
Good to distinguish between gastric v. intestinal Does not completely r/o respiratory placement; antacids, gastric resection, grossly bloody samples, continuous tube feedings can alter pH, pH monitoring equipment is not universally available |
|
|
Advantages and disadvantages of using air auscultation to determine NG tube placement |
Easy and cheap Questionable accuracy, may hear whoosing sound but tube may be in respiratory tract |
|
|
When is obstruction of NG tube suspected? What should be done before irrigating? |
Difficult to infuse or aspirate Confirm placement first |
|
|
Steps in air de-clogging method for NG tubes |
1.Inject 20 mL air with a 30 or 60 mL syringe2.Pull back plunger (should be ableto aspirate gastric or intestinal contents)3.If ineffective, repeat steps 1& 24.Use 10 mL syringe and aspirate5.If unsuccessful, call provider |
|
|
Steps in digestive enzyme method for NG tubes |
1.Use 30-60 mL syringe2.Aspirate as much liquid possible3.Instill 5 mL warm water over 1minute4.Use back and forth motion todislodge clot5.Clamp tube 5-15 minutes6.Follow steps 1-5 with enzymesolution7.Repeat once if necessary8.If unsuccessful, call provider |
|
|
Nursing management for providing oral and nasal hyfiene for those with NG tubes |
Inspect daily, change tape daily and prn, moisten mucosa, oral hygiene |
|
|
How often does passage of flatus need to be confirmed for NG tubes? |
4-8 hours |
|
|
Nursing management steps in pre-procedure for tube removal |
•Checkprovider order•AssessGI system•Gathersupplies•Washhands•Confirmpt identity•Explainprocedure•Providefor privacy•Positionin semi-fowler•Drapebarrier across chest•Usegloves |
|
|
Steps in NG tube removal |
¨Clamptest (NGtube clamped for 4-6 hours, and testing if patient can do without the tube (ifthey develop any N/V, abdominal distention) (also confirm bowel sounds andflatus continue) )¨Flushwith 30 mL air¨Un-tapetube¨Clamptube & disconnect¨Holdbreath¨Gentleand slow 6-8 inches¨Rapidfor the remainder¨Donot pull hard if resistance felt¨Oralhygiene |
|
|
What is a clamp test that is performed before NG tube removal? |
NGtube clamped for 4-6 hours, and testing if patient can do without the tube (ifthey develop any N/V, abdominal distention) (also confirm bowel sounds andflatus continue) |
|
|
When is enteral nutrition used? |
When oral intake is not adequate or not possible |
|
|
How can enteral nutrition be supplied? |
Via stomach, duodenum, jejunum |
|
|
Advantages of enteral nutrition over parenteral nutrition |
More cost effective, safer, tolerate better, easier to administer, preserves the integrity of the GI system |
|
|
Enteral feedings if the stomach needs to be bypassed: |
Nasoduodenal/jejunal feedings |
|
|
Formula characteristics to consider for enteral nutrition |
Nutrients (protein, carbohydrates, fat, vitamins, and minerals), calories, fiber, osmolality |
|
|
Why is it important to consider the osmolality of a feeding formula? |
Body osmolality is 300 mOsm/kg, higher osmolality can lead to dumping syndrome because of drawing in of water |
|
|
What are S/s of dumping syndrome? |
Feeling full, nausea, diarrhea, sweating, hypotension, tachycardia |
|
|
Types of enteral nutrition administration |
Bolus: gravity or drip Continuous Cyclic (given at night) |
|
|
How long do bolus feedings for enteral nutrition take to administer? |
500 mL bolus (gravity) typically takes 15 minutes or longer Drip bolus usually takes 30 minutes, controlled by roller clamp |
|
|
Decision tree for alterations in nutrition |

|
|
|
Precautions when using an open system for enteral nutrition |
Open systems more likely to have infection risk because formula is open to the air--- should not be hung for more than four hours |
|
|
Potential complications of enteral nutrition |
Diarrhea, N/V, gas, bloating, cramping, dumping syndrome, aspiration pneumonia, tube displacement, tube obstruction, nasopharyngeal irritation, hyperglycemia, dehydration |
|
|
What are major causes of the complications of enteral nutrition? |
Rate may be too fast, fiber too high, formula too cold (best be given at feeding formula) |
|
|
Nursing process for enteral nutrition |
Factors or illnesses that increase metabolic needs (less mobile people may need more protein to protect the skin and muscles) , hydration and fluid, renal function and electrolyte status (those with renal disease may need fluid restriction), medications (look for medications that may slow gastric motility, assess tolerance, residual checks, administer water (before and after meds, before and after feedings), do not mix medications with feedings, HOB up 30-45 degrees during feeding and one hour after |
|
|
How is tolerance to enteral nutrition assessed? |
Check residuals prior to bolus feedings and every 4-8 hours if patient is getting continuous feedings |
|
|
What residuals are concerning? |
If you calculate residual greater than 200 mL and you get this on two or more occasions, need to reevaluate the patient |
|
|
