![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
99 Cards in this Set
- Front
- Back
|
Inguinal hernia diagrams |
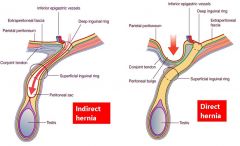
Image |
|
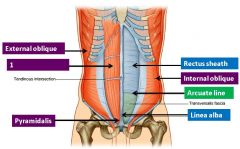
What is denoted by label 1 on this image of the anterior abdominal wall? |
Rectus abdominis |
|

What is denoted by label 1 on this image of the anterior abdominal wall? |
Internal oblique |
|
|
What is the function of the transversus abdominis? |
Compress contents, increase intra-abdominal pressure Important in childbirth (parturition), urination (micturition), defecation |
|
|
What is the function of the external obliques? |
Flexes and rotates - turns anterior abdomen to opposite side |
|
|
What is the function of the internal obliques? |
Flexes and rotates - turns anterior abdomen to same side |
|
|
What is the function of the rectus abdominis? |
Flexes and tenses |
|
|
/What is the function of the pyramidalis? |
Tenses linea alba |
|
|
What forms the rectus sheath? |
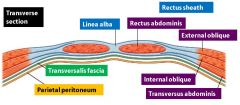
Aponeuroses of internal oblique, external oblique and transversus abdominis |
|
|
What are aponeuroses? |
Pearly-white fibrous tissue that takes the place of tendons in sheet-like muscles with a large area of attachment |
|
|
How does the rectus sheath vary vertically? |
Rectus abdominis enclosed by three aponeurotic layers above arcuate line (75%) Covered by all three below arcuate line (25%) |
|
|
What is the inguinal canal? |

A passageway through abdominal layers |
|
|
What components make up the inguinal canal? |
Spermatic cord (male) or round ligament (female) Genital branch of genitofemoral nerve Ilio-inguinal nerve |
|
|
How is the inguinal canal formed? |
Invagination of processus vaginalis |
|
|
What are the contents of the spermatic cord? |
Vas deferens Artery to ductus deferens Testicular artery Veins - pampiniform plexus Cremasteric vessels Genital branch of genitofemoral nerve Sympathetic nerves Lymphatics Processus vaginalis remnant Ilioinguinal nerve |
|
|
What allow entry of the spermatic cord through the inguinal canal? |
Deep inguinal ring in transversalis fascia Internal spermatic fascia is extension of transversalis fascia over the spermatic cord |
|

What forms the conjoint tendon in the inguinal canal? |
Internal oblique aponeurosis and transversus abdominis |
|
|
How does a direct inguinal hernia present and what causes it? |
Peritoneal bulge before spermatic cord/ round ligament Weakened musculature of posterior wall of inguinal canal - Medial to inferior epigastric vessels |
|
|
How does an indirect inguinal hernia present and what causes it? |
Patent processus vaginalis, lateral to inferior epigastric vessels Hernia passes through inguinal canal, can cause bowel obstruction, strangulation of blood supply More common than direct, more common in men due to wider inguinal canal |
|
|
What are the other types of abdominal hernia? |
Diaphragmatic - Failure in fusion during develpment causes weakening/ openings Hiatus - Fundus of stomach herniates oesophageal hiatus Umbilical - Rare, congenital Paraumbilical - Adult Femoral - Passes through femoral canal |
|
|
What is connected to the diaphragm superiorly? |
Central tendon No bony attachment, fibrous pericardium is attached |
|
|
What is connected to the diaphragm inferiorly? |
Costal margin Posterior abdominal wall Lumbar vertebrae |
|
|
Where are the crura of the diaphragm located? |
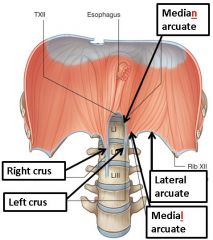
Right: L1-3 Left: L1-2 |
|
|
What are the three arcuate ligaments attached to the diaphragm? |
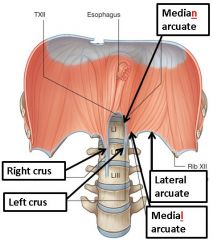
