Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
|
What clinical issues arise from lesions to the basal ganglia?
|
Abnormal voluntary movements
|
|
|
What makes up the Basal Ganglia?
|
6 masses of grey matter:
- caudate, putamen, globus pallidus (GP), subthalamus (Sub) - substantia nigra (SN), pedunculopontine tegmental nucleus (PpT) |
|
|
What separates the caudate from the putamen?
|
The internal capsule
|
|
|
What are the afferent and efferent connections to the caudate and putamen?
|
afferents: cortex, SNc
efferents: GP |
|
|
What are the afferent and efferent connections to the globus pallidus?
|
afferents: CPu, Sub
efferents: thalamus, PpT, Sub |
|
|
What cell types are in the caudate and putamen?
|
Spiny cels (projection cells)
- GABA-SP (substance P) - GABA-Enk (Enkephalin) Aspiny cells (interneurones) - GABA - ACh |
|
|
What cell type is in the globus pallidus?
|
GABA
|
|
|
What are the afferent and efferent connections to the subthalamus?
|
Afferent and efferent: GP
|
|
|
What cell types are in the subthalamus?
|
Glutamate
|
|
|
What cell types are in the substantia nigra?
|
SNr (pars reticulata) - GABA
SNc (pars compacta) - Dopamine |
|
|
What are the afferent and efferent connections of the substantia nigra?
|
SNr
- afferents: CPu, Sub - efferents: thalamus, PpT, Sub SNc: - afferents: cortex - efferents: CPu |
|
|
What cell types are in the pedunculopontine area?
|
Ach, Glu
|
|
|
What are the afferent and efferent connections of the pedunculopontine area?
|
Afferents: GP
efferents: SpC |
|
|
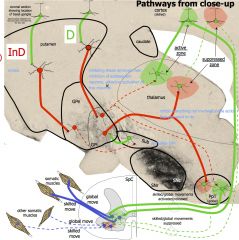
What is the DIRECT pathway?
|
|
|
|
What is the INDIRECT pathway?
|
|
|
|
What function does the SNc (substantia nigra pars compacta) have on the direct and indirect pathways?
|
|
|
|
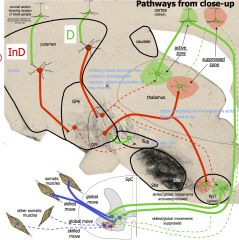
What effect does Parkinson Disease have on the SNc?
|
SNc gets switched off
DIRECT pathway: - Inhibition from CPu to GPi stopped - Inhibition to thalamus and PpT increases - Stimulation of cortex (skilled)/ PpT (global)/SC/motor decreased INDIRECT pathway: - Inhibition from CPu to GPe increased - Inhibition from GPe to subthalamus decreased - Subthalamus goes off tap stimulating GPi all the time - GPi inhibits the thalamus and PpT all the time - Skilled (cortex) and global (PpT) movements suppressed |
|
|
What are 9 key signs in Parkinson disease?
|
1. lead-pipe rigidity* (hypertonia)
2. akinesia* (no spontaneous movements) 3. bradykinesia* (slow walking) 4. expressionless face 5. shuffling gait 6. cog-wheel rigidity 7. flexed posture (reflex) 8. speech 9. micrographia |
|
|
Which parts of the brain are involved in the tremor and postural/gait aspects of Parkinson Disease?
|
Tremor - thalamus
Posture/gait - PpT |
|
|
What drugs are first line treatment for Parkinson Disease?
|
- Levodopa (converted to dopamine)
- Da agonist (eg bromocriptine) - MaOI (monoamine oxidase inhibitors - eg selegiline, COM-T inhibitors) |
|
|
What are the aims of surgical/deep brain stimulation treatments for Parkinson Disease?
|
Disrupt the abnormal circuit
Target Subthalamus, thalamus, GP |
|
|
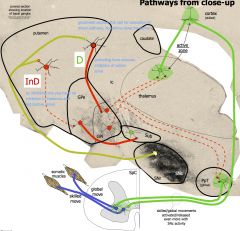
What is the cellular pathology associated with chorea?
|
Decreased GABA-Enk cells (genetic mutation)
--> decreased CPu volume - leads to decreased Indirect pathway |
|
|
What is the blood supply of the cerebellum?
