![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
105 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Atypical Parkinsonism |
Poor Response to L Dopa |
Absent Tremor only in 30% |
|
|
Anticoagulation in Pt with Stoke? b -AF c +Recurrence, MI, Vascular (+PAD) d Vascular stent or Prev. MI e +AF
|
a Aspirin or Warfarin b Aspirin 81mg |
|
|
|
Progressive Gait impairment (Lower Body Parkinsonism)+ Urinary incontinence : |
MRI Brain: Expanded Lat & 3rd Ventricle |
Normal Pressure Hydrocephalus |
|
|
Mirgraine Rx and Pregnancy ? |
Paracetol , Ondansteron & Placil are Safe |
Triptans class C |
|
|
Post Concussion & Post Traumatic Stress disorders? |
PTSD : Anxiety disorder Persistent memory about the event Cognitive, Emotional and memory defects + Headaches, Sleep distrub or which occur in Nightmaires, and Accident Remembering |
PCS Symptom Resemble CFS: stress/emotion/alcohol-,anxiety, or depression- Changes in personality- Apathy |
|
|
Stenting indication of ICA stenosis? |
Recurrent Symptoms Evidence of Continuing Ischemia |
|
|
|
Post Stroke mx? whats most important? |
Early rehabilitation |
|
|
|
How to Differntiate btw Malignant Hypert & NMS ? |
NMS a/w ( Haloperidol) or any antipsychotic medication |
NMS: |
|
|
if pt indicated for rtPA be you search for? |
Contraindicatiions
|
|
|
|
Natalizumab JC SE? |
Increased Risk of JC virus inf.: |
نتالي زبة تكول jc مو ماب |
|
|
Dopamin Agonist (Ropinirole) Side Effects ? |
Punding |
Compulsive disorder , doing complex repetitive activities whitout Purposes , Rx by Dec. the dose. ( other behavioral : Internet use , Shopping , Gambling ) |
|
|
Arnold Chiari malformation , which type of Nystagmus? |

Down beat nystagmus +- Syrinx 4 types Headaches aggravated by Valsalva maneuvers, such as yawning, laughing, crying, coughing, sneezing or straining, bending over, or getting up suddenly[26] Tinnitus (ringing in the ears) Lhermitte's sign Vertigo (dizziness) Nausea Nystagmus (irregular eye movements; typically, so-called "downbeat nystagmus") Facial pain Muscle weakness Impaired gag reflex Difficulty swallowing Restless leg syndrome Sleep apnea Sleep disorders[27] Dysphagia (difficulty swallowing)[28] Impaired coordination Severe cases may develop all the symptoms and signs of a bulbar palsy Paralysis due to pressure at the cervico-medullary junction may progress in a so-called "clockwise" fashion, affecting the right arm, then the right leg, then the left leg, and finally the left arm; or the opposite way around. Increased intracranial pressure Pupillary dilation Dysautonomia: tachycardia (rapid heart), syncope (fainting), polydipsia (extreme thirst), chronic fatigue [29] The blockage of cerebrospinal fluid (CSF) flow may also cause a syrinx to form, eventually leading to syringomyelia. Central cord symptoms such as hand weakness, dissociated sensory loss, and, in severe cases, paralysis may occur.[30] |
+- hydrocephalus can occur due to the narrowing at the foramen magnum |
|
|
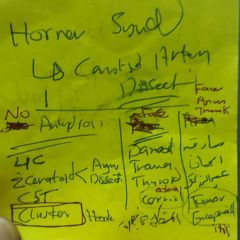
A 72 year old man presents to A and E with a funny turn. he has a history of hypertension. On examination he is found to have grade 3/5 and reduced sensation in his right arm and leg. He is also found to have reduced sensation on the left side of his face and there is evidence of a Horners Syndrome. He is ataxic. Where is the lesion likely to be? |
Lateral Medullary Syndrome |
Brain stem affected |
|
|
Give Example of MAOI? |
Seligiline |
Entecapone : Adjunct |
|
|
Tricks in Parkinson Mx? |
A Ropinirol |
Levodopa SE: |
|
|
Medical Mx of Restless leg syndorme? |
Ropinirole |
رجل مشدودة بحبل |
|
|
spontaneous, continuous lower limb movements that may beassociated with paraesthesia uncontrollable urge to move legs |
Restless leg syndrome |
Rx with Ropinirole |
|

