![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
394 Cards in this Set
- Front
- Back
|
Maternal medical conditions |
Maternal medical conditions |
|
|
Fetal mortality and morbidity are increased with |
maternal insulin-dependent diabetes (type 1), mainly from congenital malformationsand intrauterine death |
|
|
how do you decrease congenital malformations and intrauterine death in type 1 diabetic mothers |
good diabetic control this requires a multidisciplinary management and close prenatal surveillance |
|
|
what are the fetal problems associated with maternal diabetes |
congenital malformations macrosomia IUGR Polyhydramnios Preterm labor Intrauterine death |
|
|
the risk of congenital malformations is 6% for a diabetic mother this is how much greater than normal babies from non diabetic mothers |
4 times normal specific increased risk of cardiac malformations and caudal regression syndrome (sacral agenesis) |
|
|
macrosomia is due to |
maternal hyperglycemia resulting in fetal hyperinsulinemia, which promotes growth |
|
|
what % of diabetic mothers have macrosomic babies compared to non diabetic mothers |
25% diabetic mothers have macrosomic babies versus 8% of infants of non diabetic mothers. |
|
|
Macrosomia predisposes to |
cephalopelvic disproportion andincreased risk of delivery-related complications, both to the mother(cesarean section and forceps delivery) and the fetus; includingbirth injuries. |
|
|
diabetic mothers have an increased risk of intrauterine growth restriction, how much |
3 fold increase usually associated with maternal vascular disease |
|
|
diabetic mothers have a 10% risk of preterm labour |
true |
|
|
intrauterine death in diabetic mothers typically occurs |
suddenly in third trimester Less commonwith good diabetic control and induction at 38 weeks. |
|
|
what neonatal complications do diabetic mothers get |
malformations and birth injuries hypoglycemia polycythemia hyperbilirubinemia respiratory distress syndrome hypertrophic cardiomyopathy renal vein thrombosis |
|
|
features of type 2 diabetes and gestational diabetes in pregnancy |
associated with perinatal coplications glucose intolerance from gestational diabetes complicates 1-2% of pregs and may require dietary or insulin treatment may cause neonatal macrosomia, hypoglycemia and polycythemia |
|
|
maternal medical conditions in pregnancy - broad groups |
diabetes mellitus type 1 type 2 diabetes and gestational diabetes maternal red blood cell alloimmunization - rhesus hemolytic disease - maternal antibodies to fetal red blood cell antigens - other maternal antibody conditions to fetal red blood cell antigens - anti-Kell and anti-c perinatal alloimmune thrombocytopenia - analogus to rhesus hemolytic disease but maternal antibodies to fetal platelets instead others maternal hyperthyroidism maternal hypothyroidism autoimmune thrombocytopenic purpura |
|
|
define fetal hydrops aka hydrops fetalis |
fluid accumulation in at least 2 fetal fluid compartments e.g. ascites and pleural or pericardial effusion |
|
|
what sort of presentation would you have with rhesus hemolytic disease |
antibodies found at antenatal screens previous pregnancy affected with hemolytic disease fetal hydrops on ultrasound detection of fetal anemia using ultrasound (middle cerebral artery blood flow increased for gestational age) Maternal polyhydramnios. Infant – jaundice, anemia, hydrops, hepatosplenomegaly. |
|
|
how rhesus hemolytic disease managed prenatally |
refer to specialist center if needed - due to increasing antibody levels on maternal blood screen fetal rhesus genotyping can be done non invasively through free fetal DNA detection in maternal plasma monitor with serial ultrasound for fetal anemia and signs of hydrops doppler blood flow - checking for fetal anemia measure fetal hematocrit (from cordocentesis) intrauterine blood transfusion deliver preterm if necessary |
|
|
how do you monitor fetal anemia |
usually by middle cerebral artery blood flow |
|
|
how is rhesus hemolytic disease managed postnatally |
check cord blood for blood type, hemoglobin, bilirubin and direct antibody test monitor bilirubin closely as level may increase rapidly and cause high frequency deafness or kernicterus start intensive phototherapy, adequate fluid balance and give IVIG (immunoglobulin) and perform an exchange transfusion if severe anemia or rapidly rising bilirubin concentration May need ‘top up’ blood transfusion for anemia within first threemonths of age until endogenous hemopoiesis is normal. |
|
|
how is rhesus hemolytic disease managed postnatally - summart |
check cord blood for blood type, hemoglobin, bilirubin and direct antibody test monitor bilirubin start phototherapy and give IVIG +/- exchange transfusion if severe anemia +- top up blood transfusion |
|
|
what is used in the prevention of rhesus hemolytic disease |
Anti D gammaglobulin given to rhesus-negative mothers during pregnancy, after potentially sensitizing events, and after delivery. |
|
|
when do you give rhesus negative mothers Anti D gammaglobulin to prevent rhesus hemolytic disease |
during pregnancy, after potentially sensitizing events, and after delivery. nb Neonatology at a Glance Fifteen percent of white women are rhesus-negative; less than2% of them become sensitized from inadequate or failedprophylaxis. |
|
|
whats the significance of maternal hyperthyroidism to the infant |
If mother is controlled on treatment, fetus and infant are usually unaffected. Rarely causes: Transient hyperthyroidism – fetal tachycardia, and neonatal hyperthyroidism (1–3%) – tachycardia, heart failure, vomiting, diarrhea and failure to thrive (despite good intake), jitteriness, goiter and exophthalmos (protuberant eyes). Treated for 2–3 months Transient hypothyroidism – from maternal drug therapy |
|
|
whats the significance of maternal hypothyroidism to the infant |
Important cause of congenital hypothyroidism, leading to short stature and severe learning difficulties. |
|
|
whats the most common cause of maternal hypothyroidism worldwide |
commonest cause is iodine deficiency. |
|
|
whats the significance of Autoimmune thrombocytopenicpurpura (AITP) to the infant |
Maternal autoantibodies against platelet surface antigens cross the placenta and cause fetal thrombocytopenia. Most fetuses unaffected. Rarely requires treatment in utero with repeated intravenous platelet transfusions.If severe, may cause cerebral hemorrhage before birth or from birth trauma, but this is rare. Infants withsevere thrombocytopenia or petechiae at birth should be given intravenous immunoglobulin. Platelettransfusions are reserved for platelet count <20000mm3 (20 × 109/L) or active bleeding because of theanti-platelet antibodies. The platelet count declines over the first few days before increasing |
|
|
Maternal drugs affecting the fetus and newborn infant |
Maternal drugs affecting the fetus and newborn infant |
|
|
what are some of the maternal drugs affecting the fetus and newborn infant |
maternal smoking alcohol narcotics - cocaine, heroin, thalidomide anticonvulsants antithyroid drugs Androgens Aspirin/non steroidal anti inflammatory drugs opiates folic acid inhibitors warfarin tetracyclines BB and hypoglycemic agents |
|
|
In the fetus, maternal cigarette smoking is associated with: |
• increased risk of miscarriage, abruption and stillbirth • reduction in birthweight, with increase in intrauterine growthrestriction (IUGR) related to number cigarettes smoked perday, with average birth weight reduction of 170 g at term. |
|
|
in a neonatal infant, maternal cigarette smoking is associated with |
• increased risk of sudden infant death syndrome (SIDS) • increased wheezing in childhood. |
|
|
Severe prolonged maternal alcohol ingestion is associated with |
fetal alcohol syndrome (FAS) |
|
|
Advice to pregnantwomen from the American Academy of Pediatrics and theDepartment of Health in the UK is to |
avoid alcohol whilstpregnant although the effect of occasional, mild alcohol inges-tion or occasional binge drinking is not known |
|
|
whats Neonatal withdrawal (abstinence) syndrome |
Serious problem because of widespread use of narcotics andother drugs of dependency. basically withdrawal symptoms associated with stopping narcotics or other dependent drugs Situation often complicated by multiple drug use |
|
|
mothers on heroin are usually encouraged to change to |
methadone to mitigate neonatal withdrawal syndrome |
|
|
drug users are at increased risk of |
hepatitis B and C and HIV infection if intra-venous drug user. |
|
|
when does the onset of withdrawals start |
– heroin <2 days – methadone <2 days but can be delayed up to 2 weeks. |
|
|
Cocaine does not cause problems from withdrawal but fromdirect transfer of the drug causing what fetal complications |
– placental infarction which may lead IUGR or placental abruption and antepartum hemorrhage or fetal death – rarely, cerebral infarction in utero and neonatal seizures. |
|
|
Clinical features of opiate withdrawal. |
Irritability Scratching Wakefulness Shrill cry Tremors Hypertonicity Seizures Unexplained pyrexia >38°C Tachypnea (rate >60/min) Vomiting Diarrhea Yawning Hiccoughs Salivation Stuffy nose Sneezing Sweating Dehydration |
|
|
when assessing someone with neonatal withdrawal syndrome what should you do |
assess them 6 hourly also use a scoring system e.g. Finnegan's scoring system to determine whether therapy is required |
|
|
treatment for neonatal withdrawal syndrome |
Usually with oral morphine sulfate, aiming to wean by titration ofdose with score. Medical and social services discharge planning meetings areoften required during pregnancy and after birth as the lifestyle ofmany drug users is not conducive to the care of babies andchildren |
|
|
medicines can also affect the |
fetus and newborn infants |
|
|
diethylstilbestrol (DES) given for threatened miscarriage in themother and subsequent association with |
clear-cell adenocarcinomaof the vagina and cervix in female offspring, evident only duringadolescence or early adult life. |
|
|
Pregnant women should avoid taking both prescribed and over-the-counter medications whenever possible |
true |
|
|
For prescribed drugs,the benefits must outweigh the risks and appropriate maternal andfetal surveillance should be undertaken. |
true |
|
|
Severe limb shortening (phocomelia, ‘like a seal’) frommaternal thalidomide therapy, which was widely marketed (not in US)for morning sickness from 1957. Teratogenic effects only recognizedseveral years later. |
true |
|
|
Thalidomide during Organogenesis (<8 weeks ’ gestation) results in |
Short limbs (Fig. 9.2)Absent auricles, deafness |
|
|
Anticonvulsants:• carbamazepine• valproic acid (sodium valproate)• hydantoins (phenytoin) during Organogenesis (<8 weeks ’ gestation) results in |
Fetal carbamazepine/valproate/hydantoinsyndrome – midfacialhypoplasia, CNS, limb andcardiac malformations Developmental delay |
|
|
Antithyroid drugs (iodides,propylthiouracil) after 8 weeks gestation results in |
goitre congenital hypothyroidism |
|
|
androgen medication after 8 weeks gestation results in |
masculinization of female |
|
|
aspirin or non steroidal anti inflammatory drugs after 8 weeks gestation results in |
closure of ductus arteriosus in fetus |
|
|
folic acid inhibitors (methotrexate) as cytotoxic therapy during organogenesis at <8 weeks gestation results in |
Fetal syndrome – microcephaly, neural tube defects, shortlimbs |
|
|
warfarin (coumarin) during organogenesis at <8 weeks gestation results in |
