![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
261 Cards in this Set
- Front
- Back
|
What is normal Hematocrit (HCT)? What is Hematocrit? What are potential results of low levels? |
NL: 35 - 40, <30 = anemia, Drops as blood volume expands,with low-point at 28-30wks. Hematocrit is % of red blood cells in the blood LBW baby, maternal hemorrhage, dysfunctional labor, fetal distress |
|
|
What is normal Hemoglobin (HGB)? What is Hemoglobin? |
NL: 12-16, <10=anemia Hemoglobin is the Number of red blood cells that carry oxygen from the lungs to the body's tissues and returns carbon dioxide from the tissues back to the lungs. |
|
|
What is the Maternal Serum Alpha-Fetoprotein (MSAFP) Test? |
Th AFP is a genetic screening that measures the levels of AFP between the 16-18th week. Results are combined with mother's age and ethnicity to assess probability of genetic disorders. High levels of AFP: neural tube defect (spina bifida or anencephaly). The most common reason for elevated AFP levels is inaccurate dating of the pregnancy. Low levels of AFP and abnormal levels of hCG and estriol may indicate the developing baby has Trisomy 21( Down syndrome), Trisomy 18 (Edwards Syndrome) or another type of chromosome abnormality. |
|
|
When would a nuchal translucency screening happen? |
10-14 weeks |
|
|
When is Chorionic Villus Sampling done? |
anytime after 10 weeks Risks: higher miscarry rate than amnio, ROM, subchorionic hematoma, limb reduction reported in some early CVS (8-9 wks) Advantages: earliest definitive test for fetal chrom/genetic status, opportunity to terminate preg |
|
|
When is amniocentesis performed? |
Between 15-18wks Used to diagnose fetal disease, genetic conditions or to evaluate fetal maturity |
|
|
What is PUBS? |
Percutaneous umbilical blood sampling is used to directly sample fetal blood through the mothers abdomen |
|
|
What tests are in the Quad screen? |
Done at 16-18 wks AFP hCG Estriol Inhibin-A |
|
|
What Tx are included in prenatal labwork? |
Blood type and factor Antibodies: NL should be neg CBC: HGB 10-14, HCT 30-36% Rubella: measures mother's antibody titer RPR/VDRL - syphilis HEP B HIV PAP/GC/Ch Urinalysis Varicella |
|
|
When is the Glucose challenge screen offered? |
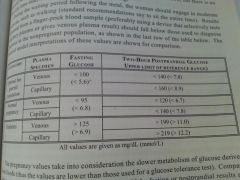
28 weeks
|
|
|
What are platelets? What is the normal range for platelets? |
100/140-400 million per millilitre (ml) of blood. Platelets are cells in your blood that help your blood to clot. Low platelet count in pregnancy is called gestational thrombocytopenia. **Low can indicate Preeclampsia |
|
|
What are some situations that would require an immediate call to the MW? |
Leaking of Fluid - Vaginal Bleeding - Persistent or Severe vomiting or you are unable to keep food or drink down for 24 hours. - Initial outbreak of blisters in the perineal or anal area during the 1st trimester - Severe pelvic, abdominal, or midback pain - Decreased Fetal Movement - Menstrual-like cramps more than 4-6 times an hour sometimes combined withbloody discharge can be a sign of premature labor. - Severe Abdominal Pain - Significant Generalized Swelling - Persistent or Severe Headaches after 25 weeks.- Fever of 101 F or Higher - Urgency or Burning With Urination - Signs of labor (UC's 5 min apart and strengthening, bloody show, ROM) |
|
|
Why am I even doing this? |

|
|
|
How much of their time do normal newborns spend sleeping? |
60% -- should alternate between sleeping and waking (quiet alert, active crying, crying, drowsiness) |
|
|
What are normal respirations for a newborn? |
40-60 BPM |
|
|
What is the NL temp for a newborn? |
97.7-99.5 F |
|
|
Normal newborn HR? |
110-160 BPM |
|
|
Normal newborn Bowel movements? |
Mec within 1st 24hrs then up to 72 hrs, transitional stool days 3-5 and bright yellow stool after mother's milk comes in.