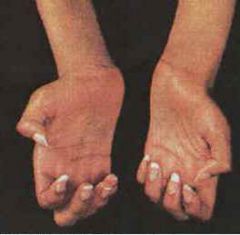
with Axillary and groin freckles |
NF1: Ch 17 ,1 in 4000 mild >> which may be evident at birth and nearly always by the time the child is 10 years old, may include light brown spots on the skin ("cafe-au-lait" spots), two or more growths on the iris of the eye, a tumor on the optic nerve, a larger than normal head circumference, and abnormal development of the spine, a skull bone, or the tibia. |
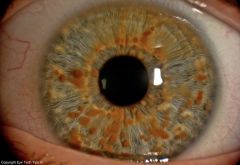
Lisch Nodule |
|
|
Ramsay Hunt Syndrome? |
Vesicular rash of the ear or mouth (as many as 80% of cases) The rash might precede the onset of facial paresis/palsy (involvement of the seventh cranial nerve [CN VII]) Ipsilateral lower motor neuron facial paresis/palsy (CN VII) Vertigo and ipsilateral hearing loss (CN VII) Tinnitus Otalgia Headaches Dysarthria Gait ataxia Fever Cervical adenopathy
|
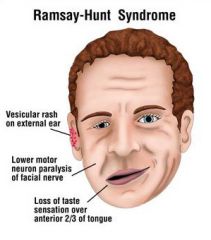
Facial weakness usually reaches maximum severity by 1 week after the onset of symptoms. |
|
|
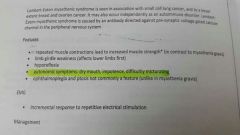
Forgotten Feature in LEMS? |
|
|
|
|
3 Forgotten causes of of Facial Pulsy? |
|
|
|
|
How to dif bw Hunting and AD? |

|
|
|
|
Css of Resless leg syndrome? |

|
|
|
|
Tips of Fredritchs ataxia? |
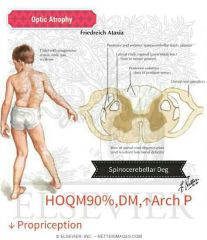
|
|
|
|
Myotonic Dystrophy Tips? |
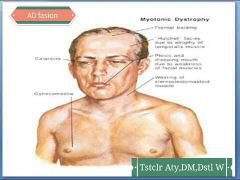
|
|
|
|
??? |

|
|
|
|
PML? CAUSE And Patho? |

|
Natalizumab play a cause to jc |
|
|
Shy Drager R5? |
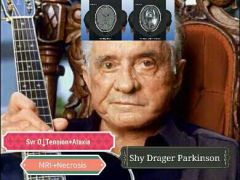
|
|
|
|
???? |

|
|
|
|
TRIAD of IIH? |

|
اتذكر ال ايييجة الي حاطة ايدهة علة راسهة |
|
|
Causes of Dactylitis? |

|
|
|
|
Presentation of Acoustic Neuroma? |
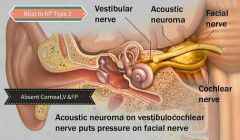
|
|
|
|
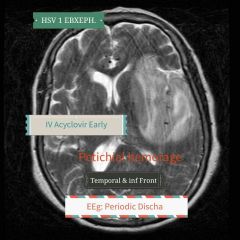
HSV Encephalitis? R5 Not Meningitis |
|
|
|
|
Visual opacities? 6 types |

|
|
|
|
Optic Defect localizing signs? |

|
|
|
|
R5 MERRF? |

|
|
|
|
Site of Huntington Defect? |
|
|
|
|
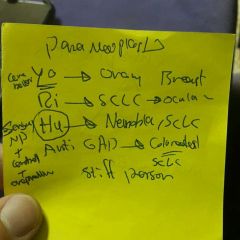
Paraneoplastics Neuro Manifest? |

