Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
21 Cards in this Set
- Front
- Back
|
As your intracranial pressure increases, what are the 3 things that can happen (state in order!)
|
1. CSF decreases first (compressing ventricles)
2. blood flow goes down (ischemia) 3. herniation of CNS tissue (brain itself shifts from one compartment to another) |
|
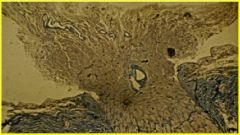
what's the pathology here? how does this show up in a patient and what could be causing this?
|
you're seeing the optic nerve disc being squeezed out by excessive pressure intracranially.
this presents as papilledema and anything from a hemorrhage to a tumor in the intracranial vault could be causing this. |
|
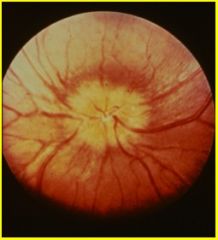
what is the pathology here? what does this tell you?
|
papilledema. nerve head is bulging up out at you. tells you that the pt has increased intracranial pressure
|
|
|
are faster or slower expansion of masses within the brain better? explain.
|
slower. a faster expanding lesion could be very lethal as the progression to more life threatening stages (ie. loss of medullary fxn) would be much faster. a slow growing tumor would have more time to deal with medically
|
|
|
which type of herniation forces tissue to go beneath the falx cerebri? what is the clinical result of this type of herniation?
|
subfalcine herniation (aka. cingulate gyrus herniation)
pt will experience UMN weakness in legs contra to lesion (but ipsi to the growing lesion). also sensory may be affected as well as urinary incontinence |
|
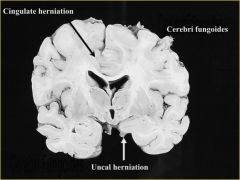
what is cerebri fungoides?
what is an uncal herniation and what does it cause clinically? |
cerebri fungoides - if there's a skull defect, the brain may herniate up and out like a mushroom
uncal herniation - uncal lobe herniates across infratentorium and squashes midbrain, compressing CN 3 (this leads to ipsilateral pupillary dilation - blown pupil - and paresis of extra-ocular muscles that are controlled by CN 3) |
|
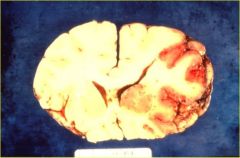
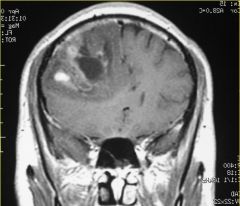
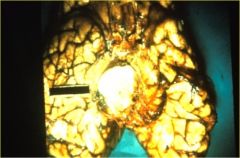
what pathology is imaged here? what is this caused by?
|
Coronal section of cerebral hemisphere with cingulate herniation. Caused by stroke of middle cerebral artery. See ventricular compression.
|
|
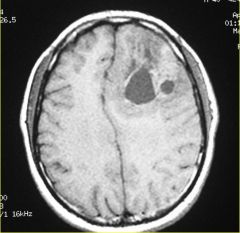
what pathology is shown here?
|
axial CT of cingulate herniation
|
|
what pathology is shown here? which artery is at risk because of this type of herniation? what would pt feel like?
|
coronal section of subfalcine herniation (cingulate herniation). The sulci and ventricle on the left side of picture are absent
anterior cerebral artery pt would be confused and drowsy with UMN weakness in lower body contra to herniation and ipsi to lesion |
|
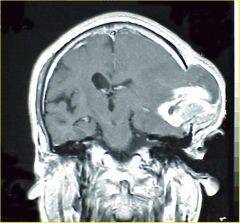
what pathology is shown here?
|
cerebral fungoides.
see compression of ventricles and no sulci on ipsi side -- intracranial pressure is higher on the left side of pts head |
|
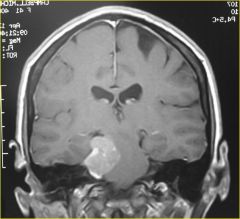
name this herniation. what would the patient present as clinically?
|
right sided mass with uncal herniation. pt would have a compressed CN 3 that presents as a right blown/dilated pupil (that could not constrict with light) and right looking laterally due to unopposed lateral rectus muscle pulling on the right eye (down and out)
|
|
|
what is a duret hemorrhage?
|
when an uncal herniation continues to herniate and distorts the midbrain stem, leading to a hemorrhage that's NON-REVERSIBLE!!
|
|
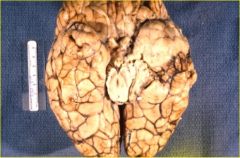
what pathology is shown here?
|
uncal herniation on right side of picture. pt would get ipsi CN3 deficit
|
|
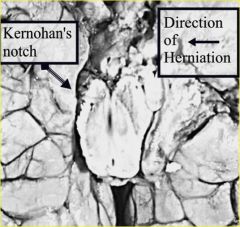
what pathology is imaged here? what would it show up as clinically?
|
KERNOHAN'S NOTCH!!
Right side (of picture) abnormal Temporal lobe tumor. CN3 on right (of picutre) is messed up. Mickey mouse brain stem is elongated- it’s being squished and shifted. The peduncle on the other side will be squished, carrying CST and CBT fibers resulting in contra UMN weakness (contra to the notch; ipsi to the mass!!). |
|
think about this image...what would happen?
|
Look for a blown pupil. If you have kernohan’s notch, then you have UMN weakness contra to the notch, ipsi to the mass.
|
|
|
what is the order of motor tone changes during neurological deterioration (this could happen if induced pharmacologically with anesthesia) - this is the progressive "turning off" of fxn progressing from rostral to caudal
|
1. decorticate = arms flexed, legs extended (structures above red nucleus not working)
2. decerebrate = arms extended, legs extended (structures bw red nucleus and vestibular nucleus not working) 3. flaccid= loss of muscle tone overall; You’re approaching brain death. note: When a pt is undergoing anesthesia, they go from delirium to stupor and then assume decorticate, then decerebrate posture, then flaccid…as they recover, they go back from flaccid to decerebrate and then to decorticate posture and then back to alert. |
|

what is shown here and how did it happen? what is the worse thing that could happen?
|
tonsillar herniation. with enough increase in ICP, the medulla and cerebellum both will try to get through the only hole in the skull (foramen magnum). the worse thing that could happen is the medullary fxn being distorted and comprimisting respiratory control. you also meet criteria for brain death due to lack of brainstem fxn.
|
|

what is this?
|
duret hemorrhage = midline brain stem hemorrhage caused by uncal herniation
|
|
|
what's the overall order of a brain mass leading to brain death?
|
Mass one side --> cingular herniation --> uncal herniation --> ipsi CN3 compression (blown pupil) --> potential contra kernohan’s nothch --> cerebellar tonsillar herniation --> brainstem compression --> brain death
|
|
|
what' sthe only circumstance to do an lumbar puncture with increased ICP (bc otherwise you NEVER perform it, risking imminent danger)?
|
when pt has meningitis
|
|

what is this? define non-communicating vs. communicating hydrocephalus?
|
hydrocephalus.
non-communicating = compromise in CSF flow due to blockage within the ventricar system itself and casuing only hte ventricles prior to blockage to dilate (ie. blockage of the aqueduct of Sylvius) communicating = blockage at the arachnoid granulations, causing ALL the ventricles to dilate |