Fetal coumarin (warfarin)syndrome – nasal hypoplasia, microcephaly, hydrocephalus, optic atrophy, congenital heart defects, stippled epiphyses, purpuricrash |
|
|
tetracyclines during pregnancy at >8 weeks gestation results in |
Hypoplasia of tooth enamel,yellow–brown staining ofteeth |
|
|
beta blockers and hypoglycemic agents during pregnancy at >8 weeks gestation results in |
Neonatal hypoglycemia Poor fetal growth |
|
|
during labor and delivery what drugs cause respiratory depression of the neonatal infant at birth |
opiate analgesia |
|
|
define kernicterus |
bilirubin induced brain dysfunction Bilirubin is a highly neurotoxic substance that may become elevated in the serum, a condition known as hyperbilirubinemia serious complication related to very high levels of bilirubin. It can lead to permanent brain damage, hearing loss and death. Signs and symptoms of acute encephalopathy include: hypotonia, lethargy, poor feeding, irritability, high-pitched cry, seizures, apnoea and hypertonia. |
|
|
jaundice in neonates is mostly |
physiological |
|
|
small neonate |
Low birth weight (LBW): <2500g Very low birth weight (VLBW): <1500g Extremely low birth weight (ELBW): <1000g Appropriate for gestational age (AGA) infants weigh between the 10th and 90th percentile for gestational age. Small for gestational age (SGA) infants weigh less than the 10th percentile for gestational age. Large for gestational age (LGA) infants weigh above the 90th percentile for gestational age. IUGR: Growth restricted infants are not achieving their growth potential. Growth restriction can cause an infant to be small for gestational age. |
|
|
Approximately 60% of infants born at 24 weeks gestation will survive to discharge. Chances of survival improve with gestational age and 97% of infants born at 30 weeks are expected to survive. |
true |
|
|
Preterm babies are however at risk of disability in the long term. This includes cerebral palsy, developmental delay and visual and hearing impairment. |
true |
|
|
Antenatal corticosteroid administration to women at risk of premature delivery results in a significant decrease in the mortality rate of preterm infants. It has also shown to decrease the morbidity associated with prematurity, including respiratory distress syndrome, intraventricular haemorrhage and necrotising enterocolitis. |
true |
|
|
Prolonged hypoglycaemia can cause permanent neurlogic damage. At risk infants need to be monitored and managed appropriately to prevent this serious complication. |
true |
|
|
Risk factors for hypoglycaemia are: |
Intrauterine growth restriction Diabetic mothers Large for gestational age Prematurity Hypothermia Hypoxic ischemic encephalopathy Sepsis Haemolytic disease |
|
|
Birth asphyxia is defined as |
the failure to establish breathing at birth. Birth asphyxia is one of the major causes of early neonatal mortality. Improved neonatal resuscitation skills improve neonatal survival. |
|
|
Hypoxic-ischaemic injury is the most common cause of |
neonatal encephalopathy. use APGAR score to assess neuro function |
|
|
The VACTERL association consists of: |
Vertebral anomalies, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies and limb anomalies |
|
|
There are two antiglobin (Coombs) tests |
Direct antiglobin test Indirect antiglobin test |
|
|
Direct antiglobin test is used for |
used to detect antibodies on the red cell surface where sensitization has occured in vivo. |
|
|
a positive direct antiglobin test occurs in what conditions |
Haemolytic disease of the newborn Autoimmune haemolytic anaemia Haemolytic transfusion reactions |
|
|
Indirect antiglobin test is used for |
used to detect antibodies that have coated the red cells in vitro. |
|
|
the indirect antiglobin test is used in |
Routine cross-matching Detecting blood group antibodies in pregnant woman |
|
|
Glucose-6-phosphate dehydrogenase (G6PD) is |
an enzyme that plays an important role in red blood cell metabolism. G6PD deficiency is an X-linked recessive hereditary disease that can manifest in neonates as prolonged jaundice. The jaundice occurs secondary to red blood cell haemolysis. African, Middle Eastern and Southeast Asian people are most commonly affected. A Coombs test will be negative because the haemolysis is not immune mediated. |
|
|
The normal temperature range for a neonate is 36.5°C to 37.2°C. If not adequately attended to a newborn infant may experience hypothermia and cold stress. |
true |
|
|
Infants lose heat through: |
Conduction - heat is lost through direct contact with a surface with a different temperature Convection - air currents carry heat away from the body surface Radiation - heat loss via electromagnetic waves from the skin to surrounding surfaces Evaporation - heat loss when water evaporates from the skin or breath |
|
|
ward stuff |
ward stuff |
|
|
what respiratory condition in pediatric patients result in a focal or distributed sound across the chest on auscultation or what you can just hear |
asthma, bronchiolitis and croup result in wide spread or distributed sound pneumonia and foreign object typically focal sound |
|
|
if you hear any focal sound then the patient needs a |
chest x ray |
|
|
management for mild to moderate and severe croup |
mild to moderate = steroids severe = nebulised adrenaline |
|
|
brief pathophys of asthma |
allergen causes allergic response = mast cell release of histamines = bronchoconstriction and bronchospasms resulting in wheeze |
|
|
brief pathophys of bronchiolitis |
usually viral infection resulting in hypersecretion resulting in wheeze |
|
|
according to steve, children under 1 and maybe under 2 do not have asthma because they can't have an allergic reaction |
ok |
|
|
according to steve you treat asthma with beta agonist which will cause bronchodilation but it won't have the same effect on young infants with bronchiolitis, although as the children get older they develop more smooth muscle within their bronchioles which means that if you treat them with beta agonist for that bronchiolitis it will cause some bronchodilation and thus help to open up the airways (despite still having hypersecretion) reducing a wheeze |
ok |
|
|
Routine examination of the newborn infant |
Routine examination of the newborn infant |
|
|
A comprehensive medical examination within 24hours of birth, the ‘routine examination of the newborn infant’,should be performed. The purpose is to: |
detect any abnormalities confirm and or consider the further management of any abnormalities detected antenatally consider potential problems related to maternal pregnancy history or familial disorders allow the parents to ask any questions and raise any concerns about their baby determine whether there is concern by caregivers about the care of the baby following discharge provide health promotion, especially prevention of SIDS |
|
|
A comprehensive medical examination within 24 hours of birth, the ‘routine examination of the newborn infant’, should be performed. The purpose is to: (summary) |
detect abnormalities aid management decisions id probs with maternal preg hx or familial probs parents can ask questions about concerns concern after discharge health promotion esp prevent SIDS |
|
|
in preparing for a routine examination of the newborn infant what do you need to prpare |
Maternal charts (records) Equipment Environment |
|
|
Maternal charts (records): |
• Check maternal antenatal, labor and delivery charts. |
|
|
what equipment do you need for the routine exam of newborn infant |
• Tape measure. • Stethoscope. • Ophthalmoscope. |
|
|
what should you consider about the environment in which to carry out the routine examination of the newborn infant |
• Warm room free from drafts. • Privacy, suitably lit. • Examine on firm mattress in crib. • Both parents present if possible. • Always wash hands and clean stethoscope before eachexamination. |
|
|
regarding the infant what are important aspects to consider in the routine examination of the newborn infant |
baby must be completely undressed during the course ofthe examination so that all the body is observed needs to be relaxed = successful exam opportunitistic exam but must be done |
|
|
what does opportunitistic exam relate to |
i.e. check eyes whenopen, heart when quiet, hips left until last. However, the examina-tion must be complete. |
|
|
routine examination of newborn infants should include |
looking for any congenital abnormalities general appearance, posture, movements fontanel and skull structures - Look, feel check for dysmorphic facies check red reflex pale/red face check ears look and feel for cleft palate check tongue for central cyanosis check breathing (RR, WOB, resp distress) and chest movement check hands - digits, palmar crease check for jaundice auscultate chest check back and spine check abdomen - look, liver, spleen, kidney, masses, tender (whince) check femoral pulses check hips - DDH check muscle tone check genitalia - testis in scrotum, normal penis and anatomy for girls check anus - look for patency check feet for talipes do measurements for weight, head circumference and length (crown-rump) |
|
|
Significant congenital abnormalities which may be identifiedon routine examination |
Dysmorphic infant (see Chapter 8) Cataracts (see Chapter 61) Cleft lip and palate (see Chapter 39) Heart murmurs (see Chapter 48) Urogenital – hypospadias, undescended testes (see Chapter 51) DDH (developmental dysplasia of the hip) Imperforate anus (see Chapter 47) Spinal anomalies (see Chapter 58) |
|
|
Checking for red reflex. If absent, i.e. the pupil iswhite (cataracts, glaucoma, retinoblastoma), refer directly to |
an ophthalmologist |
|
|
what are the signs of respiratory distress |
increased respiratory rate flaring of nostrils grunting chest retractions (sternal and intercostal) |
|
|
the normal live can be palpated below the costal margin |
yes, normal liver 1–2cm below costal margin, spleen tip and left kidney may be palpable |
|
|
whats the normal newborn heart rate |
110 to 160 beats/min but may drop to 80 during sleep |
|
|
when examining the back and spine what are you looking for |
sacral dimples hair swelling nevus other lesions over the spine - e.g. spina bifida occulta ortethered cord nb if these found do ultrasound and then maybe MRI |
|
|
in coarctation what difference in blood pressure is significant |
greater than 15mmHg |
|
|
how do you assess muscle tone in neonate |
observe for normal movements of limbs feel when handling the baby (support the head when picking up baby) on holding prone, term babies will lift their head to horizontal position |
|
|
Back and spine: check from top to bottom.Sacral dimples below the line of the natalcleft – common and benign. If proximal tonatal cleft, ultrasound to identify if there is a track to the spinal cord, though rare |
true |
|
|
neurologic examination of the newborn |
states of alertness visual fixing and following hearing consolability head circumference face movements - cranial nerves, blinking, sucking strong posture and spontaneous motor activity |
|
|
a detailed neurological exam is done if any concerns about |
neurological abnormality |
|
|
A normal neurologicexam is helpful prognostically, e.g. following hypoxic–ischemicencephalopathy, a normal neurologic examination and normalfeeding by 2 weeks of age are associated with |
a good prognosis |
|
|
in the infant examination of alertness it is classified using the |
prechtl scale |
|
|
using the prechtl scale for classifying the level of alertness of infant, describe it |