Patient positioning for enteral nutrition |
HOB up 30-45 degrees during feeding and one hour after |
|
|
Important nursing process considerations for PEG tubes, G-tubes, or J-tubes |
Skin care, teaching self-care, body image and coping, tube dislodgement, referrals |
|
|
A nasally placed feeding tube should stay in place for no more than (blank) weeks before being replaced with a new tube? |
Four |
|
|
When administering continuous or cyclic tube feedings, a primary nursing responsibility is preventing (blank)? |
Aspiration pneumonia |
|
|
T/F: The most commonly used single lumen nasogastric tube is the gastric (Salem) sump |
False (most common is Levin) |
|
|
T/F: Visualizing the placement of a nasogastric or nasoenteric tube on x-ray is the only definitive way to verify its location. |
True |
|
|
T/F: When administering oral medications to a patient receiving tube feedings, medications may be crushed and mixed with the feeding formula |
False |
|
|
Definition of obesity v. Morbid obesity |
Obesity: BMI greater than 30, or being 20% above ideal body weight Morbid obesity: greater than 100 pounds above ideal, BMI over 40 |
|
|
Prevalence of obesity/overweight in US |
One third obese, 2/3 overweight |
|
|
Pharmacological methods for managing obesity? OUtcomes? |
Xenical: prevents digestion of fat Acomplia: aids lipid and glucose metabolism-->was pulled in 2009 because of dangerous psychological side effects (suicide) Outcomes: patient rarely lose more than 10% of body weight when using pharmacological methods for morbid obesity |
|
|
Standard treatment for morbid obesity |
Bariatric surgery |
|
|
Possible mechanisms for bariatric surgeries |
Restriction, malabsorption depending on the type of surgery |
|
|
Benefits of bariatric surgery |
Report having 61% loss in body weight; recovery of chronic illness |
|
|
Criteria for bariatric surgery |
BMI of 40 or more, or BMI 35-39 with chronic condition Psychological evaluation and trial diet required before surgery |
|
|
What is a biliopancreatic diversion with duodenal switch? |
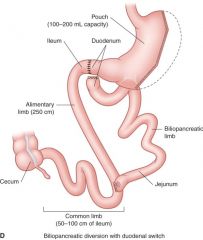
1/2 stomach removed, and a pouch that holds 100-200 mL capacity; intestines rerouted so 60% of small intestine is bypasssed so that only 20% calories are absorbed. Divides intestines into two sections: alimentary limb and the biliopancreatic limb |
|
|
Will patient have dumping syndrome with biliopancreatic diversion with duodenal switch? |
No, because pyloric valve is in place |
|
|
What is a Roux-En-Y gastric bypass? |
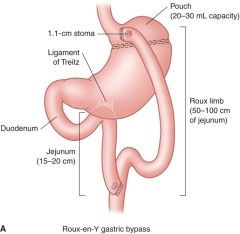
Most common procedure. Staples creat 20-30 mL pouch. Bypasses most of stomach, duodenum, jejuneum |
|
|
Does dumping syndrome occur with Roux-en-Y gastric bypass? |
Yes because pyloric sphincter is bypassed |
|
|
What is a vertical sleeve? |
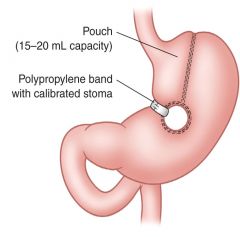
Restrictive procedure, pouch that holds 15-20 mL is created, no bypass occurs |
|
|
Benefits with vertical sleeve |
Less issues with vitamin and protein deficiencies (b/c is restrictive rather than malabsorptive) |
|
|
What is gastric banding? |
Restrictive procedure Prosthetic band creates pouch of 10-15 mL--> can be adjusted |
|
|
Mechanism of biliopancreatic diversion with DS |
Moderate restriction, moderate malabsorption |
|
|
Mechanism of RNY procedure |
Signficant restriction, mild malabsorption |
|
|
Mechanism of vertical sleeve |
Significant restriction, no malabsorption |
|
|
Mechanism of gastric banding |
Moderate restriction, No malabsorption |
|
|
Weight loss at 10 years post op: biliopancreatic diversion with DS |
80-90% loss of excess weight |
|
|
Weight loss at 10 years post op: RNY |
70% loss of excess weight |
|
|
Weight loss at 10 years post op: Vertical sleeve |
60-70% loss of excess |
|
|
Weight loss of at 10 years post-op gastric banding |
50% loss of excess weight |
|
|
Longterm dietary modification for biliopancreatic diversion with DS |
Consume less than 1000 calories QD in thefirst 12-24 months, 1200-1500 thereafterFatty foods causes diarrhea & malodorous gas/stoolNoncompliance with supplements and high protein diet--> deficiency more severe than RNYNodrinking with meals |
|
|
Longterm dietary modification for RNY |
Consume less than 800 calories QD in thefirst 12-18 months, 1000-1200 thereafterHigh sugar and fat foods causedumping syndrome 3 smallhigh protein meals per day Vitamin or protein deficiency usually preventable with supplements No drinking with meals |
|
|
Long-term dietary modification for vertical sleeve |
Consume less than 600-800 calories QD inthe first 24 months, 1000-1200 thereafterNO dumpingWeight regain may be more likely than inother procedures if dietary modifications not adopted for life No drinking with meals |
|
|
Long-term dietary modification for gastric banding |
Consume less than 800 calories QD in thefirst 24 months, 1000-1200 thereafterCertain foods can get "stuck"if eaten (rice, bread, dense meats, nuts, popcorn) causing pain and vomitingNodrinking with meals |
|
|