|
|
|
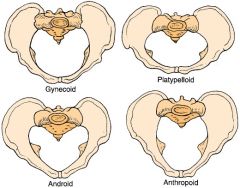
What is a gynecoid pelvis? |
round in shape, most common and most conducive to childbearing |
|
|
What is a android pelvis? |
male/ heart shaped pelvis, encroaching spines, narrow arch -- deep transverse arrest is often seen |
|
|
What is an anthropoid pelvis shape? |
anterio-posterior oval, posterior babies common |
|
|
what is a platypeloid pelvis shape? |
kidney shaped, most rare and least likely to have a vaginal birth |
|
|
LOOK! Pelvises! |
|
|
|
Show me some brightness |

|
|
|
TORCH...and I don't mean a flashlight |
Toxoplasmosis Other (HIV, syphilis, Hep B) Rubella Cytomegalovirus Herpes simplex (HSV) |
|
|
How is Toxoplasmosis contracted? |
Through cat feces, infected soil and infected or undercooked meat (pork) |
|
|
When is the fetus most at risk from toxo? |
HIGH RISK: 10-24wks Outcomes: Can cause severe congenitalmalformations if mother aquires infection in pregnancy, it crossesplacenta to fetus. Many infants don't demonstrate symptoms at time of birth, but later inchildhood. Seizures, motor and cognitive deficits, and mental retardation. Most severecases have nuerologic anomalies such as anencephaly, hydrocephalus, microcephaly, &intracranial calcifications. |
|
|
What would be the physical findings of a mother infected with toxo? |
flu like symptoms
swollen lymph system (glands) muscle aches and pains lasting weeks ABX can be given to mother c a new infection |
|
|
What are the effects of an untreated HepB infection for mother and baby? |
Maternal: preterm labor, cirrhosis and liver cancer Neonatal: stillbirth, 90% chance of chronic infections |
|
|
What the devil is Rubella? |
Rubella is a virus (German Measles) that is highly contagious -- If woman contracts rubella in 1st trimesterapprox. 52% chance that baby will be born with Congenital rubella syndrome (cataracts, cardiac defects, anddeafness.) Infection after 20 wksgest. rarely causes defects. |
|
|
What is CMV? or Cytomegalovirus |
Most common congenital infection @ birth in the US - 1% of babies: of those 1%, 10% will by symptomatic, of which 25% will have fatal disease and 90% of survivors will have serious consequences (hearing damage/loss,vision impairment, and varying degrees of mental retardation. ) -- 70% of children between 1-3 will be secreting CMV, mums should wash hands all the time |
|
|
Herpes |
Neonatal herpes is a severe systemic viral infection with high morbidity and mortality. This can occur if the mother acquires a primary during late pregand baby is born before development of maternal antibodies develop. Primary infectionoccurring in early preg can lead to congenital HSV infection which although rare can causesevere congenital abnlties. HSV transmitted to the baby during delivery may result inneonatal death, severe CNS, or ocular damage. |
|
|
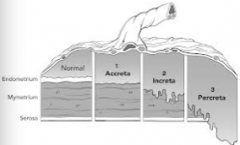
What are the layers of the uterus? |
Endometrium: innermost mucous membrane that lines the uterine cavity and contains glands, blood vessels and lymphatic spaces -- called the decidua in pregnancy "falling off" Myometrium: middle layer that is very vascular and makes up most of the uterus Peritoneum: outer layer |
|
|
What's hCG? |
Human Chorionic Gonadotropin: made by the embryo after conception and later by the placenta. May cause N&V. Prevents normal involution of corpus luteum at end of menstrual cycle...hCG causes corpusluteum to secrete increased amounts of estrogen and progesterone. hCG is used asbasis for pregnancy tests. hCG is present in maternal blood serum 8-10 days afterfertilization, and is detected In urine at times of missed period. hCG reaches its max 50-70 days gestation and begins decrease and plancentahormones increase |
|
|
Who loves you? |

|
|
|
What's progesterone? |
a hormone that enriches the uterus with a thick lining of blood vessels and capillaries to sustain growing baba and must be present in high levels for implantation to occur. Produced by the ovaries at first, the placenta takes overproduction of progesterone and secretes it after 10 weeks. May cause breast tenderness, heartburn, or constipation. |
|
|
Wait...but who ELSE loves you? |

|
|
|
What's even the point of estrogen? |
Causes enlargement of uterus, breasts andbreast glandular tissue, increase vascularity and vasodilation. By 7 weeks, theplacenta produces more than 50% of estrogen in maternal circulation. By end ofpregnancy, placental estrogen is 30X the daily production in middle of normalmenstrual period. |
|
|
What does hPL, human placental lactogen, do to ensure that the fetus gets what it needs? |
stimulates changes in maternal metabolic processes to ensure protein, glucose, and minerals will be available for fetus. hPL secretions can be detected by 4 weeks |
|
|
Try really really hard to remember the order of fertilization... G Z B E F |
Gamete(s) - Zygote - Blastocyst - Embryo - Fetus |
|
|
So like when do all those fertilization things happen? |
