Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Absent mitochondria in center of type 1 fibers.
|

Central Core Disease
|
|
|
|
Mutations of the Z bands where actin inserts. There are inclusions in the cells that look like rods.
|

Nemaline Myopathies
|
|
|
|
Nuclei are at the center of the cell (like where they start out embryologically at 10 weeks) instead of the periphery of the cell where they are normally in a baby.
|
Centronuclear--monotubular myopathy.
|
|
|
|
Pediatric progressive weakness, calf "pseudohypertrophy," Gower sign, joint contractures, kyphoscoliosis, decreased pulmonary function
|

Duchennes/Becker MD
|
|
|
|
Pathology:
1.Fiber size variation: atrophic and hypertrophic fibers, generation and re-generation of fibers, no group atrophy like neurogenic problems 2.Fibrosis of the endomysium 3.Fatty infiltrate |

Duchennes/Becker MD
|
|
|
|
Dystrophin Marker is completely absent on gel.
|

Duchenne's MD
|
|
|
|
Dystrophin marker is a bit heavier, so its not lined up in the right place on the gel.
|
Becker's MD
|
|
|
|
These people have myotonia, facial and distal weakness and wasting, cardiomyopathy, heart block, cataract, gonadal atrophy, diabetes, frontal balding, swallowing difficulties, constipation
|
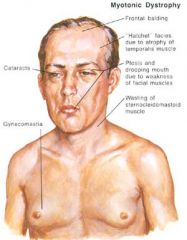
Myotonic Dystrophy
|
|
|
|
Pathology:
1.Increased central nuclei 2.Fiber size variation 3.They resemble other dystrophies in advanced cases 4.Caused by CCTG expansion on chromosome 3 |
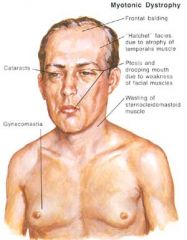
Myotonic Dystrophy
|
|
|
|
-Multi-system disorders due to respiratory chain defects, and have variable phenotypes (even if identical genotypes).
-Generalized weakness, progressive external opthalmoplegia is common. |

Mitochondrial Diseases
|
Ragged Red Fibers!
|
|
|
Pathology:
-Extra redness |

Mitochondrial Disease
|
Ragged Red Fibers!! Have extra mitochondria b/c they are trying to compensate for their inefficiencies.
|
|
|
Mitochondrial Crystal Inclusions
|

Mitochondrial Disease
|
Parking Lot Inclusions
|
|
|
-Cytochrome oxidase deficiency is the most common type of problem is what disease?
-Cytochrome oxidase deficiency causes muscle fibers to become atrophic. |

Mitochondrial Disease
|
Ragged Red Fibers
|
|
|
Pompe's and McArdel's disease are what types of disease?
|
Glycogen Storage Disease.
|
|
|
|
Cause infantile hypotonia, cardiomegaly, hepatomegaly.
|

Pompe's Disease
|
|
|
|
-Cramp's or fatigue, weakness due to excercise.
|

McArdel's Disease
|
|
|
|
Both of these diseases show rise of serum lactate after excercise due to blockage of glycolysis.
|
Pompe's Disease and McArdle's Disease
|
|
|
|
This disease lead to the accumulation of glycogen.
|
Glycogen Storage Diseases: Pompe's and McArdle's
|
|
|
|
What glycogen storage disease is fatal before 2 years?
|

Pompe's Disease
|
|
|
|
-Have a fixed mild myopathy but need to prevent renal failure due to myoglobinuria.
-If given oral sucrose before excercise they do okay. |

McArdel's Disease
|
|
|
|
-Elevated creatine kinase.
-Pathology: 1.Lots of lymphocytes b/c its a cell-mediated immune response against muscle fibers 2.necrotic fibers -Treat with steroids |
Polymyositis
|
|
|
|
-Elevated creatine kinase
-Develop weakness over weeks and months -Have a facial rash -Humoral-mediated microangiopathy with ischemic necrosis of muscle fibers Pathology: 1.Peri-fasicular atrophy 2.Perimysial-perivascular inflammation Tx: responds to corticosteroids |

