Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
15 Cards in this Set
- Front
- Back

|
Cholesteoma granuloma
-most commonly occur within the petrous apex but occasionally arise in the mastoid segment, middle ear, and orbitofrontal region - smooth, well-defined, homogeneous masses that display high signal intensity at T1-weighted imaging -high T1 signal of these lesions is unaffected by fat suppression techniques -Cholesterol granulomas are also often hyperintense at T2-weighted imaging and may display a hypointense rim secondary to hemosiderin deposition |
|
|
Cockayne syndrome
-autosomal recessive defect in DNA repair that is characterized clinically by premature aging, encephalopathy, microcephaly, deafness, and photosensitivity -cerebral atrophy, white matter hypomyelination, and extensive calcifications within but not limited to the bilateral lentiform and dentate nuclei -MR spectra show the presence of lactate and decreased levels of choline and N-acetylaspartate -calcifications may exhibit high signal intensity at T1-weighted imaging and low signal intensity at T2-weighted imaging |
|
|
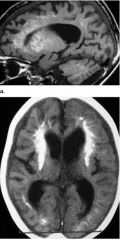
Cortical Laminar necrosis
-sequela of a global hypoxic ischemic event or, less commonly, an effect of immunosuppressive therapy or chemotherapy -third layer of the cortex is particularly susceptible to depletion of oxygen and glucose -: High-signal intensity cortical lesions appear on T1-weighted images about 2 weeks after the inciting event and become increasingly conspicuous at 1–2 months after the event, along with maximum contrast enhancement -T1 signal hyperintensity usually fades after 2 years, whereas parenchymal atrophy progresses |
|
|
Craniopharyngioma
-benign neoplasms derived from epithelial rests in the Rathke pouch -tend to be solid and occur in adults, whereas the adamantinomatous variety tends to be cystic and occurs in children -most craniopharyngiomas are located in the suprasellar region, about half demonstrate an intrasellar component as well -d 90% of craniopharyngiomas contain calcifications that are visible at CT and cystic components that sometimes show signal hyperintensity on T1-weighted images -cystic portions of craniopharyngiomas also frequently display T2 hyperintensity and rimlike enhancement on contrastenhanced T1-weighted images |
|

|
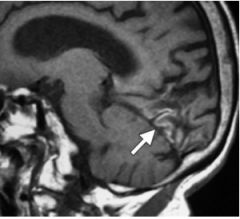
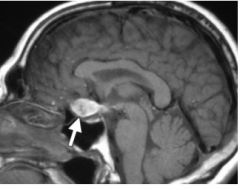
ECTOPIC POSTERIOR PITUITARY
-rare congenital malformation of the hypothalamus that is associated with hypoplasia or absence of the pituitary stalk and resultant dwarfism due to growth hormone deficiency -ectopic posterior pituitary lobe is most commonly located along the median eminence in the floor of the third ventricle -ectopic posterior pituitary gland also might result from traumatic or surgical transection of the pituitary stalk -Signal hyperintensity in the posterior aspect of the pituitary gland on T1-weighted images is related to the paramagnetic effect of the vasopressin–neurophysin II–copeptin complex |
|
|
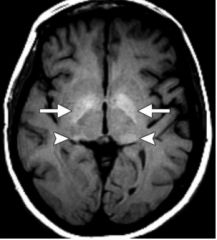
Hepatic encephalopathy
-bilateral regions of signal hyperintensity in the lentiform nucleus and substantia nigra on T1-weighted images -related to the accumulation of manganese in patients with hepatic encephalopathy and may be encountered also in welders and recipients of hyperalimentation therapy -focal areas of signal hyperintensity in subcortical white matter on T2-weighted images, and elevated glutamine and glutamate levels at MR spectroscopy that are probably related to ammonia toxicity -potentially reversible with liver transplantation |
|
|
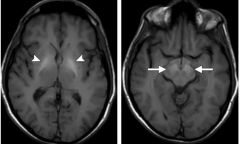
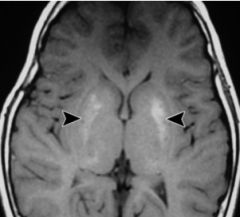
NEUROFIBROMATOSIS TYPE 1
-autosomal dominant disorder of the neurofibromin gene on chromosome 17 -wide variety of intracranial manifestations, including hypothalamic–optic nerve and brainstem pilocytic astrocytomas; neurofibromas; neurofibrosarcomas; plexiform neurofibromas; hydrocephalus; arachnoid cysts; cerebrovascular occlusions; nontumorous highsignal-intensity foci or unidentified bright objects that occur predominantly in the basal ganglia and posterior fossa on T2-weighted images; and highsignal-intensity lesions, distinct from unidentified bright objects, that most commonly appear in the basal ganglia on T1-weighted images -T1-hyperintense basal ganglia lesions occur in approximately 20% of patients with type 1 neurofibromatosis (57,58) and predominantly involve the globus pallidus and internal capsules bilaterally and symmetrically -basal ganglia lesions in type 1 neurofibromatosis do not exhibit mass effect, surrounding edema, or enhancement. |
|
|
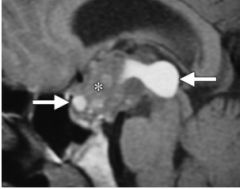
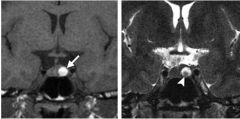
RATHKE CLEFT CYST
-occasionally cause headaches, visual disturbances, and diabetes insipidus -half of Rathke cleft cysts show hyperintense signal at T1-weighted imaging -hyperintense at T2-weighted imaging -Small intracystic nodules with high signal intensity at T1-weighted imaging and low signal intensity at T2-weighted imaging are present in approximately 45% of cases -presence of peripheral enhancement and an increased risk of recurrence after surgical resection |
|
|
WILSON DISEASE
-rare autosomal recessive condition caused by mutations in the ATP7B gene with resultant abnormal copper metabolism and accumulation -Patients may present with dysarthria, dystonia, tremor, choreoathetosis, liver failure, and classic Kayser-Fleischer rings at ophthalmologic examination -most commonly found in the bilateral basal ganglia and ventrolateral thalami -Regression of the signal abnormality at T1-weighted MR imaging correlates with response to treatment -Involvement of the striatum at MR imaging manifests with pseudoparkinsonian signs, dentatothalamic tract involvement manifests with cerebellar signs, pontocerebellar tract involvement correlates with pseudoparkinsonian signs, and globus pallidus involvment is associated with portosystemic shunting secondary to cirrhosis |
|