The ovum (gamete) passes into the fallopian tube and is fertilized by a sperm (gamete). They merge to make a ZYGOTE, once the zygote reaches the uterus it is a blastocyst, the outer layer becomes the placenta and chorion, the inner portion becomes the fetus, amnion and umbilical cord. When the blastocyst adheres to the uterine wall - implantation The zygote becomes an embryo until 8wks, when it becomes a FETUS |
|
|
What are some functions of the placenta besides paying your rent? |
- Providing metabolic and nutrient exchange between embryonic/maternal circulation - Pulmonary exchange of O2 and CO2 - Limited barrier for infections - Hormone production hPL, oogesterone, progesterone |
|
|
Functions of the umbilical cord? |
The body stalk attaches the embryo to the yolk sac andcontains blood vessels that extend into chorionic villi. As body stalk elongates, it becomes toumbilical cord (the vessels of the cord decrease to one large vein and 2 smaller arteries).Wharton’s jelly surrounds the blood vessels in the umbilical cord which prevents compression ofumbilical cord in utero. The cord can attach itself to the placenta at various sites although centralinsertion is considered normal. |
|
|
What about functions of the amniotic fluid...? |
- Protects and cushions baby from injury - Prevents adhesions - Allows free movement of fetus (muscle development) - maintains constant temp |
|
|
What are the three layers of the blastocyst? |
Ectoderm: mainly forms skin and nervous system Mesoderm: forms bones and muscles, heart and blood vessels; certain internal organs Endoderm: form mucous membrane and glands |
|
|
What week is implantation complete after fertilization? |
10-11th |
|
|
When does the fetal heart begin to beat? |
4 weeks |
|
|
What week marks the end of the embryonic period? |
end of 7th week |
|
|
What are some herbs that are contraindicated in pregnancy? |
goldenseal, ephedra, cotton root bark, blue cohosh, pennyroyal, birthroot |
|
|
What are the following sx of? elevated pulse, low BP, paleness of skin, cold sweat, clammy, low body temp, shallow/rapid resps, urine output decrease |
Shock |
|
|
What is hypovolemic shock caused by? |
Result of a reduction in intravascular volume, such as severe hemorrhage |
|
|
What is cardiogenic shock caused by? |
impaired ability of heart to pump blood, may be seen following pulmonary embolism or women with cardiac defects |
|
|
What might cause neurogenic shock? |
an insult to the nervous system - uterine inversion, septic or toxic, may occur with severe generalized infection |
|
|
Can a woman go into shock after an anaphylactic reaction? |
Yes |
|
|
What is the treatment for shock? |
o provide fluids orally o position mother flat, legs elevated o administer O2 o keep mother warm- avoid overheating o non-allopathic remedies - Rescue remedy o activate emergency medical services o prepare to transport |
|
|
What is the risk of not getting enough folate in pregnancy |
neural tube defects in the baby |
|
|
Why would a woman take vitamin C in pregnancy? |
80-500mg/day to help resist infection and help c iron absorption |
|
|
What is the daily dose of Magnesium in pregnancy? |
450mg -- Acts as catalyst in untilization of carbs, fats, proteins, calcium, andphosphorus. Coenzyme in energy and protein metabolism, enzyme activator, tissue growth, cellmetab, muscle action. High amounts may be toxic in people with kidney malfunction. |
|
|
What are the short term benefits to giving a laboring woman O2? |
acts as analgesic, relieving muscle tension as well as pain/nausea |
|
|
What risk factors make methergine contraindicated? |
women with impaired liver or kidney function, sepsis, HTN, pre-e, or Hx of PPD |
|
|
True or False: Never give methergine before the placenta has been delivered. |
TRUE. |
|
|
A BPP is scored by these and what else? - Fetal HR reactivity - Breathing movements - Amniotic fluid volume - Tone -__________________? |
Movement! +2 movements in 30 min |
|
|
How do you use a single dose vial? |
Assemble supplies, wash hands, open and close syringe, place filter needle on syringe. using a gauze pad, grasp vial belowneck place thumb of opposite hand above neck and break away from your body. Holdingsingle dose ampule insert syringe and fill syringe. Remove syringe and place needle forinjections. |
|
|
AND again ... what should hematocrit (% of RBC/ total blood volume) be above? |
should be above 33 hemodilution: significant drop occurs between 24-32 weeks o 1st- 36-48%, 2nd- 30-36% (hemodilution drop) Non-pregnant- 35-47% |
|
|
Hemoglobin should be above? |
should be above 11 Hemoglobin levels at different trimesters/PP(Hb):1st- 12-13, 2nd- 10-11 (2 pt drop nml around 28 wks), 3rd- 12-13 (or back to initial healthy level at beg. of preg) Non-preg- 11.5-16.5 |
|
|
What are some obstetric complications that may face an obesse woman? |
diabetes, HTN, pyleonephritis, uterine dysfunction, and hemorrhage |
|
|
What are complications that may arise for a malnourished pregnancy? |
IUGR, preeclampsia, maternal or fetal infection, prematurity, stillbirth, dysfunctional labor, hemorrhage |
|
|
