Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
22 Cards in this Set
- Front
- Back
|
This artery profuses the areas of the brain that has to do with facial, upper extremities and hands.
A. anterior cerebral a. B. middle cerebral a. C. posterior cerebral a. |
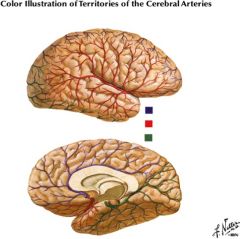
B. middle cerebral a.
(red) |
|
|
This artery profuses the base of temporal lobe and all of the calcarane area.
A. anterior cerebral a. B. middle cerebral a. C. posterior cerebral a. |
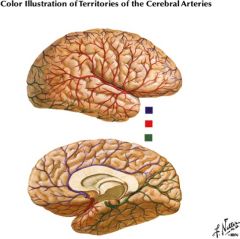
C. posterior cerebral a. (green)
|
|
|
This artery stays on midline, mostly concerned with sensory and motor of the lower extremity.
A. anterior cerebral a. B. middle cerebral a. C. posterior cerebral a. |
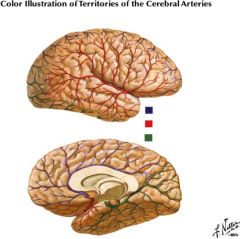
A. anterior cerebral a. (purple)
|
|
|
This branch of the anterior cerebral artery goes into the anterior limb of the internal capsule, head of caudate and portions of orbital frontal gyrus.
A. lateral striates B. medial striates |
B. medial striates
(Lateral striates goes into the internal capsule and basal ganglia.) |
|
|
Infarction here results in the following signs:
- Contralateral face and arm weakness without sensory loss - Behavioral and cognitive abnormalities, including abulia (no motivation), agitation, neglect, and aphasia A. lateral striates B. medial striates |
B. Medial striate artery
The clinical signs reflect involvement of the anterior limb of the internal capsule, rostral basal ganglia (caudate nucleus and putamen), and the basal frontal lobe. |
|
|
Remember, the internal capsule is profused by THREE vascular territories. Name em.
|
Anterior choroid, medial striate of anterior cerebral artery, middle cerebral's lenticular striates.
|
|
|
Anterior choroidal artery goes to the choroid plexus but en route, it also profuses two things. What?
|
hippocampus and the internal capsule's posterior limb!
|
|
|
Occlusion of this artery, a branch of the internal carotid artery, may be asymptomatic or may result in one or more of the following:
- Contralateral motor deficit (hemiplegia) involving the face, arm, and leg due to involvement of the posterior part of the posterior limb of the internal capsule and the cerebral peduncle. This is the most consistent and persistent deficit. - Contralateral hemisensory deficit, usually transient, involving, in most cases, all sensory modalities (hemianesthesia) due to involvement of the sensory tracts within the posterior limb of the internal capsule. - Contralateral visual field defect (hemianopia or quadrantanpoia) due to involvement of the retrolenticular part of the internal capsule (visual radiation) or the lateral genticulate nucleus. This is the most variable feature of the syndrome. |
anterior choroidal artery syndrome
|
|
|
Unilateral occlusion of this artery is associated with the following clinical picture:
- Contralateral hemiplegia or hemiparesis affecting primarily the lower extremity and to a lesser extent the upper extremity - Contralateral sensory deficit affecting primarily the lower extremity and to a lesser extent the upper extremity - Transcortical motor aphasia when the left (dominant) hemisphere is affected (wouldn’t test you on this third one) A. Unilateral anterior cerebral artery syndrome B. Unilateral middle cerebral artery syndrome C. Unilateral posterior cerebral artery syndrome |
A. Unilateral anterior cerebral artery syndrome
Remember, anterior cerebral – stays on midline, mostly concerned with sensory and motor of the lower extremity. |
|
|
This syndrome occurs when both these arteries arise anomalously from a single trunk. In addition to the signs encountered in the unilateral syndrome, the following signs and symptoms occur in the bilateral syndrome due to involvement of orbitofrontal cortex, limbic structures, supplementary motor cortex, and cingulate gyrus:
- Loss of initiative and spontaneity - Profound apathy - Memory and emotional disturbances - Akinetic mutism (complete unresponsiveness with open eyes only) - Disturbance in gait and posture - Grasp reflex - Disorder of sphincter control A. Bilateral anterior cerebral artery syndrome B. Bilateral middle cerebral artery syndrome C. Bilateral posterior cerebral artery syndrome |
A. Bilateral anterior cerebral artery syndrome
Remember, anterior cerebral – stays on midline, mostly concerned with sensory and motor of the lower extremity. |
|
|
This is the most frequently encountered stroke syndrome. The clinical picture varies according to the site of occlusion of the vessel and to the availability of collateral circulation. The conglomerate clinical signs and symptoms of this syndrome consist of:
- Contralateral hemiplegia or hemiparesis (complete or partial paralysis) affecting primarily the face and upper extremity and, to a lesser degree, the lower extremity. Weakness is greatest in the contralateral hand because more proximal limb and trunk muscles as well as facial muscles have greater representation in both hemispheres. - Contralateral sensory deficit, also more prominent in the face and upper extremity than in the lower extremity. Position, vibration, deep touch, two-point discrimination, and stereognosis are more affected than pain and temperature because the latter two sensory modalities may be perceived at the thalamic level. |
Middle cerebral artery syndrome
Remember: middle cerebral – facial, upper extremities, hands |
|
|
Small caliber lenticulostriate arteries, branches of the ______________, supply most of the internal capsule. Typically the lentriculostriate supplies areas that are concerned with motor activity.
