![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back
|
1. How many percent formaldehyde is used in formalin solution?
|
37% formaldehyde is used to prepare 10% formalin solution |
|
|
2. During necrosis, describe and name the morphological changes of nucleus?
|
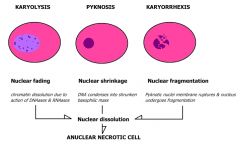
- all ncl changes are due to breakdown of DNA and chromatin by lysosomal enzymes (proteases and nucleases) pyknosis - condensation and clumping of nucleus which becomes dark basophilic karyorrhexis - Nuclear fragmentation in to small bitsdispersed in the cytoplasm karyolysis - dissolution of the nucleus |
|
|
3. What is pyknosis, and when does it occur?
|
- nucleus becomes smaller and stains deeplybasophilic as chromatin clumping continues (shrinkage of ncl, chromatin forms shrunken solid mass)
- seen in apoptosis as well as necrosis of the cells |
|
|
4. What is karyorrhexis, and when does it occur?
|
- pyknotic nucleus breaks up into many smaller fragments scattered about the cytoplasm - apoptotic cells |
|
|
5. What is karyolysis, and when does it occur?
|
- pyknotic nucleus may be extruded from the cell or it may manifest progressive loss of chromatin staining - necrotic cells |
|
|
6. What are the main causes of necrosis?
|
- reduced oxygen supply (arteriosclerosis, hypoxaemia...)
- physical agents (crush) - chemical agents (acid, lye) - toxins (corrosive sublimate) - viruses - abnormal immunological reaction - nutritional deficiencies (qualitative, quantitative) - genetic abnormalities (aging) |
|
|
7. Name the 5 different types of necrosis
|
1. Coagulative necrosis
2. Liquefactive (colliquative) necrosis 3. Caseous necrosis 4. Fat necrosis 5. Fibrinoid necrosis |
|
|
8. What is typical in coagulative necrosis, in which tissues does it occur, and does the tissuecontain much or less protein?
|
- most common type (irreversible focal injury) - in infarcts in any tissue (except brain) - Due to loss of blood - Gross: tissue is firm and pale - Micro: Cell outlines are preserved (cells look ghostly), and everything looks red |
|
|
9. White infarct in tissues is a result of what?
|
- white infarct (anemic)
- result of arterial occlusions in solidorgans with end-arterial circulations (e.g., heart, spleen, andkidney) |
|
|
10. Which tissues are mostly associated with white infarct?
|
- solidorgans with end-arterial circulations (e.g., heart, spleen, andkidney), and where tissue density limits the seepage of bloodfrom adjoining patent vascular beds |
|
|
11. What tissues are most likely to undergo coagulative necrosis?
|
- all tissues except of brain (solely liquefactive ) - spleen, heart, kidney |
|
|
12. What is liquefactive (colliquative) necrosis, and such a name as “liquefactive”?
|
- in infections and in brain infarcts - Due to lots of neutrophils around releasing their toxic contents, “liquefying” the tissue - Gross: center of the tissue is liquid and creamy yellow (pus), later cyst wall is formed - Micro: lots of neutrophils and cell debris |
|
|
13. What tissues are more likely to undergo liquefactive necrosis and why?
|
- tissues must rich in lipids - dissolution of the tissue by the action of hydrolytic enzymes - necrosis caused by bacterial infection - ischemia of CNS |
|
|
14. Which organ is mostly associated with liquefactive necrosis?
|
brain, CNS |
|
|
15. What is caseous necrosis?
|
- typical for tuberculosis (centre of foci)
- combines signs of coagulative and liquefactive necrosis - Due to the body trying to wall off and kill the bacilli with macrophages - Gross: White, soft, cheesy-looking (“caseous”) material - Micro: fragmented cells and debris surrounded by a collar of lymphocytes and macrophages (granuloma) |
|
|
16. What is the most commonly causative agent for caseous necrosis?
|
Mycobacterium tuberculosis |
|
|
17. What hypersensitivity is associated with caseous necrosis?
|
delayed hypersensitivity reaction (granulommatous inflammatory reaction) |
|
|
18. Caseous necrosis is a combination of two other types of necrosis, which?
|
causeous and liquefactive |
|
|
19. What is the etiology of fat-necrosis?
|
- in acute pancreatitis
- Damaged cells release lipases, which split the triglyceride esters within fat cells - Gross: chalky, white areas from the combination of the newly-formed free fatty acids with calcium (saponification) - Micro: shadowy outlines of dead fat cells (see image above); sometimes there is a bluish cast from the calcium deposits, which are basophilic |
|
|
20. Which organs are most prone to fat-necrosis, and why?
|
- pancreas (following acute pancreatic necrosis) - may affect fat depots through abdominal cavity - sometimes extra-abdominal as well
- breast (traumatic fat necrosis) |
|
|
21. What is saponification?
|
lipases split the triglyceride esters containedwithin fat cells - released fatty acids combine withcalcium to produce grossly visible chalky white areas |
|
|
22. What is fibrinoid necrosis?
|
- immune reactions in vessels
- Complexes of antigens and antibodies (immune complexes) combine with fibrin - Gross: changes too small to see grossly - Micro: vessel walls are thickened and pinkish-red (called “fibrinoid” because it looks like fibrin but has other stuff in there too |
|
|
23. What is microscopical typical feature of fibrinoid necrosis?
|
- brightly eosinophilic, hyaline-like deposition in the vessels wall (thickening)
- leucocytoclasis (necrotic focus surrounded by nuclear debris of neutrophils) - local haemorrhage may occur due to rupture of blood vessels |
|
|
24. What is the etiology of fibrinoid necrosis?
|
inflammation of vessels or hypertenion |
|
|
25. Can hypertension lead to fibrinoid necrosis, and why?
|
yes - it is unclear, but the following sequence is suggested: - initialevent = some form of vascular damage to thekidneys - this most commonly results from long-standinghypertension, with eventual injury to the arteriolar walls. - result is increased permeability of the small vessels to fibrinogenand other plasma proteins, endothelial injury, and plateletdeposition - appearance of fibrinoidnecrosis of arterioles and small arteries and intravascularthrombosis. |
|
|
26. What is gangrene?
|
for of necrotic tissue with super-added putrefaction |
|
|
27. What is putrefaction?
|
anaerobic decomposition of organic matter by bacteria and fungi that results in obnoxiously odorous products; rotting.
|
|
|
28. What is responsible for the black color in gangrenous tissue?
|
liberation of hemoglobin from haemolysed RBC which is acted upon by H2S produced by bacteria resulting in formation of black iron sulfide |
|
|
29. There are 3 basic types of gangrene, which?
|
dry, wet, gas |
|
|
30. What kind of gangrene is associated with diabetic foot?
|
wet gangrene (high sugar content favours bacteria) |
|
|
31. What kind of gangrene is associated with bed sores?
|
wet gangrene (increased pressure - blockage of venous, less commonly arterial blood flow = affected part is stuffed with blood) |
|
|
32. Which bacteria is associated with gas gangrene?
|
Clostridia (gram-positive anaerobic bacteria) |
|
|
33. What is the most common cause of dry gangrene?
|
ischemia of the distal part of the limb |
|
|
34. Which places is wet gangrene most likely to occur?
|
moist tissues and organs (mouth, bowel, lung, cervix, vulva) |