When taking a new client's health hx she tells you that she had a LEEP procedure, what are you concerned about? |
incompetent cervix, premature labor |
|
|
TPALM? |
T- babies born at term P- babies born prematurely A- abortions; spont. or induced (any preg ending before 20 weeks) L- currently living children M- multiples |
|
|
Gravida means??? |
number of times a woman has become pregnant, regardless of multiples or when pregnancy was lost triplets = gravida 1 |
|
|
Para |
Number of pregnancies that terminated in birth of fetus that surpassed 28wks |
|
|
Renee has never been pregnant, she is a _______ |
Nulligravida |
|
|
What's the difference between the indirect and direct Coombs test? |
Indirect Coombs Test: (maternal screen) (neg; screens for minor blood factors and presence of antibodies; tests forpresence of antibodies in blood serum as opposed to RBC Direct Coombs test (fetal screen) (neg; checks presence of antibodies directly on RBC; could tell if fetal RBCare being attacked) |
|
|
A bluish cervix caused by increased vascularity would be called???? |
Chadwick's sign |
|
|
The bony opening through which the fetus passes during birth is called |
the True Pelvis |
|
|
How many calories does a pregnant woman need daily? |
-3000 calories -80 g protein -at least 2 qts water or more Assess and educate the specialized needs for nutrients in other types of diets. (vegetarian,vegan etc) |
|
|
If a mom was at a good weight before pregnancy she should gain about... |
a pound a week in pregnancy or 25-45 lb over the course |
|
|
What can odor tell you about that cup full of pee? |
Ammonia: after standing for awhile Fecal: recto-vaginal fistula Fishy: cystitis (bladder infection) New mown hay: diabetes Overripe apple: ketonuria—may be due to not eating enough Unpleasant: decomposition of certain foods or drugs |
|
|
What does the color of pee tell you? What might you suspect if her pee looked "rusty"? |
Clear to amber: normal to concentrated Pale to clear: very dilute- high fluid intake Milky: pus from UTI; vaginal secretions Red-orange: food, drugs or vitamin pigments; blood from vagina or kidney infection Bright yellow:B-vitamin supplements Brown or greenish: bile pigment- liver dysfunction Brown or black: severe urinary tract bleeding |
|
|
How often should you check for ketones in a long/tiring labor? |
Check for ketouria every 3 hours during long and tiring labors Ketouria may be first sign of clinical exhaustion and dehydration. Other signs include dry mucous membranes, rising pulse above 100 and rising temp above101, concentrated urine and rise in hematocrit |
|
|
What's the normal pH of urine? HINT: it's slightly acidic |
6.5 |
|
|
What foods help to heal the body of vaginal infections? |
dark-green veg, high-quality protein, whole grains, citrus and lots of fluids; cranberry juice to increase vag acidity |
|
|
Tell me more about BV -- how would you know to diagnose it and what would you do about it? |
Signs: increased ph, scanty, thin, homogeneous, milky, white, gray, or white,malodorous copious discharge; a positive wiff test, (vag. Irritation, pruritus, burningpain of the vulva- can be absent); fishy odor (particularly after sex) Microsoft Word - NARM EXAM study guide.doc dark-green veg, high-quality protein, whole grains, citris and lots of fluids; cranberry juice to increase vag acidity Risks: PROM, premature labor, chorioamnionitis Treatment: Antibiotics or unpricked clove of garlic 3x's a day and oral acidophilus for 5 days. |
|
|
What the devil is Naegele's rule? |
take LMP, subtract 3 months, add one week |
|
|
OH NO! I missed my period! What day after conception might I be able to have a positive urine pregnancy test? |
26 days after conception |
|
|
When might a first time mom expect to feel her baby move? |
16-18 weeks |
|
|
How accurate is ultrasound? |
In 1st trimester: accuracy of +/- 3 to 5 days depending on gestational age,sonographer’s skill, fetal position, and available technology. 2nd trimester: accuracy of +/- 1-2 weeks 3rd trimester: accuracy of +/- 2-3 weeks |
|
|
Where will the fundus be at 10 weeks? |
barely clears the SP |
|
|
Where will the fundus be at 16 weeks? |
1/2 between U and SP! |
|
|
What week will the fundus be at the belly button? |
20weeks |
|
|
What's the NL range of BP for a woman? |
90/50 - 140/90 30/15 above or below baseline warrants investigation |
|
|
What is NL pulse? and what would make it higher or lower? |
60-90 but a rise of 10-15 pts is normal in pregnancy High >100 - anxiety, anemia, pain, infection, hemorrhage Low - congenital heart defect, hypertension, hyperthyroidism, hypothyroidism |
|
|
What are NL resps? |
12-20 |
|
|
Maternal temp? |
97.6-99.6 |
|
|
What changes to diet can help reduce edema and why? |
salt food to taste, increase protein, and nutrient rich calories |
|
|
What are some presumptive signs of pregnancy? |
amenorrhea, N&V, tingling/enlargement of breasts, increased urination, fatigue, skin pigment changes, quickening |
|
|
What are some probable signs of pregnancy |