Potential complications of bilopancreatic diversion with DS |
Nausea and vomiting, heartburn, severediarrhea, kidney stones, stricture, ulcers (less than RNY), bowel obstruction,nutritional deficiencies (Vitamin A,D,E,K), loss of too much weight requiringsurgical intervention,leak |
|
|
Potential complications with RNY |
Dumping syndrome, stricture, ulcers, bowel obstruction, anemia,nutritionaldeficiencies (Iron, Vitamin B12, folate), leak |
|
|
Potential complications of vertical sleeve |
Nausea and vomiting, heartburn,inadequate weight loss, weight regain leading to revision, leak |
|
|
Potential complications of gastric band |
Slow weight loss, slippage, erosion, infection, port problems,device malfunction |
|
|
Nursing management for bariatric surgery |
¤Preoperativecare, evaluation and counseling ¤Postoperativecare is similar to gastric resection but the patient is at greater risk forcomplications due to obesity¤Educationregarding postoperative diet--slow progression from clear fluids to solid foods over a period of weeks ¤Psychosocialinterventions to modify eating behaviors¤Follow-upcare ¤Educationregarding long-term effects |
|
|
T/F: Afterbariatric surgery, the average patient loses between 25% and 35% of presurgical bodyweight within the first 18 to 24 months postprocedure. |
True, can lose to 60% |
|
|
T/F: Afterbowel sounds have returned and oral intake is resumed following bariatricsurgery, six small feedings consisting of a total of 600 to 800 calories perday should be consumed. |
True |
|
|
T/F: Traditionally, the term morbid obesity applies to adults whose BMI exceeds 40 kg/m2. |
True |
|
|
Risk factors for GI disorders |
Family history, lifestyle, domino effect, previous abdominal surgeries or trauma, neurologic disorders |
|
|
Definition of GERD |
Backward movement of gastric or duodenal contents into the esophagus causing heartburn. More than 2x per week make it likely that GERD is present. |
|
|
Etiology of GERD |
Relaxation of lower esophageal sphincter |
|
|
Contributions to GERD |
fatty foods, carbonated beverages (esp. those with caffeine), milk, chocolate, alcohol, peppermint and spearmint, tobacco, hormone replacement therapy, progesterone in pregnancy, having an NG tube, NSAIDs, calcium channel blockers, nitrates, pyrloric stenosis, overeating, eating before bed, tight clothing, overweight and obesity, citrus fruits, tomato products |
|
|
How does pyloric stenosis contribute to GERD? |
Delays gastric emptying into duodenum which can force LES to open |
|
|
Clinical manifestations of GERD |
Pyrosis (burning in esophagus that may radiate to upper jaw and throat), dyspepsia, sour taste, hypersalivation, dysphagia, odynphagia (painful swallowing), eructation (bleching), fullness, nausea |
|
|
Nonsurgical interventions for GERD |
Promote gastric emptying and avoid gastric distention, watch acidic foods, medications, eliminate foods, don't eat 3 hours before bed, don't lie down an hour after meals, sleep in low-fowlers |
|
|
What is surgical intervention for GERD? |
Nissen Fundoplication |
|
|
What is Nissen Fundoplication? |
Surgical intervention for GERD--- the fundus (top of stomach) is wrapped around the LES which reinforces the closing feature of the spinchter |
|
|
Risks of Nissen Fundoplication? |
Risks: bleeding, infection, and obstruction; dyphagia common for about 6 weeks post-op b/c edema, some pts may report bloating and gas buildup because of inability to belch |
|
|
What is Barrett's esophagus? |
Acid begins to erode esophagus, and cells begin to resemble those in the intestine because of prolonged acid exposure...these cells are precursor to esophageal cancer |
|
|
How is Barrett's esophagus diagnosed? |
Via endoscopy and biopsy |
|
|
Definition of hiatal hernia |
When an opening through the diaphragm where the esophagus passes (hiatus) widens and the upper part of the stomach moves into the lower part of the thorax |
|
|
Risks for hiatal hernia |
Increases with age, obesity, women> men |
|
|
Causes of hiatal hernia |
Unknown |
|
|
Concerns with hiatal hernia |
Obstruction, strangulation of bowel |
|
|
Sliding v. rolling hernia |

Sliding: most common (90-95%) when upper stomach and gastroesophageal junction are displayed and slides up and down through hiatus Rolling: all or part of stomach pushees through hiatus and sits next to esophagus |
|
|
Clinical manifestations of sliding hiatal hernia |
Can be asymptomatic, GERD symptoms |
|
|
Clinical manifestations of rolling hiatal hernia |
Can be asymptomatic, GERD symptoms, breathlessness after eating, chest pain that mimics angina, feeling of suffocation, worse lying down |
|
|
Which type of hiatal hernia has a higher risk for strangulation? |
Rolling |
|
|
S/S of strangulation with hiatal hernia |
Pain in affected area, fever, N/V MEDICAL EMERGENCY |
|
|
Interventions for hiatal hernia |