|
AMYLOID ANGIOPATHY
-disorder of b-amyloid deposition in cortical, subcortical, and leptomeningeal vessels -responsible for only about 2% of all intracranial hemorrhages, it is relatively common among the elderly -petechial microhemorrhages or macrohemorrhages with irregular borders in a lobar distribution in cortical and subcortical regions are characteristic findings of amyloid angiopathy -Intraparenchymal hemorrhages at various stages of evolution, as well as subarachnoid, subdural, and intraventricular hemorrhages, may be seen at imaging |
|

|
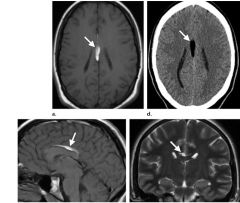
CEREBRAL VENOUS THROMBOSIS
-most commonly manifests with a headache -computed tomography (CT) is the presence of a hyperattenuating clot, although this feature is apparent in only about 20% of cases -e “empty delta” sign, a filling defect at contrast-enhanced CT or CT venography, is present in less than 30% of cases -subacute thrombus often has high signal intensity on T1-weighted images, signal intensity on T2 weighted images is more variable but is also usually high -MR venography is effective for depicting the extent of venous occlusion and collateral vessel formation |
|

|
CEREBRAL VENOUS THROMBOSIS
|
|

|
COLLOID CYST
-headache is the most common clinical manifestation in symptomatic patients -atonic seizures, nausea, vomiting, diplopia, transient loss of consciousness, and (rarely) sudden death -About two-thirds of colloid cysts show high signal intensity at T1-weighted MR imaging, and most exhibit low signal intensity at T2-weighted imaging -Colloid cysts that show low signal intensity at T1-weighted imaging and high signal intensity at T2-weighted imaging have a tendency to enlarge rapidly |
|
|
PERICALLOSAL LIPOMA
- |
|
|
RUPTURED DERMOID CYST
-rare complication that can cause severe chemical meningitis and sensory or motor hemisyndrome -dermoid cysts typically show high signal intensity on T1-weighted images, variable signal intensity on T2-weighted images, and lack of enhancement on contrast-enhanced images -MR spectroscopy discloses mobile lipid peaks at 0.9 and 1.3 ppm -e lesions are usually well-defined, nonenhancing masses with fat attenuation at CT |