Enlargement of abdomen/uterus, palpation of fetal outline, fetal movement, palpation of bh ctx, +preg test |
|
|
Positive signs |
FHT, U/s |
|
|
What week is colostrum present in the breast? |
12 weeks |
|
|
When is the first trimester again? |
1-12 weeks |
|
|
How about the second trimester? |
13-27 |
|
|
And the third trimester is from when to when? |
28-40? DUH |
|
|
WWHo is predisposed to gestational diabetes if it's even a thing? |
family hx, obesity, >maternal age, previos baby >9lb |
|
|
What herbal relief could you offer a woman having difficulty sleeping? |
1/2 dropperful skullcap or valerian lavender Hops tincture in last trimester Homeopathic: aconite 30c for nervous tension |
|
|
What is the primary cause of nausea and vomiting in pregnancy? |
elevated estrogen and HCG |
|
|
What can offer relief from N&V |
50mg vit B6 at bedtime and midday small meals c protein regularly ginger tea/ capsules Homeopathics: pulsitilla, sepia, nux vomica, ipecacuanha, antimonium tartrate, argentums nitricum, petroleium, sulfur, tabacum |
|
|
What might fatigue and dizziness beyond the first trimester indicate? |
anemia |
|
|
A woman presents with itchy palms and soles of feets, you immediately suspect what and run what labs to confirm? |
intrahepatic cholestasis - bile acids and a liver panel |
|
|
Relief from general skin itchiness in pregnany? |
dandelion and yellow dock root tinctures, plain yogurt rubbed into skin, more sunshine, swim in the ocean |
|
|
Why are yeast infections more common in pregnancy? |
increased vaginal alkalinity caused by elevated progesterone levels |
|
|
What HGB and HCT should a woman striving for a homebirth maintain? |
HCT of 34 and HGB of 11.5 |
|
|
Vegans may be deficient in what vitamin found primarily in animal products? |
B-12 |
|
|
What effect might a B-12 deficient mother have on a newborn? |
CNS damage and may cause irreversible brain damage |
|
|
What non-allopathic remedies could you offer to a woman suffering from hemorrhoids? |
redclover and nettle infusion nourishes the circulatory system grated raw potato compresses witch hazel hamamelis 30c during flareups |
|
|
What herbal remedy might be effective against carpal tunnel in pregnancy? |
skullcap infusion and B6 regular exercise and acupuncture may also be helpful |
|
|
Tylenol is considered safe in pregnancy...what over the counter headache remedies are not? |
Aspirin/ ibuprofen (motrin, bayer, advil, nuprin, and medipren) |
|
|
Define the grading system for pitting edema |
+1 = 2mm +2 = 4mm +3 = 6mm |
|
|
What is the maximum amount of safe blood loss for a mother experiencing an inevitable abortion? |
2 cups (500cc) |
|
|
What is breakthrough bleeding? |
bleeding at 4, 8 and12 weeks of pregnancy, when you would normally have your period. Often accompanied back ache, cramps, aheavy sensation in your pelvis, feeling bloated and ‘off’. The perioddoesn’t arrive because during pregnancy, hormones prevent your period from occurring. Sometimes the hormone levels are not yet high enough to stop your period andtherefore you have this breakthrough bleeding. It can last for around threemonths – after this time the placenta begins to take over hormone productionfrom your ovaries. |
|
|
What week would an ectopic pregnancy be most likely to rupture? |
between 8-10weeks |
|
|
What four causes are responsible for rates of ectopic pregnancy increasing fivefold in the past decade? |
1. prevalence of STDs 2. trauma from IUDs 3. progesterone based contraception 4. infection following abortion |
|
|
A 6 wk pregnant woman comes to you complaining of consistent pelvic pain, spotting, and diarrhea. You immediately suspect? |
Ectopic pregnancy |
|
|
The drug methotrexate is used to....? |
dissolve an ectopic pregnancy which spares the tube potent chemotherapy drug that is a teratogen and folic acid antagonist |
|
|
What are the symptoms of a molar pregnancy? |
persistent light brown bleeding, uterus is large for dates and feels woody, hard or doughy to the touch. PIH or pre-e before 24 weeks |
|
|
A woman who is 34 weeks pregnant calls you and says she has had repeated episodes of light bleeding/heavy spotting. She tells you that the blood was bright each time and she feels no pain. You suspect _______________ and send her for an ultrasound to confirm. |
placenta previa |
|
|
Why is placenta previa associated with increased risk of 3rd stage hemorrhage? |
poor contractibility of lower uterine segment |
|
|
What risk factors predispose women to placenta previa? |
maternal age over 35, multiparity, hx of previa, multiple gestation, smoking and previous uterine surgery |
|
|
Non-allopathic remedies for HTN? |
o garlic supplementation o cal/magnesium and phosphorus o hops, skullcap, passionflower, hawthorn, and chamomile all induce relaxation and reduce systolic pressure. o Diastolic pressure can bereduced through the use of cayenne pepper, which acts as avasodilator and cardiac stimulant. |
|
|
Preeclampsia generally occurs after what point in pregnancy? |
26 weeks |
|
|
Describe preeclampsia |