|
|
|
|
Copper def 3 F and likely cause? |

|
|
|
|
S2 splitting Conditions |

|
Where memory sight in Brain? |
|
|
Allodynia a/w? |

|
|
|
|
Brands of Antidepressants? |

|
|
|
|
Chondrocalcinosis X Ray ¿ |
|
R5 of Tardive dyskinesia? |
|
|
5 As of Alzehiemer D? |

|
|
|
|
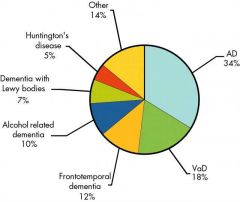
>> of Dementias? |
|
|
|
|
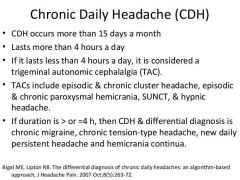
How to diff CDH? |
|
<> 4h |
|
|
Cogn. Imp Drugs? |

|
|
|
|
BISAP? |
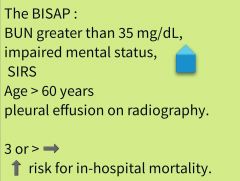
Be sure from net |
|
|
|
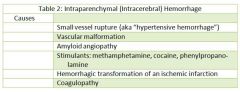
Css of Cerebral Hemorrhage? |
|
|
|
|
Rule of Dexamerhazone in Meningitis? |
Just pneumococcal one 1 dose before ABs And Continue *4 for 4 days |
|
|
|
Primipixole SE? |
→ Sudden Sleep, Hallucination |
|
|
|
When u say this Imfarct is lacunar? |
Small Vessel: < 0.5 mm are the lenticulostriates, the brainstem penetrating and the thalamogeniculate.
|
|
|
|
Common Css, of ICH acc to Age? |
< 45 y: Drug Abuse ( Cocaine and amphetamin) and AV Malformation >55 y HT and amyloid Angiopathy |
Excessive Alcohol Also |
|
|
2 presentation of Berry Aneurysm? |
1 Sever Headache 2 CN 3 Pulsy with ipsilateral Pupillary dilatation and ? |
Xanthocromia: conversion of Hemoglobin to Billirubin |
|
|
Notes on Drugs |
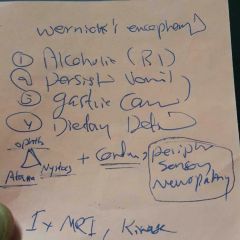
Drugs Cause Perph. Neurop: NM VIA TCA Amiodarone→للدوة الوحيد الي يسوي → Demylination Triptans→ لاتنطي حتة لو rf لل ischemia وينطه at onset of Headache مو Aura
Amytriptyline: امي تبتليني البولة محصورة مالتهة
Citalopram يطير الشهوة عليك بس ما يخصيك عكس ال opiates
بالبال بالخاطر ال buscopan كونترا انديكيتد بال MS؟؟؟ |
|
|
|
4 components of Stroke? |
Aphasia (Language not muscle) Weakness Numbness Ophthalmic |
|
|
|
You cant say Apraxia in? You cant say snsory or cerebellar in? |
Motor abn Unconsiousness (Motor may be preserved : respond to pain) |
|
|
|
>> pres in Conversion disorder? |
Blindness |
|
|
|
Old age + dysphagia 1st slowly to solids then rapid liquids with Depression or Postural Inst? |
Parkinson |
|
|
|
Mycosis Fungoides? |
|
Albert Bazin $ |
|
|
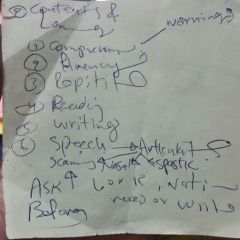
Contents of Language? |
|
|
|
Forgotten C? Cluster of Horns 2 TT? |
|
|
|
|
Pentad of Wernick's En. ? 2 of 4 Causes? |
|
|
|
|
Neuro Paraneoplastic Abs? |
|
|
|
|
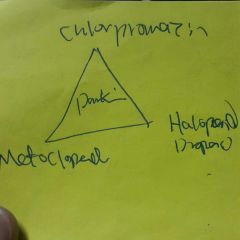
3 Drugs © Parkinson? |
|
|
|
|
EMG changes in MND? يعني هي العضلة مابيهة شي بس صوجة هو ماعندة طاقة |
↓AP ↑Amplitude |
|
|
|
What diff Apoplexy from SAH? 3 |
Hypotention Hypothyroid Extraocular Pulsy |
|
|
|
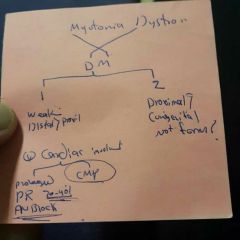
Myo Dystrophy Classification? Cardiac involvement ? |
|
|
|
|
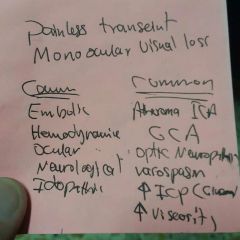
Amaurosis Fugax? © |
|
|
|
|
NPH 2° to ? |
Head Injury SAH Meningitis |
Reversible Rx by Shunt |
|
|
Exam of Encephalopathy? |