1: eyes closed, regular respiration, no movements state 2: eyes closed, irregular respiration, no gross movements state 3: eyes open, no gross movements state 4: eyes open, gross movements, no crying state 5: eyes open or closed, crying. |
|
|
for a satisfactory level of alertness using the Prechtl scale, the level must be |
state 3 Inability todo this may occur because the infant is abnormally lethargic orhyperexcitable (or deeply asleep or hungry!). An abnormal crymay also indicate abnormal neurology. |
|
|
one of the neurological assessments of infant is visual fixing and following, what does this mean |
normal term infant should fix and follow a face or target of concentric black and white circles or a red ball moving from side to side |
|
|
when do you expect a neonate to be able to have visual fixing and following |
at about 32 weeks gestation The infantshould make eye-to-eye contact when held about 30cm from theobserver. |
|
|
in a normal neurological examination of hearing how should an infant respond |
Infants respond to noise with a facial grimace, turning of the heador startle |
|
|
another aspect of neurological exam is consolability, what is this |
baby stops crying to voice or soothing movements or gestures such as rocking from side to side. It indicates communication between the infant and caregiver. |
|
|
why is it important to measure head circumference in a neurological exam of an infant |
This is a surrogate measure of brain volume and subsequently ofbrain growth. |
|
|
Face (cranial nerves) |
There should be normal facial movements, blinking of the eyesand ability to suck strongly. |
|
|
what is the posture of a term baby |
flexed of all four limbs Movements are smooth, sym-metric and varied. The infant can move the fingers and can abductthe thumbs. |
|
|
in neonatal neurological exam its key to assess Posture and spontaneous motor activity |
Posture flexed Passive tone in limbs and trunk Active tone in limbs and trunk Primary reflexes Deep tendon reflexes Plantar responses |
|
|
passive tone in limbs and trunk are key parts of the posture and spontaneous motor activity in assessing neurology of neonate |
Develops from hypotonia at 24 weeks of gestation to strong flexortone at 40 weeks, initially in the lower then upper limbs |
|
|
Posture |
32 weeks Arms extendedSome flexion ofthe legs 40 weeks Full flexion ofall four limbs |
|
|
Passive tone in limbs and trunks looks at 3 key areas |
popliteal angle foot dorsiflexion scarf sign |
|
|
Passive tone in limbs and trunk Popliteal angle |
Popliteal angle - With thigh beside abdomen,extend knee as far aspossible 32 weeks 110 to 120 degrees Term 90 degrees or less |
|
|
Passive tone in limbs and trunk Foot dorsiflexion |
With knee flexed, ankle isdorsiflexedMeasure angle betweendorsum of foot and anteriorof leg 32 weeks 30 to 40 degrees Term 0 degress |
|
|
Passive tone in limbs and trunk Scarf sign |
Hand pulled across chesttowards opposite shoulderPosition of elbow noted 32 weeks very weak resistance Term Does not reach midline (i.e. strong resistance) |
|
|
Active tone in limbs and trunk looks at 3 main things |
righting reaction neck flexor tone ventral suspension |
|
|
Righting reaction involves |
Holding infant uprightunder axillae 32 Weeks Brief supportof lowerlimbs only 40 weeks Upright andtakes weightfor few secs |
|
|
neck flexor tone (raise to sit) involves |
Holding infant's shoulders,pull from lying to sitting 32 weeks No movementof headforwards 40 weeks Minimal headlag. Similarlyfor neckextensor tone(back to lying) |
|
|
ventral suspension involves (holding baby with back to ceiling and chest to floor) |
32 weeks Someextension ofhead andback 40 weeks Head extendedabove body,back extendedand limbs fully flexed |
|
|
what are the primary reflexes that are assessed as a part of the motor part of the neurological exam |
Placing reflex Palmar grasp Plantar grasp Asymmetric tonic neck reflex Motor reflex |
|
|
describe the placing reflex |
When dorsum of foot isstimulated by edge of bed,places foot on the surface |
|
|
describe the palmar grasp |
flexion of fingers when object placed in the palm of the hand |
|
|
describe the plantar grasp |
toes curl on stroking the ball of the foot |
|
|
describe the asymmetric tonic neck reflex |
fencing posture on turning head to one side |
|
|
describe the moro reflex |
On sudden head extension (butsupport the infant’s head in yourhand), symmetrical abduction andextension followed by flexion andadduction of the arms |
|
|
if the primary reflexes cannot be elicited what does that indicate |
central nervous system depression Moreimportant, their persistence suggests damage to upper corticalcontrol |
|
|
deep tendon reflexes may be decreased or increased in |
depressed in LMN lesions occassionally increased with UMN lesions check also for assymetry |
|
|
one deep tendon reflex is ankle clonus - what about it |
Ankle clonus is common and usually of no pathologicsignificance. |
|
|
plantar responses can be elicited but so what |
Elicited by stroking the lateral part of the foot from heel to toe.Unhelpful at this age as normal response may be flexor (toe down)or extensor (toe up). |
|
|
minor abnormalities in the first few days |
minor abnormalities in the first few days |
|
|
what are some of the minor abnormalities in the first few days |
distortion of the shape of the head (molding from delivery) caput succedaneum, cephalhematoma, chignon swollen eyelids subconjunctival hemorrhages from delivery small white cysts along the midline of the palate breast enlargement traumatic cyanosis peripheral cyanosis lanugo vernix umbilical hernia vaginal discharge cracking and peeling of skin positional talipes |
|
|
how can you tell the difference between true talipes equinovarus (club foot) and positional talipes |
The foot can be fullydorsiflexed to touch the front of the lower leg. In true talipes equinovarus this is notpossible. |
|
|
minor abnormalities in the first few days skin lesions |
stork bites milia miliaria erythema toxicum mongolian blue spots transient pustular melanosis aka transient neonatal pustolosis harlequin color change sucking blisters |
|
|
other minor abnormalities |
natal teeth - front lower incisors present at birth, remove if loose to avoid risk of aspiration extra digits - consult plastics; if thin skin tag, just tie off with silk thread ear tags - consult plastics; has increased risk of renal abn. |
|
|
define lesion |
A lesion is any single area of altered skin. It may be solitary or multiple |
|
|
define rash |
A rash is a widespread eruption of lesions. |
|
|
define dermatosis |
Dermatosis is another name for skin disease. |
|
|
description of skin lesion http://www.dermnetnz.org/terminology.html |
superficial/deep distribution configuration colour morphology skin surface secondary skin changes |
|
|
define macule |
A macule is an area of colour change less than 1.5 cm diameter.The surface is smooth. if its greater = patch |
|
|
define papule |
Papules are small palpable lesions. The usual definition is that they are less than 0.5 cm diameter, although some authors allow up to 1.5 cm. They are raised above the skin surface, and may be solitary or multiple. it may be: Acuminate (pointed) Dome-shaped (rounded) Filiform (thread-like) Flat-topped Oval or round Pedunculated (with a stalk) Sessile (without a stalk) Umbilicated (with a central depression) Verrucous (warty) |
|
|
enlargement of a papule in three dimensions (height, width, length) is known as |
nodule It is a solid lesion. |
|
|
define a cyst |
A cyst is a papule or nodule that contains fluid so is fluctuant. |
|
|
define plaque |
A plaque is a palpable flat lesion greater than 0.5 cm diameter. Most plaques are elevated, but a plaque can also be a thickened area without being visibly raised above the skin surface. They may have well-defined or ill-defined borders. |
|

what this |
Stork bites Pink macules on upper eyelids, mid-forehead (also called salmonpatch) and nape of the neck (Fig. 20.4). Common. Dilated super-ficial capillaries. Those on the eyelids and forehead fade over thefirst year. Those on the neck persist but are covered with hair. |
|

whats this |
stork bite |
|

whats this |
Miliaria Pin-sized vesicles, particularly over the neck and chest. Usuallydevelop at 2–3 weeks. Caused by sweat that is retained due toobstructed eccrine glands. Avoid excessive clothing and heating. |
|

whats this |
milia White, pinhead-sized pimples on the nose and cheeks and fore-head. Resolve during first month of life. Are from retention ofkeratin and sebaceous material in the pilosebaceous follicles. |
|

whats this |
erythema toxicum Small, firm, white or yellow pustules on erythematous base (Fig.20.5). It is the most common transient lesion, usually appears at1–3 days but up to 2 weeks of age; primarily on trunk, extremities and perineum. Moves to different sites within hours. Containseosinophils. May be present at birth. |
|

whats this |
erythema toxicum arises over the first few days, spares the palms and soles. It does not bother the baby. It resolves spontaneously over one to two days. |
|

whats this |
erythema toxicum affects 50% of full-term neonates but is uncommon in premature babies. |
|
|
mongolian blue spots |
Blue–black macular discoloration at base of the spine and on thebuttocks (Fig. 20.6). Usually but not invariably in black or Asianinfants. Sometimes also on the legs and other parts of the body.Fade slowly over the first few years. Of no significance unlessmisdiagnosed as bruises. |
|
|
Transient pustular melanosis(transient neonatal pustulosis) |
Resembles miliaria, but present at birth and may continue toappear for several weeks. Superficial vesiculo-pustular lesionsrupture within 48 hours to leave small pigmented macules withwhite surround. More common in black infants, in whom thelesions are often hyperpigmented. |
|
|
Harlequin color change |
Sharply demarcated blanching down one half of the body – oneside of the body red while the other is pale. Lasts a few minutes.Thought to be due to vasomotor instability. It is benign. |
|
|
sucking blisters |
Vesicles on hand, fingers or lips, from vigorous sucking in utero. |
|
|
whats the vernix |
greasy, yellow-white coating presentat birth, a mixture of desquamating cells andsebum which protects fetus from macerationin utero |
|
|
traumatic cyanosis |
skin discolorationand petechiae over the head and neck orpresenting part from cord around the baby'sneck or from a face or brow presentation.The tongue is pink |
|
|
small white cysts along the mid-line of the palate (Epstein pearls).Cysts of the gums (epulis) or floor ofthe mouth (ranula) |
true |
|
|
can it be normal to have swollen eyelids (without discharge) and vaginal discharge and cracking and peeling of the skin esp feet and hands at birth |
yes, don't worry it will go away |
|
|
what are some common or important birth injuries |
caput, chignon, cephalhematoma, subgaleal (subaponeurotic) hemorrhage, skull fractures minor injuries = forcep marks; scalpel lacerations |
|
|
what are some common or important birth injuries to the face |
facial palsy asymmetric crying facies |
|
|
what are some common or important birth injuries to the neck and shoulders |
fractured clavicle brachial palsy - erb palsy |
|
|
what are some other common or important birth injuries |
extremety fracture spinal cord injury intraabdominal organ rupture, injury or bleed genitalia bruising |
|

whats this |
chignon |
|
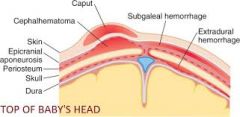
what are the anatomic locations of the different injuries to the head during birth |
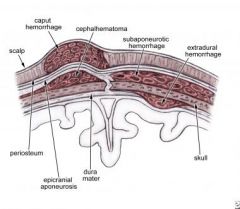
|
|

whats this |
Cephalhematoma |
|
whats this |