inadequate albumin in bloodstream causes fluid to leak from cells, resulting in reduced blood volume, hemoconcentration and generalized edema. Blood flow to kidneys is reduced which triggers compensatory rise in BP. If hypertension becomes severe, vasospasm and irritation of cell walls causemicrothrombi (tiny clots) to form. These stretch the filtering slits in kidneys that largeprotein molecules begin to slip through, leading to proteinuria. Microthrombi can do significant harm to other arts of body; they can impaircirculation to liver leading to epigastric pain and liver damage or in sever cases, canlead to DIC as body exhausts clotting factors. |
|
|
Hemoconcentration at 28wks (abnormally high hematocrit-sharp contrast to usual dip in hct readings with hemodilution at this point in preg) would be a sign of what prenatal condition? |
preeclampsia |
|
|
What does HELLP stand for? |
Hemolysis, Elevated Liver enzymes, Low Platelets |
|
|
Pyelonephritis is |
a kidney infection |
|
|
What is pemphigoid gestationis (herpes gestationis)? |
autoimmune blistering skin disease that isn't herpes. generalized itching and burning of the skin c rash beginning on the abdomen and spreads to the rest of the trunk and extremities. developed blisters may become infected. Treatment: induction @ 35-37wks d/t placental insufficiency and IUGR |
|
|
What are the risks to a mother with gestational diabetes? |
4x pre-e 10x polyhyrdaminos higher risk of pp hemorrhage increased risk of shoulder dystocia |
|
|
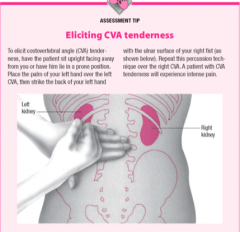
Where do you elicit CVA tenderness |
|
|
|
What is the definition of small for gestational age? |
fundal height less than 2cm weeks gestation |
|
|
What might cause SGA? |
IUGR fetal demise oligohydraminos (abnl low fluid) malnourished mother transverse/oblique lie genetically small infant that is normal! |
|
|
What is thrombophlebitis? |
blood clot slows the circulation in a vein *can be caused by sitting/standing stationary too long **varicose veins are risk factor |
|
|
What is Respiratory Distress Syndrome? |
baby struggles to get enough oxygen because there is inadequate surfactant (lubricating protein that allows alveoli to inflate) |
|
|
What are signs of RDS in a newborn? |
cyanosis, tachypnea, grunting with expiration, retractions, nasal flaring |
|
|
Before what gestation would a birth be considered preterm? |
after 20 weeks and before 37weeks |
|
|
Define preterm labor |
ctx causing cervical change &/or ROM before term gestation |
|
|
What are the components of the bishops score? |
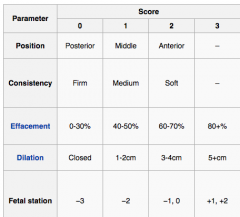
One point is added for: pre-eclampsia &/or every previous vaginal delivery One point is subtracted for: postdates, nulliparity (no previous vaginal deliveries), &/or PPROM Average score for induction = 6 |
|
|
What condition would contraindicate sweeping a woman's membranes ? |
low-lying or marginal placenta |
|
|
The normal pH of the vag during pregnancy is 4.5-5.5, what is the pH of amniotic fluid? |
7-7.5 |
|
|
What recommendations would you give to a full-term mom who has expereinced PROM? |
monitor temp every 3-4 hrs increase vitamin c to 250mg/ 2-4hrs no baths, no sex, nothing in vagina cotton undies if at all can take echinacea tincture |
|
|
After 24 hrs of PROM without labor how would your management change? |
prolonged rupture of membranes CBC may be necessary, ck FHT's regularly, supplemental vitamin E along with thevitamin C, ingesting 5 to 10 drops of Echinacea tincture 2 to 3 times a day to preventinfection, and drinking Nettle, Comfrey, or Violet leaf infusions for healing |
|
|
What is the protocol for dealing with HTN in labor? |
ck. B/P q 20m in labor, if it continues to rise transport, ck.clonus/hyperreflexia if pos. transport, ck. FHT's q 20m., push fluids, herbalremedies and epsom salt bath, if B/P rises in transition lay mom on left side c 6L/m O2 and if birth isn't imminent transport *B/P may rise to140/90 c exertion of 2nd stage* *watch for preeclampsia in p.p.* |
|
|
What is a normal pulse in pregnancy? |
55-95 BPM *increases by 15 BPM in early pregnancy and remains elevated |
|
|
What might be indicated by a maternal pulse over 100 BPM in labor? |
anxiety, pain, infection, ketosis, or hemorrhage *above 100 in first few hrs PP would indicate delayed PPH |
|
|
What can you learn from the color of amniotic fluid at ROM? |
- Green: meconium that may cause (or already has) fetal hypoxia - muddy/slightly green: previous meconium from which fetus has recovered - frank thick meconium- indicates a breech - golden-yellow: (rare) fetus severely affected by Rh isoimmunization (excessbilirubin in urine) - bleeding(upon ROM): may be caused from ruptured vasa previa and is an acuteemergency |
|
|
What are early decels in FHT thought to be caused by? |
head compression from 4-7cm a pattern of early decels before the head reaches the pelvic floor is unusual and may be due to extreme muscle tension linked to Hx of sexual abuse |
|
|
How is an early deceleration defined? |