-Limitoreliminate foods that relax the lower esophageal sphincter: fatty foods, milk, caffeine, mint, chocolate, carbonated beverages, alcoholic beverages, tobacco -Promote gastric emptying or avoid gastric distention (this also helps to prevent movement of the hernia): eat small, frequent meals, do not eat 3 hours before bed, avoid laying down for 1 hour after meals, avoid tight fitting clothes, achieve a healthy weight -Limit or eliminate foods that add fuel to the acid fire d/t their acidic content: tomato or citrus products -Medication -Sleep in low fowler's position |
|
|
Definition of chronic gastritis |
When lining of stomach (mucosa) becomes inflamed or swollen and over time the mucosa can actually erode. Can be acute or chronic. |
|
|
Risk factors for chronic gastritis |
Age (40-50% have H. pylori by age 50), men and women equal in risk, HIV/AIDs, Crohn's |
|
|
Types of gastritis |
Nonerosive or erosive |
|
|
Causes of nonerosive v. erosive chronic gastritis |
Nonerosive usually caused by H. pylori (transmitted from person to person or through contaminated food or water); Erosive is usually caused by long term NSAID use or alcohol use |
|
|
Connection between chronic gastritis and pernicious anemia |
Chronic gastritis can cause pernicious anemia (parietal cells are destroyed and cannot produce intrinsic factor) |
|
|
What can make gastritis worse? |
Stress, caffeine, cigarettes, spicy food, NSAIDs |
|
|
Chronic gastritis clinical manifestations |
Anorexia, heartburn, sour taste, belching and bloating, N/V, epigastric discomfort, intolerance to spicy foods |
|
|
What happens if a patient with gastritis requires hospitalization? |
-Gastritisdiagnosed by upper endoscopy, fecal occult blood tests, monitoring for anemia -Hospitalizationusually because of blood in feces or emesis; will need to monitor blood counts-Ifptrequires hospitalization,care is usually supportive, may include NG tube to allow stomach to rest andheal (for decompression)-Pt will be on PPI, IV fluids becauseNPO, may have TPN |
|
|
Interventions for chronic gastritis |
¡H. Pylori-->combo of antibiotics¡NSAIDs,alcohol-->collaborate with health care team,educate patient, refer¡Smoking cessation¡Stressmanagement¡Avoiding trigger foods |
|
|
Definition of peptic ulcer disease (PUD) |
Sores in the lining of the GI system (stomach, upper small intestine), peptic ulcers erode beyond gastric mucosa at least 0.5 cm |
|
|
Risk factors for peptic ulcer disease Major underlying cause? |
Those with gastritis, NSAID use, 65+, family history, diet Major underlying cause is H. pylori |
|
|
Four locations for peptic ulcer disease |
Most common is duodenum, then gastric, then pylorus, and then esophagus |
|
|
Clinical manifestations of peptic ulcer disease |
Dull, gnawing, burning pain; mid epigastric area, can manifest posteriorlly to the thoracic or lumbar region (back), also heartburn, diarrhea, constipation, bloody stool or emesis--> if blood loss is significant may see s/s of anemia |
|
|
How is dx of peptic ulcer disease made? |
Endoscopy |
|
|
Differences between duodenal and gastric ulcers |
Duodenal: 2-3 hours after meal pain, pain occurs at night, pain relieved by food, hypersecretion of stomach acid, weight gain Gastric: Pain immediately after a meal or 30-60 minutes after meal, pain rarely at night, pain worse with food, normal or hypoactive stomach acid secretion, weight loss |
|
|
Timing of pain for duodenal v. gastric ulcers |
Duodenal: 2-3 hours after meal, occurs at night, relieved by food Gastric: Immediately after a meal, or 30-60 minutes after meal, rarely at night, worse with food |
|
|
Stomach acid secretion for duodenal v. gastric ulcers |
Duodenal: hypersecretion Gastric: Normal or hyposecretion |
|
|
Weight change in duodenal v. gastric ulcers |
Duodenal: weight gain Gastric: weight loss |
|
|
Treatments for duodenal and gastric ulcers |
Antibiotics, bismuth salts (suppresses H. pylori), PPIs, NG tubes for decompression, pt may need to have region near pylorus dilated to alleviate obstruction |
|
|
Complications of peptic ulcer disease |
15% will have hemorrhage, perforation and penetration, gastric outlet obstruction (pyloric area gets scar tissue and becomes stenosed) |
|
|
When is surgical intervention for peptic ulcer disease advised? |
If obstruction or perforation present; or ulcer won't heal over 12-16 weeks |
|
|
Types of surgical interventions for peptic ulcer disease |
-Vagotomy: Vagus nerve is cut to decrease gastric acid secretion -Pyloroplasty:Pylorus is widened to facilitate emptying -Antrectomy (Bilroth I):Pylorus is removed and stomach connected to duodenum -Antrectomy Billroth II: Pylorus is removed and stomach connected tojejunum |
|
|
What is a vagotomy? |
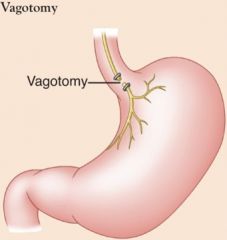
Surgical intervention for peptic ulcer disease; vagus nerve is cut to decrease gastric acid secretion |
|
|
What is a pyloroplasty? |
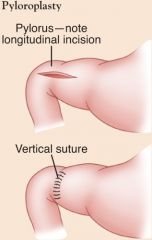
Surgical intervention for peptic ulcer disease; pylorus is widened to facilitate emptying |
|
|
What is a Bilroth I procedure (Antrectomy)? |
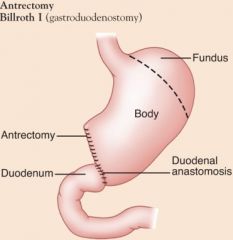