Median (aorta) Medial (psoas major) Lateral (quadratus lumborum) |
|
|
What are the features of the skeletal muscle component of the diaphragm? |
60% slow-twitch fibres Increased fatigue-resistant fibres for endurance Higher oxidative capacity and larger blood-flow than limb muscles |
|
|
How is the diaphragm innervated? |
Mostly by phrenic nerve C3-5 Marginal part innervated by spinal nerves T6-12 Crura by spinal nerves from T12 Contracts as a single unit |
|
|
Where do the phrenic nerves pass through the diaphragm? |
Right: Through caval opening (T8) Left: Through diaphragm itself |
|
|
Liver anatomy |
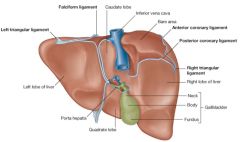
Image |
|
|
Extrahepatic biliary system |
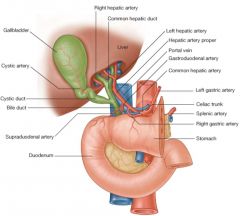
Image |
|
|
Gallbladder anatomy |
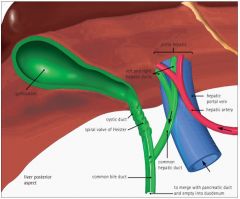
Image |
|
|
Spleen anatomy |
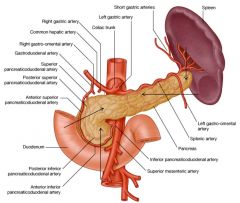
Image |
|
|
Pancreas anatomy |
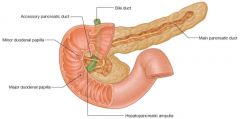
Image |
|
|
Which veins unite to form the portal vein? |
Superior mesenteric and splenic |
|
|
Where does the union leading to the portal vein happen? |
Behind the neck of the pancreas |
|
|
Why are portal systemic anastomoses clinically important? |
In cases of portal hypertension, varices/ venous dilations can form when blood is shunted into collateral vessels Can result in as little as 20% of portal blood reaching the liver |
|
|
What clinical conditions may arise if the sphincter of Oddi became blocked by a gall stone? |
Would result in blockage of both bile and pancreatic juice, causing gall stone pancreatitis |
|
|
What is the arterial supply of the pancreas? |
Neck, body and tail: splenic artery Head: inferior and superior pancreaticoduodenal arteries |
|
|
How can the jejunum and ileum be distinguished from each other? |
Position in abdomen Calibre (thickness) Fat in mesentery Organisation of arterial arcades Microanatomy of walls |
|
|
What are taenia coli, haustra and appendices apiploicae? |
Taenia coli: longitudinal SM Haustra: folds in walls Appendices epiploicae: fatty appendages |
|
|
In what region of the abdomen does the pain of appendicitis normally begin as a vague sensation? |
Umbilical |
|
|
What is the superficial inguinal ring? |
Exit of the inguinal canal - opening in aponeurosis of external oblique Pubic crest sits at base |
|
|
What is the deep inguinal ring? |
Entrance to inguinal canal Immediately lateral to superior epigastric artery |
|
|
What is the cremasteric reflex? |
Reflex from stimulation of sensory ilioinguinal nerve in the anterior thigh causes contraction of cremaster muscle in the spermatic cord that elevates the testis through the genital branch of the genito-femoral nerve |
|
|
Renal anatomy |
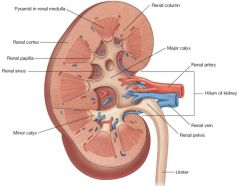
Image |
|
|
What is the role of the diaphragm in respiration? |
Contracts and lowers during inspiration to increase volume of the thoracic cavity |
|
|
What is the action of the psoas major? |
Flexion of thigh at hip (as iliopsoas) |
|
|
What is the action of the psoas minor? |
Weak flexion of vertebral column Sometimes absent |
|
|
What is the action of the quadratus lumborum? |
Lateral bending, accessory respiratory muscle |
|
|
What is the action of the iliacus? |
Flexes thigh at hip (as iliopsoas) |
|
|
What are the differences in the anatomy of the right and left suprarenal gland? |
Right is pyramid shaped, left is crescent shaped |
|
|
What is the sole motor supply to the diaphragm? |
Phrenic nerve |
|
|
What structures unite to form the ampulla of Vater? |
Bile duct, pancreatic duct |
|
|
What is the ampulla of Vater? |
Where the pancreatic duct joins the bile duct at the major duodenal papilla |