|
PICA (Posterior inferior cerebellar artery)
AICA (Anterior inferior cerebellar artery) SCA (Superior cerebellar artery) |
|
|
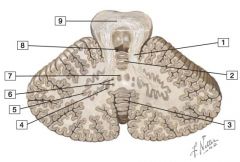
1. Superior cerebellar peduncle
2. Lingula 3. Vermis 4. Emboliform nucleus 5. Dentate nucleus 6. Globose nucleus 7. Fastigial nucleus 8. Fourth ventricle 9. Decussation of the superior cerebellar peduncles Comment: The cerebellum helps to smooth and coordinate movements as its most conspicuous function, and it also coordinates neural activities associated with nonmotor functions. |
|
|
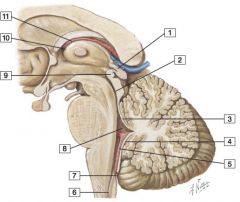
1. Habenular commissure
2. Cerebral aqueduct 3. Superior medullary velum 4. Inferior medullary velum 5. Choroid plexus of fourth ventricle 6. Central canal of spinal cord 7. Median aperture (foramen of Magendie) 8. Fourth ventricle 9. Posterior commissure 10. Interventricular foramen of Monro 11. Choroid plexus of third ventricle |
|
|
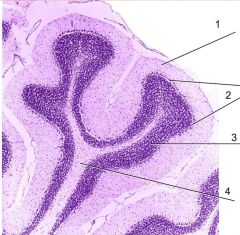
Cerebellum
1. Molecular layer 2. Purkinje layer 3. Granule layer 4. White matter of folium |
|

|
Flocculus
|
|
|
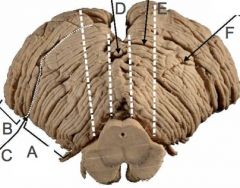
A. Anterior Lobe
B. Posterior lobe C. Primary fissure D. Vermis E. Paravermis F. Lateral hemisphere |
|
|
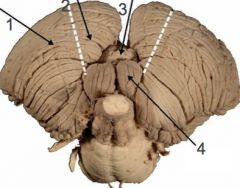
1. Lateral hemisphere
2. Paravermis 3. Vermis 4. Tonsil |
|
|
What information does the spinocerebellum (vermis and paravermis) receive?
|
the vermis receives information from the trunk and controls the trunk muscles whereas the paravermal region receives information from the limbs and controls limb muscles
|
|
|
Locate the lesion:
Unsteadiness, swaying, falling. Tendency to fall backwards when walking. Spontaneous nystagmus. Signs are usually bilateral. |
Vestibulocerebellum (Archicerebellum)
|
|
|
Locate the lesion:
loss of muscle tone and fatigue, asynergia, dysmetria (hypermetria, pastpointing), intention tremor, dysdiadochokinesia (inability to perform rapid successive movements), nystagmus, speech disturbances (slurred speech, separating of syllables). |
Cerebrocerebellum (Neocerebellum)
|
|
|
Which lesions can typically produce four types of disturbances:
i) delays in initiating and terminating movement, ii) intention tremor at the end of the movement, iii) disorders in the temporal coordination of movements involving multiple joints, and iv) disorders in the spatial coordination of hand and finger muscles. |
Cerebrocerebellar
|
|
|
What do the putamen and GPe and GPi form?
|
The lentiform nucleus
|
|
|
Which part of the substantia nigra makes it appear black?
|
SNc (pars compacta)
|
|
|
Functionally the basal ganglia can be divided into input nuclei, output nuclei and intrinsic nuclei. Which nuclei are in each group?
|
Input: Caudate and putamen (striatum)
Output: GPi and SNr Intrinsic: GPe, subthalamic nucleus and SNc |
|
|
What is the disorder:
Rapid involuntary movements of the face, tongue and limbs. It is associated with neuronal degeneration of the striatum, especially the caudate and to a lesser extent the cerebral cortex. Dementia appears in the later stages. It is due to an autosomal dominant gene. |
Huntington't Chorea
|
|
|
What is the disorder:
"Continuous, violent, coordinated involuntary activity involving the axial and proximal appendicular musculature such that the limbs are flung about". Ballistic movements are large, proximal, rotatory throwing or kicking movements. The violence of the movements may injure skin, tissues, and joints and, if severe, bones. The ceaseless vigorous activity of hemiballismus may result in malnutrition and emaciation in untreated individuals. The movements, although sometimes briefly suppressed volitionally, are usually continuous during the waking hours and are enhanced by voluntary movement of the involved limb, stress, and anxiety. The movements are reduced or absent during sleep |
Hemiballismus
|
|
|
What is the disorder:
Involuntary slow writhing movements of the hands and fingers, seems to involve damage to the striatum. |
Athetosis
|
|
|
What is the gold standard of pharmacological treatment for Parkinson Disease?
|
Levodopa/ Carbidopa
(Levodopa converted to dopamine, Carbidopa inhibits the peripheral conversion of levodopa to dopamine and the decarboxylation of oxitriptan to serotonin by aromatic L-amino acid decarboxylase. This results in increased amount of levodopa and oxitriptan available for transport to the CNS) |