Surgical intervention for peptic ulcer disease; Pylorus is removed and stomach connected to duodenum |
|
|
What is a Billroth II procedure (antrectomy)? |
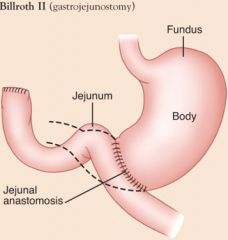
Surgical intervention for peptic ulcer disease; pylorus is removed and stomach connected to jejunum |
|
|
Nursing interventions for peptic ulcer disease |
Pain, fluid and nutrition balance, anxiety, home and community-based care |
|
|
T/F: Mostpeptic ulcers result from infection with the gram-negative bacteria H. pylori, which may be acquired through ingestionof food and water. |
True |
|
|
Currently, the most commonly used therapy for peptic ulcers is a combination of (blank), proton pump inhibitors, and bismuth salts that suppresses or eradicated H. pylori |
Antibiotics |
|
|
Definition of chronic constipation |
Constipation is a symptom not a disease. Defined as having less than 3 BMs per week and stool is hard, volume is decreased. Symptoms present 12 weeks over a 12 month period of time. |
|
|
Clinical manifestations of chronic constipation |
Manifests with straining, pain and pressure, sensation of incomplete evacuation, hard stools-- also headaches, decreased appetite, indigestion, fatigue, abdominal distention |
|
|
Causes of chronic constipation |
Low fiber diet, ignoring urge to defecate, inadequate fluid intake (less than 8 glasses a day), sedentary lifestyle, certain medications (antidepressants, opioids), neuromuscular disorders (MS, Parkinson's), endocrine dx (hypothyroidism), spinal cord injuries |
|
|
Complications of chronic constipation |
Hemorrhoids, fissures, megacolon, obstruction, impaction |
|
|
Definition of chronic diarrhea |
More than 3 BMs a day with increased volume, persists for 2-3 weeks and then returns sporadically over time |
|
|
Clinical manifestations of chronic diarrhea |
Urgency, peri-anal discomfort, cramps ,anorexia, thirst, intestinal rumbling |
|
|
Causes of chronic diarrhea |
Medications (antibiotics), tube feedings, diseases (IBS, IBD), C. diff |
|
|
Complications of chronic diarrhea |
Cardiac abnormalities/dysrhythmias, dehydration, alteration in skin integrity |
|
|
Stool characteristics corresponding to certain disorders |
Watery--small bowel disorder Loose, semi-solid--large bowel disorder Voluminous, greasy-- malabsorptive disorder Blood, mucus, pus--inflammatory disorder Oil droplets: pancreatic insufficiency Nocturnal: diabetic neuropathy |
|
|
What age range is at greatest risk for IBD? |
15-30 |
|
|
Definition of ulcerative colitis |
Recurrent ulcerative and inflammatory disease of mucosal and submucosal layers of rectum and colon; continuous lesions |
|
|
Definition of Crohn's disease |
AKA regional enteritis Subacute and chronic inflammation of GI wall that spreads deep into layer of GI tissue (typically in ileum or ascending colon, cobblestone appearance) |
|
|
Location of Ulcerative colitis v. Crohn's disease |
UC: Colon Crohn's disease: Mouth to anus |
|
|
Lesions in ulcerative colitis v. Crohn's disease |
UC: contiguous Crohn's disease: not contiguous (cobblestone) |
|
|
Course for ulcerative colitis v. Crohn's disease |
UC: exacerbations and remissions Crohn's: prolonged bouts |
|
|
Diarrhea in ulcerative colitis v. Crohn's disease |
UC: more severe (10-20 bouts QD) Crohn's: less severe (5-6 bouts QD) |
|
|
Symptoms of ulcerative colitis v. Crohn's disease |
UC: LLQ pain, passage of mucous and pus, tenesmus (ineffective painful straining), rectal bleeding, anorexia Crohn's: RLQ crampy pain, eating stimulates cramps, anorexia, steatorrhea (fatty stool), fever |
|
|
Bleeding for ulcerative colitis v. Crohn's disease |
UC: Common and severe Crohn's: not common and mild` |
|
|
Fistulas in ulcerative colitis v. Crohn's disease |
UC: rare Crohn's: Common |
|
|
Complications of ulcerative colitis v. Crohn's disease |
UC: Perforation; Toxic megacolon--bowel perforation Crohn's: Bowel obstruction, abscesses, colon cancer |
|
|
Surgery for ulcerative colitis v. Crohn's disease |
UC: curative Crohn's: not curative |
|
|
How are ulcerative colitis and Crohn's disease diagnosed? |
Both diagnosed with colonscopy |
|
|
Common complication of IBD |
Nutritional imbalance |
|
|
Goals of IBD |
Manage: bowel elimination, pain, fluid volume, nutrition, fatigue, anxiety, coping, skin, knowledge, self-health, complications |
|
|
Interventions for IBD |
Diet, activity, and stressors management. Provide ready access to restroom or commode. Manage pain. Fluid volume. Low residue diet. Rest. Anxiety and coping management. Skin care, Understanding and self-care. |
|
|
What is a low-residue diet for IBD? |
Well-cooked tender meat, poultry and fish, milk and mild cheeses, juices without pulp, canned fruit and firm bananas, white or refined bread, no raw veggies, no skin or seeds |
|
|
Definition of IBS |
Chronic functional bowel disorder |
|
|
Causes of IBS |
Unknown: stress hormones, hereditary |
|
|
How is IBS diagnosed? |
No diagnostic test for IBS, based on s/s |
|
|
Clinical manifestations of IBS |