|
|
What controls the entrance to the duodenum? |
Sphincter of Oddi |
|
|
What are the features of the submandibular gland? |
70% flow 4:1 serous:mucous Stimulated by CN VII |
|
|
What are the features of the parotid gland? |
25% flow 20:1 serous:mucous Stimulates by CN IX |
|
|
What are the features of the sublingual gland? |
5% flow 3:7 serous:mucous ratio Stimulated y CN VII |
|
|
What is xerostomia? |
Dryness of the mouth |
|
|
What is sialorrhea? |
Clinical term for excessive salivary production |
|
|
What is sialadenitis? |
Clinical term for inflammation of glands |
|
|
What is sialolithiasis? |
Clinical term for a stone in the duct of a gland |
|
|
What converts trypsinogen to trypsin? |
Enteropeptidase |
|
|
What is portal hypertension? |
Increased pressure in portal system >10 mmHg Opens up anatomoses at junction, contributes to ascites |
|
|
What might liver function tests show in liver disease? |
Low serum albumin Prolonged PT |
|
|
What is diarrhoea? |
Loss of fluid and electrolytes (>500ml/ day) from the GI tract |
|
|
What is osmotic diarrhoea? |
Caused by malabsorption. Can be triggered by laxatives (magnesium salts), non-absorbed foods (sorbitol) or congenital/ acquired disorders of digestion (lactase deficiency, glucose-galactose malabsorption) |
|
|
What is secretory diarrhoea? |
Ion transport defect. Imbalance between secretion and absorption. Can be triggered by enterotoxins (E. coli, cholera), laxatives (sodium bases, ricinoleic acid, alow), hormone secreting tumours (VIP, serotonin), medication, allergy |
|
|
What is the cause of motility disturbance? |
Insufficient time for absorption |
|
|
How is diarrhoea treated? |
Oral rehydration fluids (kaolin, chalk), reduce motility (morphine, opiate analogues), inhibit secretion (opiates, NSAIDs), antibiotic and probiotic therapy |
|
|
What are the features of glucokinase? |
Found in the liver High affinity for glucose (high Km) High capacity for glucose (V(max)) Stimulated by glucose (feed forward), NOT inhibited by glucose 6-P |
|
|
What are the features of hexokinase? |
Found in most tissues High affinity for glucose (high Km) Low capacity for glucose (V(max)) Inhibited by glucose 6-P (increased cell energy) |
|
|
What is the benefit of storing glucose as glycogen? |
Glucose is osmotically active. If stored as free the high concentration would cause massive water uptake, cell lysis |
|
|
What is the link reaction? |
Pyruvate (3C) converted to Acetyl CoA (2C) by pyruvate dehydrogenase complex CoA in, CO2 out, NAD+ reduced to NADH |
|
|
What enzymes form complex I of the electron transport chain? |
CoQ Oxyreductase NADH dehydrogenase NADH passes electrons into this complex |
|
|
What enzymes form complex II of the electron transport chain? |
Succinate dehydrogenase FADH2 passes electrons into this complex |
|
|
What do complexes I and II feed electrons into? |
Coenzyme Q |
|
|
What does coenzyme Q feed electrons into? |
Cytochrome bc-1 (complex III) Then Cytochrome C |
|
|
What does Cytochrome C feed electrons into? |
Cytochrome C Oxidase (complex IV) |
|
|
What is the final complex that Cytochrome C Oxidase transfers electrons to? |
Oxygen - lack of it means ETC stops |
|
|
What is ATP synthase and why is it important? |
Proton transport creates electrochemical gradient (chemiosmosis) Protons reenter matrix through ATP synthase which converts ADP to ATP by oxidative phosphorylation |
|
|
What is the effect of carbon monoxide/ cyanide on the electron transport chain? |
Inhibits transfer of electrons from complex IV to oxygen. ATP production ceases, causes rapid cell death |