A. anterior cerebral artery B. middle cerebral artery C. posterior cerebral artery |
B. middle cerebral artery
|
|
|
Infarction in the territory of the lenticulostriate artery, a branch of the middle cerebral artery, is associated with pure [ motor / sensory ] hemiplegia because of involvement of the internal capsule.
|
motor!!
|
|
|
Unilateral occlusion of this artery is associated with the following:
- Contralateral visual field deficit (hemianopia) - Visual and color agnosia - Contralateral sensory loss of all modalities with concomitant pain (thalamic syndrome) - Pure alexia |
unilateral posterior cerebral artery syndrome.
As a rule, the posterior cerebral artery syndrome is not associated with motor deficit. The hemiplegia reported occasionally in these patients is attributed to involvement of the midbrain by the infarct. |
|
|
This syndrome includes: vascular lesion of dorsolateral medulla involving the spinal tract & nuc. of V, spinal lemniscus (spinothalamics), and nucleus ambiguus (PICA). Typically includes a Horner’s syndrome (slight ptosis).
A. Wallenberg's B. Weber's |
A. Wallenberg’s Syndrome
This is involved spinothalamic tract (thus contralateral loss of pain and temp), nucleus ambiguus (thus difficulty in swallowing and speaking. Laryngeal CN X, Pharyngeal IX), trigeminal spinal tract and nucleus (pain and temperature fibers- ipsilateral from head and neck), and can expand sometimes even to the vestibular nuclei and cerebellar peduncle. Note that pyramids and medial lemniscus are spared. |
|
|
This syndrome involves: Ipsilateral external strabismus (exotropia), ptosis, mydriasis (pupillary dilation) with contralateral spastic hemiplegia (positive Babinski).
|
Weber’s Syndrome (Alternating Oculomotor Hemiplegia) involving crus cerebri of the midbrain (corticospinals and corticobulbars) and oculomotor nerve (branches of PCA)
|
|
|
This is characterized by: Ipsilateral tongue paralysis (tongue deviates to side of lesion) with contralateral hemiplegia. Contralateral loss of conscious proprioception, vibratory sense.
|
Anterior spinal artery. Alternating hypoglossal hemiplegia involving the medullary pyramid (corticospinals) and hypoglossal nerve (anterior spinal artery). Medial lemniscus also involved.
|
|
|
Occlusion of this arterial system usually results in brain stem infarcts. The clinical picture varies according to the specific branch affected and the brain stem territory involved (e.g., lateral medullary syndrome, medial medullary syndrome, Benedikt syndrome, Weber’s syndrome, etc.). Common to all vertebral-basilar artery syndromes are the following:
- Bilateral long tract (motor and sensory) signs - Crossed motor and sensory signs (e.g., facial weakness or numbness combined with contralateral extremity weakness or numbness) - Cerebellar signs - Cranial nerve signs - Alteration in state of consciousness (stupor or coma) - Disconjugate eye movements |
Vertrbral - basilar arteries syndrome
In general, the presence of “the four Ds with crossed findings” suggests a brain stem stroke from vertebrobasilar occlusion. The four Ds are diplopia (double vision) , dysarthria (trouble speaking), dysphagia, and dizziness. |
|
|
In general, the presence of “the four Ds with crossed findings” suggests a brain stem stroke from vertebrobasilar occlusion. The four Ds are ....
|
- diplopia (double vision)
- dysarthria (trouble speaking), - dysphagia - dizziness. |
|
|
Internal carotid lesions are characterized by motor and sensory deficits that are [ bilateral, crossed / contralateral ] whereas veretebrobasilar lesions are characterized by motor and sensory deficits that are [ bilateral, crossed / contralateral ].
|
Internal carotid = contralateral motor and sensory deficits
Vertebrobasilar = bilateral, crossed motor and sensory deficits |
|
|
Internal carotid lesions are characterized by the [ absence / presence ] of aphasias (speech deficits) and [ absence / presence ] of cranial nerve deficits.
|
Aphasia = present
CN defect = absent |
|
|
Verebtrobasilar lesions are characterized by the [ absence / presence ] of aphasias (speech deficits) and [ absence / presence ] of cranial nerve deficits.
|
Aphasia = absent
CN defect = present |