decelerate at beginning of UC, reach low as ctx peaks, and return to baseline as it ends. In early 2nd stage dips by 10bpm are considered NL |
|
|
How are late decels defined? |
FHT dips at peak of ctx and slowly returns to baseline, may be linked to uteroplacental insufficiency or maternal ketoacidosis |
|
|
What are some causes of uteroplacental insufficiency? |
- fetal anemia associated with Rh sensitization - IUGR associated with maternal HTN, hyperthyroidism, intrauterine infection - ABNL placentation: revia, vasa previa - Abruption - HTN - severe dehydration -hypertonic UC (pit) -postdates |
|
|
True or False? Severity of fetal distress cannot be measured by depth of decels. |
True. A shallow decel is as serious as a deep decel, and is in fact dangerous because it’s easier to miss |
|
|
What FHT pattern would suggest hypoxia or maternal acidosis? |
no variability with prolonged or late decels |
|
|
What is thought to be the cause of variable decels? |
umbilical cord compression - but at various times in labor, not specific to a certain phase of labor or onset/peak/end of ctx |
|
|
Are variable decels usually cause for concern? |
No, variables that quickly return to NL baseline are not associated with hypoxemia or acidosis The seriousness depends on frequency, depth, rate of return, effect on baseline FHR and variability |
|
|
What are some causes of tachycardia? |
- maternal hyperthermia - fetal hypoxia - congenital anomalies (cardiac) - maternal dehydration - fetal anemia - hyperthyroidism |
|
|
What might bradycardia indicate? |
- maternal hypothermia
- prolapsed cord - OP/ transverse presentation of fetal head - cardiac anomalies |
|
|
What time intervals should you listen to FHT in labor? |
every hour in early labor, q 30 min in active labor, every 15 min or every few ctx in 2nd stage |
|
|
What is a sinusoidal pattern and what does it suggest? |
an undulating, repetitive, uniform FHR equally distributed 5-15 bpm above and below baseline for at least 10 min, associated with chronic fetal anemia *extremely rare and ominous pattern identified by an absence of short-term variability and no accelerations |
|
|
What is a wandering baseline? |
Appears to be a very late development in the progression offetal deterioration. An extremely rare finding, diagnosed when baseline FHR is unableto be found or established. It is usually WNL of 120-160, but is identifiable by its totalabsence of short-term variability. This is also an ominous indicator of fetal distress. |
|
|
Define effacement |
estimation of the percentage of cervix that has been drawn up into the lower uterine segment, how thin is it? |
|
|
Why would an arrest of labor possibly be concerning at 6cm? |
because the cervix can dilate to 6cm without pressure from the presenting part |
|
|
How do you determine what station the baby is at? |
find the presenting part and the ischial spines. Zero station when the head is in line with the ischial spine. Ranges from -4 to +3 -5 would be totally unengaged presenting part and +5 would be presenting part at vaginal opening |
|
|
Which fontanelle would you feel on a vaginal exam if the baby's head was deflexed? |
the anterior fontanelle, you would feel the triangle shaped posterior fontanelle if the baby's head was flexed |
|
|
What is the average timeline for a first time labor according to friedman's stupid curve? |
6.4 hrs for early, 4.6 hrs active and 1.1 hrs for pushing, subsequent labors being 50% shorter on average |
|
|
What homeopathics might be useful if the mother is dehydrated and/or vomitting? |
China, carbo veg, ustilago 200c |
|
|
What herbs might be useful for a mom who is dehydrated/ vomiting in labor? |
peppermint, chamomile, ginger pressure point PC-6 on inside of wrist |
|
|
What positions may be useful in relieving a swollen/anterior lip? |
H&K, leaning forward on ball, upright if she has been supine, side lying if she has been upright |
|
|
What can be given for a swollen lip?
|
arnica, sepia or ice on lip
|
|
|
How is a manual internal rotation (to reposition a posterior baby) completed? |
(Upon vaginal exam you should feel the anterior fontanellenear the pubic bone. 1. slightly disengage--dislodge ant. font. from the plane in the pelviswhere it is lodged, by spreading your fingers to either side of the sagittal suture and pushupward on the parietal bones--flexion and rotation may occur with this alone. 2. Exertsteady even pressure on the bony edge of ant. font. and rotate it to transverse position. 3.Now flex the head by pushing the font. toward the side of the vaginal wall, quickly reach for the posterior fontanelle, secure an edge and complete the rotation to anterior. (an assistantcan help externally by grasping the baby's shoulder and backside and pushing it to theanterior position. The mother can slowly roll over in the direction you are turning the babyat the same time--immediately check FHT's) |
|
|
What herbs might you use to induce rest in a laboring mother who is exhausted? |
hops, valerian or skullcap tinctures, glass of wine, homeopathic aconite |
|
|
How do you use a DeLee mucous trap?