Subgaleal(subaponeurotic)hemorrhage |
|
|
which part of the skull is usually fracture in birth |
usually parietal occipital in breech deliveries |
|
|
genital disorders |
genital disorders |
|
|
what genital disorders should you look out for in birth |
inguinal hernia hydrocele undescended testis torsion of the testis hypospadias circumcision |
|
|
whats the classification of hypospadias |

|
|
|
Infants with hypospadias must not be circumcised as the fore-skin may be needed at surgery. |
true |
|
|
Neural tube defects and hydrocephalus |
Neural tube defects and hydrocephalus |
|
|
neural tube in embryo |
In the embryo, the flat neural plate folds to become the brain andspinal cord. |
|
|
Neural tube defects arise from a deficiency in thisprocess: |
• anencephaly – from failure of cranial development of most ofthe cranium and brain • spina bifida – from failure of caudal development of thevertebral bodies and spinal cord • midline defects – from failure of fusion, e.g. of the skull as anencephalocele. |
|
|
most neural tube defects are diagnosed how |
Most are now diagnosed antenatally, by ultrasound or α-fetoprotein measurement in maternal serum |
|
|
describe Anencephaly |
The condition is lethal; most are stillborn most are diagnosed antena- tally and parents opt for termination of pregnancy. |
|
|
describe encephalocele |
Herniation of sac, which may contain brain, through a midlineskull defect. Most are occipital (Fig. 58.1). Developmental impairment is likely if brain tissue is in the sac or there are other cerebralmalformations. |
|
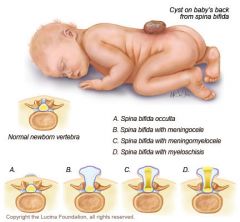
spina bifida types |
There are several types, of increasing severity: • spina bifida occulta • meningocele • myelomeningocele |
|
|
spina bifida work up |
need ultrasound or MRI scan |
|
|
meningocele has a good prognosis when |
following surgery |
|
|
myelomeningocele has a number of complications what |
associated with chiari malformation (herniation of the cerebellar vermis through the foramen magnum) kyphoscoliosis, DDH, talipes equinovarus neuropathic bladder - dribbling, predisposes to UTIs and vesicoureteric reflux, HTN, chronic RF
paralysis of the legs sensory deficity over the legs = skin damage from trauma |
|
|
whats the management of myelomeningocele |
MDT surgical closure to reduce infection risk and monitoring for hydrocephalus |
|
|
hydrocephalus |
This is from an excessive volume of cerebrospinal fluid (CSF).It is usually from blockage of CSF flow or a defect in CSFreabsorption. |
|
|
what are the congenital causes of hydrocephalus |
• Aqueduct stenosis. • Chiari malformation. • Atresia of outflow foramina of fourth ventricle (Dandy–Walkersyndrome). • Congenital infection. |
|
|
what are the acquired causes of hydrocephalus |
• Post-intrventricular hemorrhage in preterm infants. • Post-intracranial infection. • Post-subdural/subarachnoid hemorrhage. |
|
|
what are the clinical features of hydrocephalus |
• Ventricular dilatation on imaging precedes symptoms or signs • Increasing head circumference. • Separation of sutures. • Vomiting. • Apnea, abnormal muscle tone, seizures, depressed con-sciousness. • Dilatation of head veins. • Setting-sun sign (eyes deviate downwards). • Full then bulging fontanelle. |
|
|
management of hydrocephalus |
monitor with serial cranial ultrasound measurements for ventricular size and head circumference if severe and progressive or symptomatic = ventricular shunt surgically inserted |
|
|
Hydrocephalus in preterm infants |
usually secondary to intraventricular hemorrhage, whichmay cause obstruction but mainly interferes with CSF reabsorp-tion. The ventricular dilatation may regress, but if it progresses aventricular shunt will be required. Ventricular shunt insertion insmall infants may have to be delayed because of the risk of skinbreakdown, or shunt blockage if the CSF protein is high. If theinfant becomes symptomatic but a shunt cannot be inserted, CSFmay need to be removed by lumbar or ventricular puncture. A largerandomized trial showed no difference in long-term outcomebetween repeated lumbar/ventricular taps compared with removalof CSF only when symptomatic. Drug treatment with acetazola-mide, which reduces CSF production, is not used as it has beenshown to be ineffective and carries a risk of electrolyte imbalance.Therapy with fibrinolytic agents is under investigation. |
|
|
bone and joint disorders |
bone and joint disorders |
|
|
what are congenital abnormalities of the hip and feet |
DDH and talipes equinovarus (club foot) |
|
|
management for club foot |
• Refer to orthopedic surgeon. • Neonatal treatment – stretching, strapping or serial plaster castsstarted in first few days • Maximal correction is by 3 months of age. • Corrective surgery may be required at 6–12 months. |
|
|
bone and joint problems |
congenital = ddh and club foot infection = septic arthritis, osteomyelitis skeletal dysplasias = achondroplasia, osteogenesis imperfecta |
|
|
signs of septic arthritis |
• Decreased joint movement. • Joint is swollen, warm, red (Fig. 60.4). • Effusion may be present. |
|
|
is septic arthritis common in newborns |
no • Usually from extension from underlying bone infection, ratherthan primary infection of the joint or from hematogenous spread. |
|
|
septic arthritis diagnosis by |
joint aspiration suggesting infection |
|
|
what imaging options do you have for septic arthritis |
Ultrasound – fluid in joint space. Radionuclide bone scan, if indicated – hot spot. MRI scan of bone if necessary. Plain X-ray is of limited value – may show widened joint space. |
|
|
treatment for septic arthritis |
single or repeated needle aspiration surgical drainage of hip joint if no improvement antibiotics - for 3 to 6 weeks |
|
|
what are the long term complications of septic arthritis |
erosion of articular surface joint ankylosis |
|
|
osteomyelitis in newborns |
• Rare in newborn. • Most are hematogenous in origin, in metaphysis. • Usually presents within first 2 weeks of life. Pathogens Commonest are Staphylococcus aureus and streptococci. Signs • No movement (pseudoparalysis) of limb. • Red, warm, swollen, painful limb. Diagnosis • Blood culture positive. • Bone aspiration for cultures if indicated. Imaging • Ultrasound – periosteal elevation and soft tissue swelling. • Radionuclide bone scan, if indicated – hot spot (needle aspira-tion does not produce positive bone scan). • Plain X-ray – limited use at this stage, as only shows periostealelevation and soft tissue swelling. • MRI scan of bone if necessary. Treatment Antibiotics – prolonged course for 3–6 weeks. Continue for 2–3weeks after symptoms resolve and ESR (erythrocyte sedimentationrate) or CRP (C-reactive protein) normalizes. |
|
|
Achondroplasia |
• Short bowed limbs, normal trunk, large head. • Midface hypoplasia, frontal bossing. • Trident hand (short and broad), protuberant abdomen. |
|
|
Osteogenesis imperfecta |
• Inherited disorder of type 1 collagen formation. • Rare – 1 in 20 000 live births. Clinical features • Increased bone fragility, susceptibility to fracture (Fig. 60.5). • Blue sclerae, defective tooth formation in some patients. • Hearing loss. • Scoliosis, kyphosis. |
|
|
feeding |
feeding |
|
|
Human milk is recommended as the exclusive food for all terminfants for the first |
6 months of life. Human milk is also recom-mended for preterm infants but may need fortification. |
|
|
All mothersshould be encouraged and supported to breast-feed. Counselingshould commence early in pregnancy and mothers should beassisted by nursing or lactation specialists. |
true |
|
|
The choice to breast- or bottle-feed is personal and formulafeeding should not be criticized |
true |
|
|
Nutritional characteristics of human milk comparedwith unmodified cow’s milk |
Protein breast milk = 60% whey and 40 % casein, which is easily digestable and has high free aa and urea; glutamine the predominant aa, stimulates enterotropic hormones, enhancing feeding tolerance Fat breast milk has unsaturated fat contains long chain polyunsat FA needed for nervous system development Carb high in lactose minerals low renal solute load reduced phosphate: calcium ration vitamin supplementation required to breast milk to meet daily requirements |
|
|
does formula contain anti infective properties like breast milk |
no |
|
|
unmodified cow's, goat's and sheep's milk are unsuitable for infants |
true |
|
|
soy formula is sometimes used to prevent allergic disorders such as |
eczema and asthma although evidence for this is lacking about 10-30% of infants with cow's milk protein intolerance become sensitive to soy |
|
|
Immediate advantages of breast-feeding for the infant |
• Promotes mother–infant bonding. • Ideal nutritional composition (see below). • Contains immune factors (e.g. secretory IgA). • Reduces gastroenteritis, possibly other infections. • Less feeding intolerance. • Reduces incidence of necrotizing enterocolitis in preterminfants. • Promotes ketone production as an alternative energy substrateto glucose in first few days of life. |
|
|
long term advantages of breast feeding for the infant |
May reduce risk of SIDS (sudden infant death syndrome). May decrease incidence and severity of eczema and asthma. Less obesity, insulin-dependent diabetes mellitus (type 1) andinflammatory bowel diseases (Crohn disease and ulcerativecolitis). |
|
|
Advantages of breast-feeding for the mother |
• Enhances mother–infant bonding. • More rapid postpartum weight loss. • Decreased risk of osteoporosis. • Decreased risk of breast and ovarian cancer. • Increases time between pregnancies, which is important indeveloping countries. |
|
|
Potential complications of breast-feeding for the infant |
Cannot tell how much milk the baby has taken. - This is monitored by checking baby’s weight. Dehydration may occur if: – inadequate milk supply/poor feeding technique – hot weather. Jaundice associated with breast milk: – common – exacerbated by dehydration – even if requiring phototherapy, breast-feeding should becontinued – is prolonged (>2 weeks of age) in 15% – will require investigations to be performed. Multiple births: – twins can often be breast-fed, but rarely higher order births. Vitamin K: – low level in breast milk may predispose to hemorrhagicdisease of the newborn – prophylaxis is required. |
|
|
Potential complications of breast-feeding for the infant |
can't tell how much milk they had dehydration jaundice multiple births = twins ok, 1 teet each, but three = one misses out vitamin K deficiency |
|
|
Potential complications of breast-feeding for the mother |
• Maternal feeling of inadequacy/upset if unsuccessful. • Breast engorgement, cracked nipples – may be helped bymanual expression or breast pump. • Mastitis –requires maternal treatment and may disrupt feeding. |
|
|
Neonatology at a Glance Contraindications to breast-feeding |
Maternal HIV Maternal TB (active infection) inborn errors of metabolism - galactosemia, phenylketonuria |
|
|
drugs in breast milk |
• Most drugs are excreted in breast milk in such small quantitiesthey do not affect the infant. • Where possible, all drugs, including self-medication, shouldbe avoided during breast-feeding. Most mothers who need medi-cations can continue breast-feeding, but a few drugs precludebreast-feeding. |
|
|
‘Breast is best’ for feeding newborn infants. |
true |
|
|
growth and nutrition |
growth and nutrition |
|
|
Between 24 and 36 weeks’ gestation, a fetus growing along the50th centile gains |
15 g/kg/day Infants who are fed enterally require120–140 kcal/kg/day to maintain this rate of growth |
|
|