Dermatomyositis
|
|
|
|
What 2 autoimmune diseases might be peri-neoplastic?
|
Polymyositis, Dermatomyositis
|
|
|
|
Pathology:
1.ring vacuoles in the muscle fibers Tx: Don't respond to corticosteroids (in contrast to polymyositis and dermatomyositis) |
Inclusion Body Myositis
|
|
|
|
Pathology of muscle caused by what virus?
1.necrosis 2.macrophages 3.AZT drug effects |
HIV myopathy
|
|
|
|
What class of bugs have toxins that do local destruction?
|
Clostridium
|
|
|
|
This bug has destructive enzymes/toxins--cellulites, necrosis, gangrene
|
C. perfringens
|
|
|
|
This bug has neurotoxin that blocks the release of GABA in the CNS, causes tetanus.
|
C. tetani
|
|
|
|
This bug has a neurotoxin that blocks the release of ACh at the NMJ as well as autonomic nerve terminals. You get paralysis and autonomic dysfunctions.
|
C. botulinum
|
|
|
|
-Worm that is in a muscle
-Pain, weakness, or asymptomatic--they are at risk for myocarditis and pneumonia |

Trichinosis
|
Curled up T for Trichinosis!
|
|
|
-Pork tapeworm
-Most are asymptomatic and are at risk for CNS infections. |
Cysticercosis
|
Cysticercosis forms cysts in the head.
|
|
|
People with these types of myopathies present with pain, weakness, acute rhabdomyolysis/myoglobinuria
|
Toxic Myopathies
|
|
|
|
Type 2 fiber atrophy is caused by what toxin?
|
Corticosteroid Myopathy
|
|
|
|
Necrosis of muscle is caused by what toxin?
|
Alcoholic Myopathy
|
|
|
|
-Diseae of NMJ
-Symptoms: generalized weakness, weakness of extraocular muscles (ptosis and diplopia) -Pathology: Don't biopsy people with this disease b/c you won't see anything on the slide -Tx: immunosuppressive therapy and remove thyoma if they have one |
Myasthenia Gravis
|
|
|
|
What are the 3 major pathological disease categories of muscle?
|
1.neurogenic
2.myogenic 3.inflammatory |
|
|
|
What are the 4 main histopathologies of nerves?
|
1.Axonopathic
2.Demyelinating 3.Inflammatory 4.Amyloid Neuropathy |
|
|
|
This nerve fascial layer is important b/c it is where we put our sutures in.
|
Epineurium
|
|
|
|
This fascial layer forms the blood-nerve barrier.
|
Perineurium
|
|
|
|
This fascial layer is between nerve axons.
|
Endoneurium
|
|
|
|
-Loss of small axons, endoneurial/pervascular amyloid deposits.
-Pain and temp. sensory abnormalities and autonomic dysfunctions. Associated with cardiac myopathy and renal diseases. |
Amyloid Neuropathy-primary neuropathy
|
|
|
|
-Acute asymmetrical distal weakness rapidly progressing to proximal muscles and sensory signs
-Pathology: Endoneurial mononuclear inflammation mostly in nerve roots and accompanying segmental demyelination and some damage to axons |

Guillian Barre (Acute inflammatory demyelinating polyradiculoneuropathy)
|
|
|
|
-Symmetrical proximal and distal weakness, with sensory abnormalities and hyporelexia evolving around 2 months
-Pathology: Endoneural chronic inflammation, macrophages, segmental demyelination and remyelination, "onion bulb" formation (this formation indicates a myelin formation problem) |

Guillian-Barre (Chronic Inflammatory Demyelinating Polyneuropathy)
|
|
|
|
symmetrical sensorimotor polyneuropathy, pain & parasthesias in the lower limbs and some have autonomic dysfunctions.
-Pathology: nonspecific axonal loss, hyalinization of vessel walls, biopsy is rarely done except to rule out other treatable neuropathies |

Diabetic Neuropathy
|
|
|
|
-Slow progression of symmetrical polyneuropathy, often affecting pain fibers, and tend to affect extremities with lower temperature (like the ear lobes and nose)
-Pathology: 1.Endoneurial and/or epineurial granulomatous inflammation 2.nonspecific segmental demyelination and axonal loss 3.later showing endoneurial fibrosis and thickening perineurial sheaths 4.lipid laden macrophages may be filled with bacteria |

Leprosy
|
|
|
|
-These people present with painful vesicular eruptions and neuropathy involving localized dermatomes in adults or elderly
-Pathology: 1.nonspecific axonal loss 2.neuronal loss in the ganglia |

Varicella-Zoster Virus (shingles)
|
|