|
|
|
|
Neurological Complication inRenal disease? |
|
|
|
|
Trouble With:Speech control—volume, pitch, articulationWriting and typingOver- or under- sensitivity to light, touch, space, taste, or smells |
Dyspraxia Seen in Stage 2 HE |
Personal grooming and other self-help activitiesCooking or other household choresDrivingClumsiness |
|
|
>> inherited Neurological Disorder? |
CMT the initial symptom is foot drop the it may go to Hands, eye SC and others Motor and Sensory (Pain Preserved) with Hammer Toe No Available Rx |
|
|
|
Charcot Joint? or
|
|

|
|
|
Tabes dorsalis? |
syphilitic myelopathy (Dorsal Colomn) |
|
|
|
Todd Paralysis |
Weakness in Upper limb contra lateral to the Side of Seizure |
|
|
|
>> cause of temporal lobe epilepsy? |
Mesial Temporal Seclerosis (Hippocambus) |
|
|
|
Pelvic Thrusting >> seen in ? |
Frontal Lobe Epilepsy also: <30s absent Post Ictal Sexual Automatism Eye Deviation CL to the Seizure site Vocalization (very common) Contiousness more Preserved HemiClonic (CL Face arm and leg seizures) Jacksonian F Fencing Posture(Flexing the ipsi and relaxing the CL with DEviation of face and Eye to CL) |
|
|
|
Pain located on the front of the thigh and shin, further radiates towards the inner ankle, sometimes the medial toe |
L4 radiculopathy |
Occasionally, failure of the quadriceps muscle and reflex weakness |
|
|
Sensory loss posterolateral aspect of leg and lateral aspect of foot Weakness in plantar flexion of foot Reduced ankle reflex -n-->"} |
L5 radiculopathy Pain radiates to the side of the thigh and lower leg towards the back of the foot and toes 1-3 All reflexes are preserved |
|
|
|
S1 radiculopathy? |
Pain radiates to the posterior side of the thigh and lower leg to the ankle side, sometimes on up to the fourth toeGluteal muscles are weakenedDifficulty standing on toes |
|
|
|
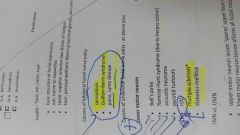
Causes of 3rd CNP? |
Causes • diabetes mellitus • vasculitis e.g. temporal arteritis, SLE
• false localizing sign* due to uncal herniation through tentorium if raised ICP • posterior communicating artery aneurysm (pupil dilated+Sever Headache) • cavernous sinus thrombosis • Weber's syndrome: ipsilateral third nerve palsy with contralateral hemiplegia -caused by midbrain strokes • Berry Aneurysms
• other possible causes: amyloid, multiple sclerosis |
|
|
|
DDX of Peripheral or Ring Enhaced lesion? MAGIC DR |
|
MAGIC DR: M: metastasis A: abscess G: glioblastoma multiforme I: infarct (subacute phase) C: contusion D: demyelinating disease R: radiation necrosis or resolving haematoma |
|
|
C5 radiculopathy? |
Pain is found along the lateral brachium of the affected side of the arm. C5 innervated muscle weakness may be found i.e rhomboids, deltoid etc. |
|
|
|
C6 radiculopathy? |
Pain is found along the lateral antebrachium of the affected arm C6 innervated muscles are weak i.e forearm pronator and supinators, wrist extensors etc. |
|
|
|
C7 radiculopathy? |