Constipation, diarrhea, combo, abdominal pain, distention |
|
|
Interventions for IBS |
Education, dietary habits (avoidance of trigger foods), chew food thoroughly and don't drink fluids with meals, stress management |
|
|
T/F: Thepatient with irritable bowel syndrome (IBS) should select foods low in fiber inorder to minimize intestinal irritation |
False |
|
|
In Crohn’s disease, the clusters of ulcerations onthe intestinal mucosa have a _______ appearance. |
Cobblestone |
|
|
Two types of intestinal obstruction |
Mechanical and functional |
|
|
Mechanical v. functional intestinal obstruction |
Mechanical: obstruction is derivedfrom an external pressure on the intestinalwall that prevents normal flow (ex. intussusception—folds in on self,neoplasms, strictures, adhesions, hernia, swallowing an object) Functional:intestinal musculature—muscle and nerves, cannot move contents along the bowels(medications—opioids, muscular dystrophy, parkinson’s) |
|
|
Where do intestinal obstructions most likely occur? |
Small intestine |
|
|
Small bowel v. large bowel intestinal obstructions |
Small bowel: adhesions, hernias, and neoplasms Large bowel: carcinomas, diverticulitis, benign tumors |
|
|
Clinical manifestations of small bowel v. large bowel intestinal obstruction |
Small bowel: Fast to develop. Colicky (sharp), wave-like pain. Blood and mucus but no fecal matter or flatus. Abdominal distention. Fecal vomiting. Weakness, weight loss, anorexia, dehydration, shock Large bowel: Slow to develop. Crampy lower abdominal pain. Weirdly shaped stool, blood in stool. Abdominal distention. Fecal vomiting. Weakness, weight loss, anorexia, dehydration, shock. |
|
|
Management of small bowel v. large bowel intestinal obstruction |
Small bowel: IV, Ng tube for decompression, fluid and electrolyte replacement, surgery (if tissue is strangulated), fix root cause Large bowel: IV, NG tube for decompression, fluid and electrolyte replacement, surgery (resection)--may need temporary or permanent colostomy, fix root cause |
|
|
T/F: Decompression of the bowel through a nasogastric tube is neccessary for all patients with small bowel obstruction |
True |
|
|
General nursing considerations for post-op GI surgery |
1.Resumingenteral intake IDepends on return of bowel sounds, start with liquids and advance as tolerate until can tolerate 8 small meals with 120 mL between meals) 2.Dysphagia3.Gastricretention (may occur from advnacing feedings too quickly) 4.Bilereflux (any surgery with pylorus removal) 5. Dumpingsyndrome6.Vitamin& mineral deficiencies |
|
|
Indications for intestinal diversions |
Cancer, trauma, IBS, diverticulitus, bowel obstruction |
|
|
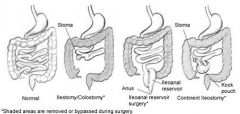
What are ileostomies? |
-Diverts ileum to a stoma -Bypassesthe entire large intestine (colon, rectum, and anus), so stools areliquid, frequently contain digestive enzymes, and must be pouched at all times |
|
|
Possible locations for colostomies |
Sigmoid, descending, transverse, ascending |
|
|
Characteristics of stool depending on colostomy location |
-Sigmoid:solid; water has been absorbed through ascending and transverse -Descending:semisolid; less irritating -Transverse:middle or right side of abdomen; mushy; effluent more irritatingbcrich in gastric enzymes -Ascending:right side of abdomen; semi liquid- rich in digestive enzymes; irritating to skin |
|
|
What is an ileoanal reservoir? |
-Essentially createsa “new rectum” -Large intestine is removed but the anus remainsintact and disease-free -The surgeon creates a colon-like pouch (ileoanalreservoir) from the last several inches of the ileum -Requires two surgeries: temporaryileostomy (3-4 months) to give the pouch time to stretch and heal -Stool collects in the ileoanalreservoir and then exits the body through the anus during a bowel movement;initially up to 10 bowel movements per day then down to 4-6 |
|
|
What is a continent ileostomy (Kock pouch)? |
-For patients who arenot good candidates for ileoanal reservoir surgery because of damage to therectum or anus but do not want to wear an ostomy pouch -The large intestine is removed and acolon-like pouch, called a Kockpouch, is made from the end of the ileum -Effluent is drained by inserting a catheter into a valve |
|
|
Areas bypassed in ileostomy/colostomy, ileoanal reservoir surgery, and continent ileostomy |
|
|
|
Basic assessments, size for ostomies |
Stomas should not produce pain for patient, color should be beefy red and moist, 1/2 to 1 inch protrusion |
|
|
How long does it take for edema from ostomy creation to go down? |
6 weeks |
|
|
When does effluent from ostomies occur? |
Colostomy drains when peristalsis occurs; ileostomy produces effluent within 24-48 hours of surgery |
|
|
How often is ostomy pouch emptied? Appliance? |
When 1/2 to 3/4 full (4-6 times per day) Entire appliance changed 5-10 days |
|
|
Medication consideration for individual with an ostomy |
No enteric coated or capsule medication |
|
|
Process of ostomy irrigation |