|
|
What is the effect of Oligomycin on the electron transport chain? |
Inhibits proton movement through complex V (ATP synthase) - ATP production ceases |
|
|
What is the effect of dinitrophenol on the electron transport chain? |
An uncoupling chemical that allows protons to pass through the inner membrane, bypassing complex V (ATP synthase) ATP production ceases |
|
|
How does non-shivering thermogenesis happen in brown adipocytes? |
Uncoupling proteins create proton leak on inner mitochondrial membrane, uncoupling the proton gradient Protons bypass complex V |
|
|
What is the function of fructokinase? |
Catalyses fructose --> fructose 1-P |
|
|
What is essential fructosuria? |
Fructokinase deficiency Benign condition, accumulation of fructose in urine Autosomal recessive |
|
|
What is the function of aldolase B? |
Catalyses fructose 1-P --> DHAP + Glyceraldehyde Deficiency results in Hereditary fructose intolerance |
|
|
What is hereditary fructose intolerance? |
During weaning, child develops: Convulsions Excessive sleepiness Irritability Poor feeding Vomoting All exacerbated after eating fructose/ sucrose Liver function tests show severe liver damage, blood tests show hypoglycaemia |
|
|
What pathway converts excess glycogen to fatty acids and triglycerides? |
Glucose Pyruvate (pyruvate dehydrogenase) Acetyl CoA (Acetyl-CoA carboxylase) Malonyl CoA Fatty acids (fatty acid synthase) - Requires NADPH - pentose phosphate pathway Esterified with glycerol to triglyceride, packed into VLDL and secreted |
|
|
What is cirrhosis? |
Scarring of the liver caused by continuous, long term liver damage. Scar tissue replaces healthy tissue in the liver and reduces overall function |
|
|
What causes cirrhosis? |
Drugs and toxins Infections (chronic viral hep B/C) Autoimmune (hepatitis, biliary, cholestasis) Metabolic (haemochromatosis) |
|
|
What are the complications associated with cirrhosis? |
Hepatic failure Portal hypertension Development of hepatocellular carcinoma |
|
|
What is primary acinar salivary secretion? |
Isotonic, plasma like (Na+ and Cl-) Mucin glycoprotein secretion Proline-rich secretion IgA secretion |
|
|
What is secondary ductal modification of salivary secretion? |
Lysozyme and K+ secretion in first section K+, HCO3- secretion and Cl-, Na+ reabsorption in second section |
|
|
What are the features of the exocrine portion of the pancreas? |
98% total production (other 2% is insulin, glucagon) Secretes digestive enzymes (Zymogens) for digestion of food as well as fluid and HCO3- to wash out enzymes and neutralise stomach acid |
|
|
What are the features of pancreatic salivary glands? |
Not as vascularised as in salivary glands NaCl secretion, isotonic 25% fluid secreted here as opposed to 100% in salivary acini |
|
|
What are the features of pancreatic ducts? |
Stimulated by Secretin Secrete large volume of fluid as well as HCO3- Apical membrane has CFTR Cl- channels and Cl-/HCO3- exchange. Isotonic, makes blood slightly more acidic, neutralises alkaline effect of CO2 absorption |
|
|
How are pancreatic secretions controlled during the cephalic and gastric phases? |
Vagus (ACh) stimulates short term acinar, to a lesser degree ductal secretion 30-40% secretory response via vagus Gastrin produced which binds to CCK receptors (weak) 25% from cephalic phase |
|
|
How are pancreatic secretions controlled during the intestinal phase? |
Vagus nerve, also hormones to provide strong stimuli, long term secretion Cholecystokinin-pancreozymin (CCK-PZ) At least 60% of all pancreatic secretion is driven by endocrine (hormonal) factors in intestinal phase |