the weight of extremelypreterm infants is often initially static or may decline, and theinfant may take up to 21 days to regain birthweight. Thereafter,their growth improves but is often suboptimal. The reason for thisgrowth failure includes: |
• the infant is unable to tolerate high volumes of nutrients • fluids may be restricted, e.g. patent ductus arteriosus • intercurrent illness, e.g. infection. |
|
|
Nutrition for infant includes |
breast milk donor human milk formulas supplements - iron, multivitamins, vitamin K feeding |
|
|
what are the advantages of breast milk over formula feeds |
• better tolerated • associated with a lower incidence of necrotizing enterocolitisand provides some protection against infection • contains hormones and growth factors • has better absorption of fats and improved bioavailability oftrace minerals • promotes mother–infant bonding • it is associated with improved cognitive development later inchildhood. |
|
|
what are the disadvantages of breast milk over formula feeds |
• depends on the mother being able to express sufficient milk overa prolonged period • growth of the preterm infant may be suboptimal. Breast milkmay need to be enhanced with human milk fortifier to increase itsenergy, protein and mineral content. Human milk fortifiers containcow’s milk protein. Fortification is usually stopped once the infantis entirely breast-fed or weighs more than 2 kg. |
|
|
whats donor human milk and what is it used for |
its donor breast milk its given to extremely preterm infants or infants at increased risk of necrotizing enterocolitis The efficacy of donorhuman milk in improving outcome has not been determined. |
|
|
Low birthweight infant formulas |
supply the increased energy (24 kcal/oz, 80kcal/100mL), protein, sodium, calcium and phosphaterequired by low birthweight infants |
|
|
what supplements can be given to babies |
iron multivitamins - A, B12, C, D, E Vitamin K |
|
|
at what gestation would you expect a neonate to be able to suck and swallow |
34 to 35 weeks gestation |
|
|
for a term baby, they can be breast fed straight away, but extremely preterm infants cannot feed for themselves why |
are unable to suck and swallow until about 34–35 weeks ofgestation also initially unable to tolerate milk in sufficient quantity to meet their nutritional requirements |
|
|
methods of feeding |
Minimal enteral (non-nutritive) feeding Gavage (tube) feeding Total parenteral nutrition (TPN) |
|
|
Minimal enteral (non-nutritive) feeding |
A small volume (e.g. 10–20 mL/kg/day), preferably with expressedbreast milk, is given during the first few days to stimulate guthormone production even when the infant is too unwell or unstableto tolerate the expected volume of feeds. This helps intestinalmaturation, motility and gallbladder function, decreasing the timetaken to establish full enteral feeding; it also lowers serum bilirubinconcentrations |
|
|
Gavage (tube) feeding The tube may be orogastric or nasogastric. |
Used when infants are too immature (<34 weeks’ gestational age)or ill to feed for themselves but are able to tolerate enteral feeds The volume of milk is gradually increased. Feeds are withheldif aspirates are more than half the volume given or if biliouswith abdominal distension, blood in the stool or other featuressuggesting necrotizing enterocolitis. Reduced gut motility invery low birthweight infants may necessitate suppositories forconstipation. The tube may be orogastric or nasogastric. As nasogastric tubeslie in the narrowest part of the upper airway, just behind the nose,a size 5 French gauge tube increases airway resistance by 30–50%in preterm infants. This increases the work of breathing and mayincrease the frequency of apnea. Some units avoid nasogastrictubes if less than 35 weeks’ gestation, but orogastric tubes are moredifficult to fix securely. There is conflicting evidence regarding continuous versus bolusfeeding in relation to weight gain and the incidence of apnea andbradycardia. The infant’s oxygen tension falls with feeds in bothpreterm and term infants. It has been argued that continuousfeeding is more physiologic for preterm infants because it is acloser approximation to the way a fetus is fed in utero. However,bolus feeds are preferred as the response of gut hormones is morephysiologic. |
|
|
Total parenteral nutrition (TPN) |
feeding via central line usually or peripherally |
|
|
TPN is associated with a number of complications what |
• line-related infection • conjugated hyperbilirubinemia • electrolyte disorders • hyperglycemia • chemical burns from extravasation • pleural or pericardial effusion – if tip of the central line becomesdisplaced and lies in the heart. |
|
|
fluid intake is markedly affected by |
gestational age thermal environment (radiant warmer and isolette) evaporative water loss (reduced by humidity etc) |
|
|
fluid intake for infants use the |
4 2 1 rule 4 ml/kg/hour for the first hour 2 ml/kg/hour for the next hour 1 ml/kg/hour for subsequent hours |
|
|
example of the 4 2 1 rule you have a 2.7 kg baby and you need to give 70% of what ever fluid you plan to give as continuous infusion over an hour |
2.7 x 4 = 10.8 10.8 x 70% = 7.56 round up 7.56 = 8 ml/kg/hour |
|
|
you give 8 ml/kg/hour for the first hour, and you decide to start some feeding via tube/TPN, how much should you give |
the amount that was quoted in the hospital was Q2 hourly, so you give the same as the fluid i.e. 8ml/kg/hour but this is a Q 2 hourly amount, i.e. like giving 8ml/kg/30min but you want to give a continuous infusion over an hour, so what do you do you times 8 x 2 = 16ml/kg/hour of feeding |
|
|
lung development and surfactant |
fetal lung passes through 4 main stages of lung development during gestation 1) embryonic phase (3-5 weeks) - resp bud arises from ventral surface of foregut (esophagus) 2) pseudoglandular phase (6 - 16 weeks) - lobe branches develop 3) canalicular phase (17 - 24 weeks) distal airway develops 4) saccular phase (24 weeks to term) everything else |
|
|
Physiology and composition of surfactant |
It is hard to blow up a balloonthat is collapsed, i.e. has a small radius.Surfactant-deficient lungs are like this. (b) Itis easier to blow up once the balloon ispartially filled with air, i.e. has a larger radius.Lungs with surfactant are like this. In the absence of surfactant, thepressure at the surface of the alveolus isgreater in the smaller than the larger alveolus,so the small alveoli collapse and the largeones expand. Surfactant lowers the surfacetension (T) and prevents alveolar collapse. |
|
|
surfactant is |
90% lipids 10% proteins made by type 2 pneumocytes reduces surface tension thus helps to prevent alveolar collapse (atelectasis) and improves lung compliance, reducing the work of breathing |
|
|
deficiency in surfactant causes |
respiratory distress syndrome In surfactant deficiency, as the lung has low compliance (i.e. it isstiff), the change in lung volume for a given change in airwaypressure is much less than in the normal healthy newborn lung(Fig. 27.5). The pressure required to initiate lung inflation (‘openingpressure’) is also higher. Without surfactant the lung alveoli col-lapse to zero volume during expiration and the next breath startsfrom a low lung volume. These changes result in increased workof breathing and hypoxemia |
|
|
in suspected preterm babies you can give antenatal corticosteroids for lung maturation and surfactant production but what if the preterm baby is already born |
surfactant therapy can be given down a tracheal tube: - natural surfactant Preterm babies are given surfactant to either prevent or treatRDS. The strategies used are:• prophylactic surfactant – elective intubation and surfactantgiven in the first few minutes after birth• early selective surfactant – intubation and surfactant if infantneeds artificial ventilation after birth• rescue surfactant therapy – once the baby develops RDS. |
|
|
Effect of surfactant deficiency and lung immaturity in preterm infants. |
surfactant deficiency and structural lung immaturity leads to atelectasis which leads to - hypoventilation (this then also leads to hypoxemia) - hypoxemia + hypercarbia + acidosis - ventilation/perfusion mismatch (this then also leads to hypoxemia) hypoxemia + hypercarbia + acidosis leads to: pulmonary vasoconstriction + right to left shunting of blood (within lung, ductus arteriosus, foramen ovale) + proteinaceous exudate in alveoli (hyaline membrane) this leads to respiratory distress syndrome |
|
|
Respiratory distress syndrome (RDS) is also known as |
hyaline membrane disease (HMD) or surfactant deficient lung disease (SDLD) |
|
|
whats the commonest respiratory disorder affecting preterms |
respiratory distress syndrome nb a major cause of morbidity and mortality in preterm infants,although this has decreased markedly in recent years. |
|
|
the main risk factors for respiratory distress syndrome are |
prematurity |
|
|
surfactant is only produced towardsthe end of the second trimester and early third trimester |
true |
|
|
what are other risk factors for respiratory distress syndrome |
maternal diabetes mellitus sepsis hypoxemia and acidemia hypothermia |
|
|
Characteristic histopathologic features of RDS include: |
• collapsed terminal air saccules • overdistended terminal airways • influx of inflammatory cells into the airway lumen • interstitial edema and protein leak onto the surface of the airwaysand air saccules • hyaline membrane formation in distal and terminal airways • necrotic damage to airway epithelial cells. |
|
|
pathogenesis of RDS |
Caused by a deficiency in surfactant production or function. Thisresults in poor lung compliance (i.e. stiff lungs), which in turn leads to alveolar collapse and impaired gas exchange. Lung imma-turity may also contribute |
|
|
Antenatal corticosteroids markedly reduce: |
• incidence of respiratory distress syndrome • mortality. |
|
|
Onset within 4 hours of birth of respiratory distress: |
• tachypnea (>60 breaths/minute) • chest retractions (sternal and intercostal retractions) • nasal flaring • expiratory grunting • cyanosis (if severe). |
|
|
how is RDS diagnosed |
based on history, physical signs, characteristic chestX-ray (Fig. 28.4) and clinical course |
|
|
Chest X-ray (after 4 hours of age) in RDS showing: |
• diffuse, uniform granular (ground glass) appearance of the lungs fromatelectasis • air bronchogram – outline of air-filled large airways against opaquelungs • reduced lung volume • indistinct heart border as the lung fields are opaque (‘white-out’). |
|
|
Common causes of respiratory distress in preterm infants. |
Respiratory distress syndrome (surfactant deficiency) Pneumonia/sepsis Transient tachypnea of the newborn |
|
|
uncommon causes of respiratory distress in preterm infants |
Pulmonary hypoplasia Pneumothorax Congenital heart disease |
|
|
Rare causes of respiratory distress in preterm infants |
Diaphragmatic hernia Non-respiratory – anemia, hypothermia, metabolic acidosis |
|
|
other causes of respiratory distress in preterm infants |
refer chap 38 |
|
|
natural course of RDS |
is for the illness to become worse over the first24–72 hours and then improve over the next few days. There isinitially tissue edema from transudation of fluid into alveoli andsubcutaneous tissues, which resolves with improvement of lungdisease. These clinical features are markedly ameliorated by ante-natal corticosteroids and postnatal surfactant therapy. |
|
|
Management of RDS |