Pain is found along the middle finger of the affected armC7 innervated muscle weakness is found i.e wrist flexors, finger extensors etc. |
|
|
|
contralateralhemiparesis and sensory loss, lower extremity > upper · disconnection syndrome (Conducting Aphasia) |
Anterior cerebral artery · |
|
|
|
· contralateral hemiparesis and sensory loss, upper extremity > lower · contralateral hemianopia · aphasia (Wernicke's) · gaze abnormalities |
Middle cerebral artery |
|
|
|
· contralateral hemianopia with macular sparing · disconnection syndrome |
Posterior cerebral artery |
|
|
|
· present with either isolated hemiparesis, hemisensory loss or hemiparesis with limb ataxia |
Lacunar |
|
|
|
· ipsilateral: ataxia, nystagmus, dysphagia, facial numbness, cranial nerve palsy · contralateral: limb sensory loss |
Lateral medulla (posterior inferior cerebellar artery) |
|
|
|
· VI nerve: horizontal gaze palsy · VII nerve · contralateral hemiparesis |
Pontine |
|
|
|
· sensory inattention · apraxias · astereognosis(tactile agnosia) · inferior homonymous quadrantanopia · alexia, acalculia, finger agnosia and right-left disorientation |
Parietal lobe lesions |
Gerstmann's syndrome (lesion of dominant parietal): alexia, acalculia, finger agnosia and right-left disorientation |
|
|
· homonymous hemianopia (with macula sparing) · cortical blindness · visual agnosia |
Occipital lobe lesions |
|
|
|
· Wernicke's aphasia · superior homonymous quadrantanopia · auditory agnosia · prosop-agnosia (difficulty recognising faces) |
Temporal lobe lesion |
|
|
|
· expressive (Broca's) aphasia · disinhibition (perceptual(hypersexuality, hyperphagia), Motor, and Cognitive) also in TBI · perseveration ( Difficulty in Switching between ideas or Orders) most Commonly in TBI · anosmia · inability to generate a list |
Frontal lobes lesions |
(Broca's) aphasia: located on the posterior aspect of the frontal lobe, in the inferior frontal gyrus |
|
|
· midline lesions: gait and truncal ataxia · hemisphere lesions: intention tremor, past pointing, dysdiadokinesis, nystagmus |
Cerebellum lesions |
|
|
|
· lefthomonymous hemianopia means? |
visual field defect to the left Lesion of right optic tract |
|
|
|
· incongruous defects; |
= optic tract lesion |
|
|
|
congruous defects = |
optic radiation lesion or occipital cortex |
|
|
|
what means congrous and in congrous? |
A congruous defect simply means complete or symmetrical visual field loss and conversely an incongruous defect is incomplete or asymmetric. |
|
|
|
Homonymous hemianopia Presentations? 3 |
· incongruous defects: lesion of optic tract · congruous defects: lesion of optic radiation or occipital cortex · macula sparing: lesion of occipital cortex |
|
|
|
macula sparing? |
: lesion of occipital cortex |
|
|
|
Bitemporal hemianopia |
· lesion of optic chiasm · upper quadrant defect > lower quadrant defect = inferior chiasmal compression, commonly a pituitary tumour · lower quadrant defect > upper quadrant defect = superior chiasmal compression, commonly a craniopharyngioma |
|