§Use 500 to 1500mL of warm tap water to irrigate remaining colon if needed§Attach sleeve & cone to colostomy§Irrigate gently§May take ½ hour to fully expel |
|
|
Purpose of ostomy irrigation |
To stimulate emptying at scheduled times (decreases occurrences of unexpected bowel movements), gives patient control |
|
|
T/F: The patient with an ileostomy with a Kochpouch will not need to use an external fecal collection bag. |
True |
|
|
Who has increased prevalence of esophageal cancers? |
Men>women, African Americans>Caucasians; clusters in China and Iran |
|
|
Risk factors for esophageal cancer |
Barrett's esophagus, smoking, alcohol use, GERD |
|
|
Clinical manifestations of esophageal cancer |
Dysphagia, weight loss, weakness |
|
|
How is esophageal cancer diagnosed? |
Biopsy, endoscopy |
|
|
Which groups is gastric cancer more prevalent in? |
Men>women, Native, Hispanic, African Americans> Caucasians, clusters in Japan |
|
|
Risk factors for gastric cancer: |
Diet, smoking ,gastritis, H. pylori |
|
|
Treatment for esophageal cancer |
Chemo and radiation, resection of teh esophagus |
|
|
Clinical manifestations of gastric cancer How is diagnosis made? |
Few sx until advanced cancer Diagnosed via CT scan |
|
|
How is gastric cancer treated? |
Chemo and radiation (may be palliative), total gastrectomy (if it has not spread) |
|
|
What are duodenal tumors and how are they usually found? Signs and symptoms? |
Usually benign. Usually found unintentionally during a scan. Individuals usually asymptomatic, but if severe, may have intermittent pain and occult bleeding. |
|
|
Treatment for duodenal tumors |
Surgery |
|
|
Risk factors for colorectal cancer |
Increasing age (>50), family hx of colon cancer or polyps, high consumption of ETOH, cigarette smoking, obesity, history of gastrectomy, history of inflammatory bowel disease, high-fat, high--protein (with high intake of beed), low-fiber. Genital cancer endometrial CA, ovarian CA) or breast CA in women) |
|
|
3rd most common cause of cancer death |
Colorectal |
|
|
Most common manifestations of colorectal cancer |
Change in bowel habits, passage of blood in stool, unexplained anemia, weight loss, fatigue |
|
|
Most common cancer diagnosis in colorectal cancer |
Adenocarcinoma |
|
|
Diagnosis for colorectal cancer |
Colonscopy and biopsy |
|
|
Symptoms of right sided lesions in colorectal cancer |
Dull abdominal pain, melena |
|
|
Symptoms of left sided lesions in colorectal cancer |
Abdominal pain, cramping, narrowed stools, constipation, distention, bright red blood |
|
|
Symptoms of rectal lesions in colorectal cancer |
Tenesmus (recurrent inclination to evacuate bowels--cramping with straining), rectal pain, feeling of incomplete evacuation after a BM, alternating constipation and diarrhea, bloody stool |
|
|
The etiology of cancer of the colon andrectum is predominantly (90%) _______, a malignancy arising from the epitheliallining of the intestine. |
Adenocarcinoma |
|
|
Select all of the potential complications associated with enteral nutrition.a.Intolerance to feeding formulab.Pneumothoraxc.Dumping syndromed.Aspiration |
Intolerance to feeding, dumping syndrome, and aspiration |
|
|
The nurse is planning discharge teaching for the client with GERD. What dietary modificaiton should be included? 1.Eatthree meals and a bedtime snack.2.Avoidintake of caffeine and alcoholic beverages.3.Drink12 - 16 ounces of water with each meal.4.Liedown for 15 – 20 minutes after eating.iD-(EX>pO+е+`P@@6X[+' |
2. Avoid intake of caffeine and alcoholic beverages |
|
|
Which client comment indicates to thenurse that more teaching is needed for the client experiencing dumping syndromeafter gastric surgery? 1.“Ishould eat six small meals per day.”2.“Ishould not drink fluids with my meals.”3.“Ishould use honey or jelly instead of butter.”4.“Ishould lie down for 30 – 60 minutes after eating.” |
3. I should use honey or jelly instead of butter |
|
|
A client is placed on enteral feedingsvia nasogastric tube to meet nutritional goals. Which intervention should thenurse include in the plan of care to help maintain fluid balance?1.Assessthe skin around the tube site.2.Weighthe client every other day.3.Maintainstrict I&O and flush the tube once a day to ensure patency.4.Irrigatethe tube with water as ordered and include this fluid in total I&O. |
4.Irrigate the tube with water as ordered and include this fluid in total I&O. |
|
|
Which landmarks should the nurse use tocorrectly measure a client prior to nasogastric tube insertion? Select all thatapply.●1.Tipof nose2.Sternalnotch3.Mandibularjoint4.Tipof earlobe5.Xiphoidprocess |
1. Tip of nose 4. Tip of earlobe 5. Xiphoid process |
|
|
A nurse is assigned to a client with anasogastric tube and is checking gastric pH to verify correct tube placement.Which pH reading should the nurse expect if the tube is properly positioned? 1.42.63.74.8 |
1. 4 |
|
|