• antenatal corticosteroids • surfactant therapy – prophylaxis/rescue via tracheal tube • oxygen therapy • prevention of lung collapse – by applying CPAP (continuouspositive airway pressure) or PEEP (positive end-expiratory pressure) on a mechanical ventilator • lung expansion – by applying a peak inspiratory pressure witha mechanical ventilator, if necessary • provision of intensive care |
|
|
The main complications are: |
• infection/lung collapse • air leaks • patent ductus arteriosus • pulmonary hemorrhage • intraventricular hemorrhage • bronchopulmonary dysplasia (chronic lung disease). |
|
|
air leaks which is a complication of RDS - what does it include |
Pulmonary interstitial emphysema (PIE) pneumothorax |
|
|
Pulmonary interstitial emphysema (PIE) |
There is tracking of air from the overdistended terminal airwaysinto the interstitium. Increases risk of pneumothorax and bronchopulmonary dysplasia (chronic lung disease). thus terminal a/ws overdistended = air gets into interstitium |
|
|
Pneumothorax occurs in about 10% of infants ventilated for RDS. Presents with: |
increased oxygen requirement reduced breath sounds and chest movement on the affected side hypoxemia, hypercarbia and acidosis on blood gases shock. Confirmed by transillumination of the chest or chest X-ray tension or spontaneous pneumothorax can occur |
|
|
A tension pneumothorax is treated by urgent aspiration followed by insertion of a chest tube. |
true |
|
|
Pulmonary hemorrhage |
This is hemorrhagic pulmonary edema. In preterm infants it isusually associated with left heart failure from a patent ductusarteriosus (left-to-right shunting) with respiratory distress syndrome requiring mechanical ventilation. Causes blood staining of tracheal aspirate with or without shock. Incidence is about 3% of infants with respiratory distress syndrome requiring mechanical ventilation. Most of these infants willhave received surfactant, but this is no longer considered to be arisk factor. Coagulation may be deranged. |
|
|
pulmonary hemorrhage is usually associated with |
left heart failure from a patent ductus arteriosus (left to right shunting) with respiratory distress syndrome requiring mechanical ventilation |
|
|
whats the treatment of pulmonary ventilation |
• increase ventilation • surfactant • if necessary, replace blood/volume and clotting factors, butavoid fluid overload • close patent ductus arteriosus. Massive pulmonary hemorrhage has a high mortality. |
|
|
respiratory distress in term infants |
respiratory distress in term infants |
|
|
signs of respiratory distress |
Tachypnea (RR > 60/min) +Nasal flaring +Grunting (prolongedexpiration againstclosed glottis) +Chest retraction – suprasternal – intercostal – subcostal cyanosis if severe |
|
|
how do you monitor respiratory distress in term infants |
• Oxygen saturation (maintain >95% in term infants). • Respiratory rate, heart rate, BP, temperature. • Arterial blood gases if needing oxygen >30% |
|
|
what investigations should you do in addition to monitoring in respiratory distress in term infants |
• Chest X-ray – confirms respiratory disease, excludes pneumothorax, diaphragmatic hernia, lung malformations. • Complete blood count,blood cultures,C-reactive protein,consider lumbar puncture. |
|
|
management of respiratory distress ABC + ABs |
• Airway and breathing – oxygen/CPAP/mechanical ventilationas required. • Circulatory support if necessary. • Intravenous fluids or frequent nasogastric feeds. • Intravenous antibiotics – broad-spectrum coverage |
|
|
Common causes of respiratory distress in term infants |
transient tachypnea of the newborn |
|
|
less common causes of respiratory distress in term infants |
Pneumonia/sepsis Meconium aspiration Pneumothorax Congenital heart disease/heartfailure Persistent pulmonary hypertensionof the newborn (PPHN) Hypoxic–ischemic encephalopathy |
|
|
Rare causes of respiratory distress in term infants |
Surfactant deficiency Diaphragmatic hernia Tracheo-esophageal fistula Pulmonary hypoplasia Pleural effusion(chylothorax) Milk aspiration Airway obstruction e.g. choanal atresia Lung anomalies (cystic congenitaladenomatoid malformation (CCAM),lobar emphysema, pulmonarysequestration) Neuromuscular disorders Severe anemia Metabolic acidosis (inborn error ofmetabolism) |
|
|
Transient tachypnea of the newborn (TTNB) |
This is by far the most common cause of respiratory distress interm infants. Caused by delay in the absorption of lung liquid especially following elective cesarean section. Usually settles within first day or two of life, but may have mildoxygen requirement and take several days to resolve. |
|
|
pneumonia is a less common cause of respiratory distress in a term infant, but what are the risk factors for pneumonia in this case |
prolonged rupture of the membranes (PROM), maternal fever, chorioamnionitis, preterm |
|
|
less common causes of respiratory distress in a term baby caused by pneumonia All infants with respiratory distress should be started on broad-spectrum antibiotics until the results of the blood culture, C-reactiveprotein (CRP), complete blood count (CBC), lumbar puncture (ifperformed) are known. |
true, why? to rule out pneumonia causing the respiratory distress Group B strep is the most common cause |
|
|
Meconium aspiration |
The proportion of infants who pass meconium at birth increaseswith gestational age, affecting 20–25% at 42 weeks. |
|
|
Meconium aspiration |
Asphyxiatedinfants may start gasping and aspirate meconium before delivery.At birth infants may inhale thick meconium which results in mechanical obstruction, chemical pneumonitisand inactivation of surfactant . There is a high incidenceof air leak. Surfactant therapy may be beneficial. Mechanical ventilation is often required. Accompanying persistent pulmonaryhypertension (PPHN) may require nitric oxide or sildenafil and sometimes ECMO (extracorporeal membrane oxygenation), i.e.cardiopulmonary bypass. |
|
|
pneumothorax at term causing respiratory distress is most commonly a complication of |
mechanical ventilation or CPAP less common spontaneous |
|
|
heart failure |
Check for evidence of heart failure – including active precordium,enlarged heart, gallop rhythm, heart murmurs and enlarged liver.and that femoral pulses are palpable (reduced in coarctation of theaorta, hypoplastic left heart syndrome). |
|
|
Persistent pulmonary hypertension of the newborn(PPHN) |
Pulmonary hypertension leads to right-to-left shunting of blood: • across the patent foramen ovale • across the patent ductus arteriosus • intrapulmonary. |
|
|
Persistent pulmonary hypertension of the newborn (PPHN) is usually secondary to |
birth asphyxia meconium aspiration sepsis diaphragmatic hernia.Occasionally it is the primary disorder. |
|
|
Persistent pulmonary hypertension of the newborn (PPHN) usually presents as |
cyanosis or difficulty in oxygenation |
|
|
specific investigations for PPHN |
CXR echo |
|
|
management of PPHN |
• Oxygen. • Optimize mechanical ventilation. • Circulatory support as required. • Consider surfactant therapy. • Pulmonary vasodilator – nitric oxide (NO). Sildenafil (Viagra)also appears to be effective. • Consider high-frequency oscillatory ventilation (HFOV). • Extracorporeal membrane oxygenation (ECMO) as rescuetherapy for severe respiratory failure. |
|
|
rare causes of respiratory distress in a term baby |
surfactant deficiency diaphragmatic hernia |
|
|
Surfactant deficiency |
Rare in term infants. May occur in infants of maternal diabetes orwith surfactant protein B deficiency, a rare genetic disorder. |
|
|
Diaphragmatic hernia Main problems |
• Pulmonary hypoplasia, as herniated bowel reduces lung development in the fetus. • Lung compression by the bowel, which increases in size as airenters it. • Pulmonaryhypertension(PPHN) –pulmonary arterioles reducedin number and size, and smooth muscle is hypertrophied. • Other anomalies – present in 15–25%. Incidence 1 in 4000 births. |
|
|
the most common site for a diaphragmatic hernia is |
Left-sided hernia of bowel through the posterolateral foramen ofthe diaphragm (Bochdalek). |
|
|
whats the presentation for diaphragmatic hernia |
• Prenatal – on ultrasound screening, polyhydramnios. Mostidentified antenatally. For antenatal management • Resuscitation – failure to respond; deteriorates with bag andmask ventilation. • Respiratory distress – but onset may be delayed if underlyinglung well developed. |
|
|
Physical signs of diaphragmatic hernia |
• Reduced air entry on affected side. • Apex beat displaced. • Scaphoid abdomen – from reduced content of bowel. |
|
|
how is diaphragmatic hernia diagnosed |
chest abdo xray |
|
|
how do you manage diaphragmatic hernia |
• Intubate and ventilate from birth. Gentle ventilation, allowingpermissive hypercapnia, i.e. PaCO2 > 60 mmHg (8 kPa) but main-taining pH > 7.25. Avoid mask ventilation. • Pass large nasogastric tube and apply suction. • Stabilize and support circulation. • Early TPN (total parenteral nutrition). • Surgical repair – delay until stable and PPHN is resolving. • Nitric oxide or sildenafil (Viagra) for PPHN. • Extracorporeal membrane oxygenation (ECMO) – pre- andpost-surgery in selected cases. |
|
|
how many people die of diaphragmatic hernias |
20-30% |
|
|
Milk aspiration |
Risk of aspiration if infant has cleft palate, neurologic disorderaffecting sucking and swallowing or has respiratory distress. Infants with bronchopulmonary dysplasia (chronic lung disease)often have gastroesophageal reflux, which predisposes toaspiration. |
|
|
respiratory support |
respiratory support |
|
|
what are the different types of respiratory support |
supplemental oxygen CPAP – continuous positive airway pressure positive pressure ventilation HFOV – high-frequency oscillatory ventilation NO – nitric oxide ECMO – extracorporeal membrane oxygenation. |
|
|
when to give supplemental oxygen |
to avoid hypoxemia Hyperoxemia should also be avoided asit may increase the risk of ROP (retinopathy of prematurity) inpreterm infants and of tissue damage from release of free radicals In preterm infants, arterial oxygen tension is maintained at 45–80 mmHg (6.0–10.5 kPa) and oxygen saturation at 90–95% Term infants – maintain oxygen saturation at >95%. |
|
|
CPAP aims to prevent alveolar collapse at endexpiration and stabilize the chest wall. It also allows supplementaloxygen to be delivered continuously. |
true |
|
|
CPAP is used for |
infants withmoderate respiratory distress and for recurrent apnea. respiratory support after birth even in preterms help wean someone off mechanical ventilation |
|
|
CPAP may be delivered as: |
• bubble CPAP – the pressure is determined using a watermanometer • flow-driver CPAP – the flow driver provides a constant streamof oxygen; special nasal prongs maintain a constant pressurethroughout the infant’s respiratory cycle by changing the directionof flow during expiration (fluidic flip). |
|
|
Complications of CPAP are: |
• pneumothorax • feeding difficulties due to gaseous distension of the stomach • often poorly tolerated by term infants. |
|
|
If respiratory failure develops, mechanical ventilation is required. Some infants with bronchopulmonary dysplasia (chronic lungdisease) require nasal CPAP for many weeks. Prolonged use ofnasal prongs may cause nasal trauma, long-term damage to thenasal septum and deformity of the nose. Correct fixation willminimize this. |
true |
|
|
Is it better to commence nasal CPAP or intubate and givesurfactant in extremely preterm infants at birth? |
Trials (SUPPORT and COIN) have shown no significant difference in BPD (bronchopulmonary dysplasia) or mortality butnasal CPAP infants need fewer days of ventilation. Nasal CPAP has the attraction of being less invasive thoughmany subsequently require mechanical ventilation. |
|
|
Positive pressure ventilationIndications |
• Increasing oxygen requirement or work of breathing or increasing PaCO2 while on nasal CPAP. • Respiratory failure – defect in oxygenation (hypoxemia) and/orcarbon dioxide elimination (hypercarbia). • Respiratory support of the extremely preterm infant for first fewdays of life to prevent respiratory failure – depends on unit policy • Apnea – prolonged/recurrent. • Upper airway obstruction. • Congenital diaphragmatic hernia. • Circulatory failure. |
|
|
Intermittent positive pressure ventilation (IPPV) |
Ventilatory support is administered using a mechanical ventilatorthrough a tracheal tube. With conventional ventilation, intermittentpositive pressure ventilator breaths are given on a background ofcontinuous distending pressure (positive end expiratory pressure,PEEP) (Fig. 25.4). Alveolar ventilation is determined by the dif-ference between peak inspiratory pressure (PIP) and PEEP, theinspiratory time and respiratory rate. Most conventional neonatal ventilators are pressure-limited andtime-cycled. They are used as tracheal tubes are not cuffed and sothere is an air leak. |
|
|
In the presence of marked chest retractions, provide respiratorysupport, including mechanical ventilation if necessary, even ifthe blood gases are normal. Evidence of respiratory failure on blood gases is a latefeature. |
true |
|
|
Patient-triggered (assist/control) ventilation andsynchronous intermittent mandatory ventilation |
Two forms of synchronized mechanical ventilation are availableto promote synchrony between the ventilator and a baby’s ownrespiratory efforts – patient-triggered ventilation (PTV) and syn-chronous intermittent mandatory ventilation (SIMV). Bothmethods use a baby’s own spontaneous respiration to trigger theventilator to deliver a breath, usually from the change in airwaypressure or flow measured in the ventilator circuit; or from arecording of the infant’s respiration. In PTV each breath triggersthe ventilator; in SIMV only a preset number of breaths in a giventime are triggered. In both, there is a backup ventilation rate if theinfant does not breathe. Multicenter studies have failed to show any advantages of PTVor SIMV over conventional ventilation for preterm infants withrespiratory distress syndrome, although these forms of ventilationmay decrease the need for sedation. There is also increasing use of combining nasal CPAP with IMV(intermittent mandatory ventilation), i.e. additional positive pres-sure ventilation or SIMV. |
|
|
What are the causes of deterioration of a ventilated infant? |
Sudden deterioration: • Tracheal tube blocked/displaced. • Ventilator/circuit disconnected or malfunction.• Air leak – tension pneumothorax or pneumomediastinum. • Pulmonary hemorrhage. • Hemorrhage – intraventricular or other sites. Slow deterioration: • Increased lung secretions. • Infection. • Patent ductus arteriosus. • Anemia. • Developing bronchopulmonary dysplasia (chronic lungdisease). |
|
|
not finished still page 66 and 67 |
...but i think unimportant |
|
|
adaptation to extrauterine life |
adaptation to extrauterine life |
|
|
The transition from intrauterine to extrauterine life involves acomplex sequence of physiologic changes that begin before birth.Remarkably, although infants experience some degree of intermit-tent hypoxemia during labor, most undergo this transition smoothlyand uneventfully. If not, cardiorespiratory depression requiresprompt and appropriate resuscitation. |
true |
|
|
summary of physiological changes in fetal to neonatal transition |
fetal circulation - blood flow across the ductus arteriosus - blood flow across the foramen ovale - lungs - are filled with lung liquid newborn circulation - closed ductus arteriosus - lungs - become aerated |
|
|
when they refer to liquor in hospital what are they referring to |
amniotic fluid |
|
|
physiological changes in fetal to neonatal transition |
before birth : - lungs filled with fluid, oxygen supplied by placenta, goes to RA, some goes via patient foramen ovale to LA thus into aorta and circulation - blood vessels that supply and drain the lungs are constricted due to high pulmonary pressures (due to the fluid), so most blood flows from the right side of heart through the ductus arteriosus to the aorta - shortly before and during labor, lung liquid production reduces - during descent through the birth canal, infants chest is squeezed and some lung liquid exudes from the trachea - Multiple stimuli (thermal, chemical, tactile) initiate breathing.Serum cortisol, ADH (antidiuretic hormone), TSH (thyroid-stimulating hormone) and catecholamines dramatically increase. - The first gasp is usually within a few seconds of birth. A negativeintrathoracic pressure is generated to achieve this. Most lung liquid is absorbed into the bloodstream or lymphatics within the first fewminutes of birth. • Aeration of the lungs is accompanied by increased arterialoxygen tension; the pulmonary artery blood flow increases and thepulmonary vascular resistance falls. • Contraction of the umbilical arteries restricts access to the lowresistance placental circulation. This results in increased peripheralvascular resistance and an increase in systemic blood pressure. • The fall in pulmonary vascular resistance and the rise in systemic vascular resistance result in near equalization of pressuresacross the duct and virtual cessation of ductal flow |
|
|
Conditions associated with abnormal neonatal adaptation to extrauterine life. Fetal, maternal and placental causes |
Fetal causes Preterm/post-dates Multiple birth Forceps or vacuum-assisted delivery Breech or abnormal presentation Shoulder dystocia Emergency cesarean section Intrauterine growth restriction (IUGR)Meconium-stained amniotic fluid Abnormal fetal heart rate trace Congenital malformations AnemiaInfection |
|
|
Conditions associated with abnormal neonatal adaptation to extrauterine life. Fetal, maternal and placental causes |
Maternal causes General anesthetic Maternal drug therapy Pregnancy-induced hypertension Chronic hypertension Maternal infection Maternal diabetes mellitus Polyhydramnios Oligohydramnios |
|
|
Placental conditions associated with abnormal neonatal adaptation to extrauterine life |
Chorioamnionitis Placenta previa Placental abruption Cord prolapse |
|
|
what are some of the consequences of abnormal transition from fetal to extrauterine life |
hypoxic ischemic encephalopathy, persistent pulmonary hypertension andmulti-organ system failure. |
|
|
the APGAR score named after Virginia Apgar, an anesthesiologist,is used to describe an infant’s condition during the first few minutesof life |
true |
|
|
whose Ignaz Semmelweis |
hungarian guy first guy to wash his hands before surgery |
|
|
when should you do an apgar score |
assigned at 1 and 5 minutes of life If thescore is still below 7 or the infant is requiring resuscitation, it iscontinued every 5 minutes until normal or 20 minutes of age |
|
|
Although often assigned, few babies truly attain a score of 10,because it is uncommon for the baby to be pink all over. The Apgarscore is useful as a guide in rapidly assessing respiration, circula-tion and the nervous system, and as a record of the infant’s condi-tion shortly after birth |
true |
|
|
APGAR score includes |
Activity (muscle tone) Pulse Grimace Appearance (colour) RR |
|
|
The Apgar score is not used to determine the need forresuscitation. Evaluation for resuscitation is made second by second and isbased on the three most important signs: |
RR HR colour |
|
|
How does resuscitation affect the Apgar score? |
The Apgar score is assigned irrespective of resuscitationbeing performed. |
|
|
Can one determine Apgar scores in preterm infants? |
Yes. However, the extremely preterm infant’s maximumscore is reduced by poor muscle tone and weaker response tostimulation than term infants. |
|
|
Sustained, severe asphyxia (Fig. 11.2) in utero or during laborresults in nb sustained, severe asphxia in utero or during labor = increased WOB, then first apnea, HR falls but BP maintained if continuing asphyxia = infants gasps, HR falls more, BP falls, over several minutes after last gasp, theres a secondary apnea - to recover give positive pressure ventilation, +/- chest compressions |
the infant making increased respiratory effort, followedby a period of apnea (primary apnea). During primary apnea theheart rate falls to about half its normal rate but the blood pressureis initially maintained. With continuing asphyxia, the infant starts to gasp, the heart rateslowly falls, as does the blood pressure. After several minutes, aftera last gasp, there is secondary apnea. To recover, positive pressureventilation, if necessary accompanied by cardiac compressions, isrequired |
|
|
What is the long-term significance of a low Apgar score (3or less)? |
An infant with a low Apgar score at 1 minute but respondingrapidly to resuscitation has an excellent prognosis. An infant with a low Apgar score beyond 10 minutes of agein spite of adequate resuscitation is at increasing risk of neuro-logic injury resulting in cerebral palsy the longer the scoreremains low. |
|
|
Cardiac disorders |
cardiac disorders |
|
|
Congenital heart disease: |
• is the most common group of structural malformations • affects 6–8 per 1000 live births• accounts for 30% of all congenital abnormalities. |
|
|
what are the risk factors cardiac disorders |
• Chromosomal disorders and syndromes, e.g. trisomy 21 (Downsyndrome), microdeletion chromosome 22 abnormalities (foraortic arch abnormalities and Di George sequence), Turner,Noonan, Williams, syndromes and many others. • Maternal – diabetes mellitus, teratogenic drugs, e.g. anticonvul-sants, fetal alcohol syndrome. • Congenital infection, e.g. rubella. • Siblings of affected child – only slight increase in risk. |
|
|
microdeletion chromosome 22 abnormalities (for aortic arch abnormalities and Di George sequence) |
ok |
|
|
clinical presentation of neonatal cardiac disorders |
• Antenatal detection on ultrasound screening. • Detection of a heart murmur. • Heart failure – respiratory distress/shock. • Cyanosis |
|
|
antenatal diagnosis of especially severe cardiac lesions done |
via antenatal ultrasound e.g. hypoplastic left heart Lesions such as transposition of the great arteries and coarctationof the aorta are difficult to identify. |
|
|
what do you do if you find a cardiac abnormality of neonate at increased risk of one during antenatal ultrasound |
refer to perinatal cardiac specialist Antenatal detection allowsparents to be counseled and postnatal management planned |
|
|
About a quarter of infants with congenital heart disease presentin the neonatal period and usually have severe lesions |
true |
|
|
Classification of cardiac disorders. |
Acyanotic or cyanotic |
|
|
acyanotic cardiac disorders include - shunts, obstruction and pump failure |
Shunts (‘holes’) VSD (ventricular septal defect) 32% PDA (patent ductus arteriosus) 12% ASD (atrial septal defect) 6% Obstruction (‘narrowing’) Pulmonary stenosis 8% Aortic stenosis 5% Coarctation of the aorta 6% Hypoplastic left heart Pump failure Supraventricular tachycardia (SVT) Cardiomyopathy |
|
|
cyanotic cardiac disorders include |
Transposition of the greatarteries 5% Reduced pulmonary bloodflow Tetralogy of Fallot 6% (most common) Pulmonary atresia Tricuspid atresia Total anomalous pulmonary venousconnection (TAPVC) |
|
|
In infants with congenital heart disease: |