A client underwent insertion of a nasoenterictube for partial bowel obstruction the previous evening. The nurse notes thatthe tube is not taped at the nose. Which of the following actions is mostappropriate at this time?1.Callthe physician immediately.2.Securelytape the tube in place.3.Notethe finding on the client’s flowsheet.4.Callthe radiology department to schedule an abdominal x-ray. |
3.Note the finding on the client’s flowsheet. |
|
|
The nurse has an order to insert anasogastric tube into the stomach of an assigned client. In what order shouldthe nurse perform the actions to complete the procedure? Place the options inthe correct order. All options must be used.1.Placedistal end of tube at tip of nose and measure to earlobe and then to xiphoidprocess to determine distance for tube insertion.2.Inserttube into the nares and advance upward and backward until resistance is met;rotate catheter gently and advance into nasopharynx.3.Sitthe client upright in a high Fowler’s position.4.Asclient to take sips of water if able while tube advanced gently into stomach5.Tapetube to the client’s nose to hold it securely in place. |
3, 1, 2, 4, 5 |
|
|
The client who has ulcerative colitis isscheduled for an ileostomy. When the client asks the nurse what to expectrelated to bowel function and care after surgery, what response should thenurse make?1.“Youwill be able to have some control over your bowel movements.”2.“Thestoma will require that you wear a collection device all the time.”3.“Afterthe stoma heals, you can irrigate your bowel so you will not have to wear apouch.”4.“Thedrainage will gradually become semisolid and formed.” |
2. “Thestoma will require that you wear a collection device all the time.” |
|
|
A client with diverticular diseaseundergoes a colonoscopy. During the abdominal assessment, the nurse looks forwhich sign to indicate a possible complication of the procedure?1.Diarrhea2.Nauseaand vomiting3.Guardingand rebound tenderness4.Rednessand warmth of the abdominal skin |
Guarding and rebound tenderness |
|
|
A client is being evaluated for possibleduodenal ulcer. The nurse assesses the client for which manifestation thatwould support this diagnosis?1.Epigastricpain relieved by food2.Historyof chronic aspirin use3.Distendedabdomen4.Positivefluid wave |
1. Epigastric pain relieved by food |
|
|
The client returning from a colonoscopyhas been given a diagnosis of Crohn’s disease. The oncoming shift nurseexpects to note which manifestation in the client? Select all that apply.•1.Steatorrhea2.Form,rigid abdomen3.Constipation4.Enlargedhemorrhoids5.Diarrhea |
1. Steatorrhea 5. Diarrhea |
|
|
The client with a duodenal ulcer asks thenurse why an antibiotic is part of the treatment regimen. Which informationshould the nurse include in the response?1.Antibioticsdecrease the likelihood of a secondary infection.2.Manyduodenal ulcers are caused by the Helicobacter pylori organism3.Antibioticsare used in an attempt to sterilize the stomach.4.Manypeople have Clostridium difficile,whichcan lead to ulcer formation. |
2. Many duodenal ulcers are caused by the H. pylori organism |
|
|
A client has a nasogastric (NG) tube inplace for gastric decompression and complains of increasing nausea. Whichaction should the nurse take first?1.Advancethe tube 2cm2.Placeclient in a recumbent position3.Irrigatewith 20ml of saline4.Obtainabdominal x-ray to assess placement |
3. Irrigate with 20 mL of saline |
|
|
A client with a subtotal gastrectomy isscheduled for discharge. Which instruction should the nurse give the client toreduce the possibility of dumping syndrome?1.“Besure to eat foods high in complex carbohydrates.”2.“Itis helpful to take a walk after eating.”3.“Avoiddrinking fluids with your meal.”4.Don’tlie down for at least 2 hours after eating.” |
3. Avoid drinking fluids with your meal |
|
|
The client with a gastric ulcer isadmitted to the hospital. The nurse should assess the client for intake ofwhich substance that increases the risk of developing a gastric ulcer?1.Aspirin2.Chili3.Acetaminophen(Tylenol)4.Coffee |
1. Aspirin |
|
|
The client is admitted to the hospitalwith ulcerative colitis. The nurse should assess the client for which sign thatindicates a complication of the disease?1.Lowhemoglobin and hematocrit2.Lowplatelet count3.Epigastric orright-sided pain following a high-fat meal4.Presenceof fat in the stools |
1. Low hemoglobin and hematocrit |
|
|
The client returns to the nursing unitpostoperatively after a colostomy. Which of the following assessments wouldrequire immediate action by the nurse?1.Stomais bright red2.Stomais bluish3.Stomais draining serous fluid4.Stomais draining no fluid |
2. Stoma is bluish |
|
|
The client with irritable bowel syndrome(IBS) asks the nurse what causes the disease. Which response by the nurse wouldbe most appropriate?1.“Thisis an inflammation of the bowel caused by eating too much roughage.”2.“IBSis caused by a stressful lifestyle.”3.“Thecause of this condition is unknown.”4.“Thereis thinning of the intestinal mucosa caused by ingestion of gluten.” |
3. The cause of this condition is unknown |