• 10–15% have complex heart disease with multiple lesions • 10–15% of children with congenital heart disease haveabnormalities of other systems. |
|
|
heart mumurs - Detected in 1–2% of normal infants on routine examination. The cause may be: |
A transient flow murmur Pulmonary artery branch stenosis Congenital heart disease |
|
|
whats a transient flow murmur |
related to circulatory changes following birth. The murmur is soft, systolic, at the left sternal edgeor pulmonary area in a well infant whose examination, includingfour limb blood pressure measurements, is otherwise normal. |
|
|
whats a murmur associated with Pulmonary artery branch stenosis. |
The murmur is best heardin the pulmonary area and radiates to the axilla and back. Resolvesin a few weeks. |
|
|
Congenital heart disease murmurs |
Though uncommon, the most worrying of these are duct-dependent lesions, which may result incirculatory failure or cyanosis when the ductus arteriosus closes The femoral pulses may be palpable even in coarctation of theaorta shortly after birth as the ductus arteriosus is still patent. definitive diagnosis = echo pulse oximeter useful if theres an innocent flow murmur, reassess infant in a few days to check murmur gone with worsening sxs to parents if worsening sxs develop = refer to peds cardiologist and echo |
|
|
does the absence of a murmur exclude congenital heart disease |
no |
|
|
Causes of heart failure in the neonatal period. |
Left-to-right shunting (high-output failure) Patent ductus arteriosus Atrioventricular septal defect (AVSD)/large ventricular septal defect (VSD) Left ventricular outflow obstruction (duct-dependent systemic circulation) Severe coarctation of the aorta Critical aortic valve stenosis Hypoplastic left heart syndrome Myocarditis/cardiomyopathy Arrhythmias Supraventricular tachycardia (SVT) Non-cardiac Severe anemia, polycythemia, arteriovenous malformation, e.g. vein of Galen malformation |
|
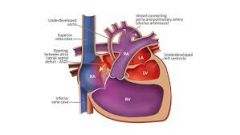
whats this |
a hypoplastic left heart |
|
whats this |
SVT |
|
|
Atrioventricular septal defect (AV canal defect) |
• Common (40%) in trisomy 21 (Down syndrome). • Surgery at 2–4 months. |
|
|
Large ventricular septal defect |
• Only presents at about 1–3 months, when pulmonary vascularresistance is low and left-to-right shunt maximal. • Surgery if medical therapy fails. |
|
|
Left ventricular outflow obstruction (low-output heartfailure/shock when duct closes) causes |
Severe coarctation of the aorta/interruption of the aortic arch Hypoplastic left heart Supraventricular tachycardia |
|
|
Severe coarctation of the aorta/interruption of the aortic arch - key features |
Key clinical sign is weak or absent femoral pulses. Blood pressurein the arms is markedly higher than in the legs (>20mmHg). Surgery is required. Less severe lesions may present as hypertension in adults. |
|
|
Hypoplastic left heart |
Presents with signs of low cardiac output when ductus arteriosuscloses. Pulses are weak at presentation, and there is severe meta-bolic acidosis. Fatal without treatment – requires a series of palliative operations (Norwood procedure) or heart transplantation. |
|
|
Supraventricular tachycardia |
Heart rate 220–300 beats/min • Heart is usually structurally normal, but accessory pathway(Wolff–Parkinson–White syndrome) is present in 40%. • If no response to placing ice pack on face, give the drug adenosine, or DC cardioversion |
|
|
Central cyanosis |
• is clinically detectable if there is over 5g/dL of reducedhemoglobin • is best detected in tongue/mucous membranes • in the absence of respiratory distress is usually due to cyanoticcongenital heart disease (Table 48.1). If there is respiratory distress, the cause may be: congenital heart disease pulmonary disease PPHN (persistent pulmonary hypertension of the newborn) polycythemia. |
|
|
Peripheral cyanosis (acrocyanosis) |
Hands and feet are blue. Common in infants in the first couple ofdays of life and in children of any age when cold. The tongue andmucous membranes are pink. It is of no clinical significance in theabsence of hypovolemia or shock. |
|
|
‘Traumatic’ cyanosis |
Cyanosis of the head, often with petechiae from venous congestion, e.g. caused by umbilical cord around baby’s neck or facepresentation. Tongue is pink. Resolves spontaneously. |
|
|
transposition of the great arteries |
aorta comes out of right ventricle and pulmonary artery from the left ventricle to survive, blood needs to mix via the foramen ovale or ductus arterious, less mixing = severe cyanosis |
|
|
with transposition of the great arteries, profound cyanosis occurs in the |
first day or two of life when the duct closes, but may be delayed if an ASD cause sufficient mixing |
|
|
whats the management of transposition of the great arteries |
give prostaglandin infusion to keep duct open balloon atrial septostomy to enlarge the foramen ovale (= promote mixing circulations) switch operation needed - where pulmonary artery and aorta switched over, coronary arteries also have to be transferred to the new aorta, which is technically demanding |
|
|
Total anomalous pulmonary venous connection (TAPVC) |
The pulmonary veins, instead of connecting into the left atrium,connect into the right side of the circulation, sometimes below thediaphragm. If the connection is narrow (obstructed) they present with cyanosis, respiratory distress and poor cardiac output. This may bedifficult to distinguish from surfactant deficiency. Treatment issurgical, sometimes in an emergency |
|
|
regarding cardiac anomalies what investigations should you do |
first you need to distinguish between, respiratory disorder, congenital heart disease and persistent hypertension of the newborn CXR - for lung diseases, enlarged heart (outflow obstruction or volume overload), abnormal shapes ECG - arrythmias, AVSD, tricuspid atresia Hyperoxia test echo and doppler cardiac catheterisation |
|
|
on chest x ray what are you looking for |
enlarged heart abnormal shapes (boot strap = ToF; egg on side with TGA) prominent pulmonary vascular markings from excess blood flow to lungs e.g. left to right shunt from patent ductus arteriosus reduced pulmonary vascular markings (oligemic) from reduced blood flow to the lungs e.g. tetralogy of fallot |
|
|
whats the hyperoxia test |
its just an arterial blood gas measuring partial pressure of oxygen at the radial artery If PaO2 >110mmHg (15kPa): – unlikely to be cyanotic heart disease – usually lung disease or PPHN (persistent pulmonary hypertension of the newborn). If PaO2 <110mmHg (15kPa): – likely to be cyanotic heart disease, but can be severe lungdisease or PPHN. |
|
|
management for cardiac anomalies |
ABC
correct metabolic acidosis, hypoglycemia and hypocalcemia give IV prostaglandin to keep ductus arteriosus patent (unless ASD then its already open) if in heart failure: - high output failure (after first weeks of life) - fluid restrict (acute only), diuretics, ACE inhibitors e.g. captopril - low output failure/shock - inotropes, volume support, arrhythmias require specific treatment refer to pediatric cardiac center |
|
|
Why may giving prostaglandin be life-saving? |
By keeping the ductus arteriosus patent when the circulationis duct-dependent. This occurs: • with obstruction to outflow of the left ventricle, when thesystemic circulation is maintained by blood flowing right to leftacross the patent ductus, e.g. severe coarctation of the aorta(Fig. 48.8) • with reduced pulmonary blood flow, when the pulmonarycirculation is maintained by blood flowing from left to rightthrough the duct, e.g. pulmonary atresia (Fig. 48.9). |
|
|
Ductus arteriosus – connects the pulmonary artery with thedescending aorta |
true |
|
|
ongoing patent ductus arteriosus is beneficial in patients with |
pulmonary hypertension some forms of congenital heart disease |
|
|
In utero – ductal patency: |
dependent on low PaO2 and high concentrations of vasodilatingprostaglandins (PGE2 and PGI2) |
|
|
Postnatal – ductal constriction is promoted by: |
• the rise in oxygen tension with the first breaths • the increase in pulmonary blood flow, which enhances clearanceof the local vasodilating prostaglandins. |
|
|
Ductal closure takes place in two stages: |
• functional closure – 24–48 hours after birth • anatomic closure – may take 2–3 weeks. In preterm infants, there may be delay in anatomic closure. |
|
|
with preterm infants a patent ductus arteriosus will eventually |
close spontaneously but unlikely for a term baby with a patent ductus arteriosus defect |
|
|
what are the risk factors for patent ductus arteriosus |
• Prematurity – incidence increases with decreasing gestationalage; most are less than 32 weeks’ gestational age. • Respiratory distress syndrome. • Sepsis • Pulmonary hypertension. |
|
|
clinical features of PDA patent ductus arteriosus |
Excessive pulmonary blood flow: • Tachypnea. • Increase in oxygen requirement. • Carbon dioxide retention, difficulty weaning from mechanicalventilation. • Apnea and bradycardia. Reduced systemic perfusion: • Tachycardia • Widened pulse pressure, causing bounding pulses • Active precordium • Heart murmur (see below) • Hepatomegaly (from right-sided heart failure). • Systemic hypotension; low diastolic arterial pressure in all. Heart murmur (Fig. 32.3): systolic best heard at left sternal border. If heart failure is present: gallop rhythm (extra third heart sound) may be loud pulmonic component (P2) of second heart sound. Silent PDA, i.e. no murmur but PDA present – common, usuallylarge shunt. The classic continuous murmur, systole extending into diastole,heard in older infants is rarely present in preterm infants. |
|
|
what is the typical murmur heard for a PDA |
classic continuous murmur, systole extending into diastole, heard in older infants is rarely present in preterm infants. |
|
|
clinical features of PDA with excessive pulmonary blood flow |
• Tachypnea. • Increase in oxygen requirement. • Carbon dioxide retention, difficulty weaning from mechanical ventilation. • Apnea and bradycardia. |
|
|
clinical features for PDA with reduced systemic perfusion |
• Tachycardia • Widened pulse pressure, causing bounding pulses • Active precordium • Heart murmur (see below) • Hepatomegaly (from right-sided heart failure). • Systemic hypotension; low diastolic arterial pressure in all. |
|
|
what investigations do you have for a PDA |
chest x ray echo with pulsed color doppler |
|
|
management for PDA |
medical management surgical closure |
|
|
medical management of PDA |
fluid management - fluid restrict esp if tx with indomethacin or ibuprofen (as they cause fluid retention) but reconsider if renal output normal diuretics - furosemide which leads to increased prostaglandin renal production to keep PDA, only use if medical tx failed/CI and waiting for surgery prostaglandin synthase inhibitors aka cyclooxygenase inhibitors (COXi) - indomethacin - ibuprofen |
|
|
surgical closure of PDA |
done if medical tx fails |
|
|
what are some of the complications of surgery for PDA |
• post-ligation cardiac syndrome – low systolic arterial pressure,need for cardiotropes and difficulty with oxygenation secondary toimpaired left ventricular function • recurrent laryngeal nerve damage, common, causing vocal cordparalysis • chylothorax from damage to thoracic duct • pneumothorax • ligation of pulmonary artery by mistake • mortality (<1%) but surgical closure is associated with worselong-term neurological outcome. |
|
|
What are the associated mobidities of PDA |
• Pulmonary hemorrhage • Cranial hemorrhage • Necrotizing enterocolitis • Bronchopulmonary dysplasia (chronic lung disease). |