|
check to see lid is screwed on tightly so device works properly, theninsert tubing about 4.5 inches into baby’s mouth. Withdraw slowly whilesucking sharply and repeatedly. Tell Mother not to push and have assstant holdshoulders back until you are finished. Repeat until no longer bringing upmeconium |
|
|
If the color of a baby's scalp is a good indicator of fetal well being a pink scalp would indicate what? |
pink:great, pink-blue:good, blue:not so great, whit-blue:ominous, lightly depress scalp to assess venous return |
|
|
What is a deep transverse arrest? |
The most common type of midpelvic disproportion, when the head is wedged behind the ischial spines and cannot rotate to the AP position
|
|
|
What is a frank cord prolapse? |
cord slips through the cervix |
|
|
What is an occult cord prolapse? |
cord slips down alongside presenting part but doesn't protrude through cervix |
|
|
How would you, as the midwife, respond to a frank cord prolapse? |
Place entire hand in vagina and hold presenting part up off umbilical cord at pelvicinlet, Do not attempt to replace cord Inform woman what has happened and elicit her cooperation Direct others to help woman get into position which gravity will aid keeping baby away from pelvic inlet: knee-chest or Trendelenburg position If cord protruding from vagina, direct others to wrap it loosely with gauze soakedwith warm normal saline o activate emergency medical services/medical backup plan to transport o monitor FHT o administer O2 to mother o faciltate immediate delivery, if birth is imminent and prepare to resuscitate the newborn |
|
|
What would be signs of partial abruption in 3rd stage? |
severe, persistent abdominal pain, tenderness, bleeding without lengthening of the cord, no apparent urge to expel the placenta, no placenta found at cervical os upon exam |
|
|
What would be appropriate midwifery management for partial separation PP? |
1. tincture of angelica 2. vigorous nipple stimulation 3. 10 units pit IM 4. repeat pit, injecting into cord 5. transport 6. with heavy bleeding MW must manually remove placenta 7. IV fluids, rest, carefully examine placenta for completeness and keep close eye on bleeding |
|
|
What are the risk factors for shoulder dystocia? |
post-dates, high parity, maternal obesity, AMA, maternal diabetes, fetal macrosomia, induction by pitocin, prolonged labor |
|
|
What would the appropriate management of a shoulder dystocia look like? |
stay calm Activate EMS, request readiness for full-scale newborn resusc effort request readiness for immediate PPH explain to mom • tell mother there is problem with delivery of baby’s shoulders, that youand baby need her cooperation, and that you will be doing things that willhurt her. Tell her that she must not push now. place mom in McRobert's or Gaskin, fetal shoulders are rotated into the oblique angle (One hand is placed on one side of the fetal chest, the other behind the opposite shoulder blade; as much force as necessary is used to rotate the body), apply suprapubic pressure (press downward and outward on the side of the head) Baby should receive Vit K after birth |
|
|
Cardinal rule for handling prolonged labors? |
"If labor begins to slow down,do not try to stimulate it!" Diminishing UC's is a sign that uterus is fatigued andmother should be encouraged to eat and rest in order for it to rebound. |
|
|
What are the specific signs of clinical maternal exhaustion? |
ketonuria, elevated temp, elevated pulse - ketoacidosis (when mum's blood becomes acidic and less able to carry O2, resulting in fetal stress) |
|
|
What would be clinical signs of an atraumatic uterine scar dehiscence? |
increased abdominal tenderness, severe suprapubic pain, lack of progress in labor, feeling faint |
|
|
Management of acute uterine inversion |
replace fundus asap• If placenta has not detached, reposition uterus with placenta still attached Start IV lie woman flat give rescue remedy, arnica, bellis perennis in 200C to 1M have assistant keep her conscious use sterile glove, apply lubricant insert hand into vagina if necessary. Hold center of fundus firmly in palm. Direct internal hand towards mother’s naval while use outside hand as guide. May take 3-5 min for fundus to gradually recede up toward palm after fundus is restored to normal position, clench internal hand into fist and begin bimanal compression Have assistant administer 10 units Pit IM Slowly remove hand by gradually converting closed fist into cone, taking care to let contracting uterus expel it rather than pulling out and risking anotherinversion Transport once woman has somewhat recovered from experience |
|
|
What is an embolism? |
entry of a foreign matter into the bloodstream, when matter enters lungs it can cause obstruction or constriction
|
|
|
What are the symptoms of an amniotic fluid embolism? |
more common in hard labor: gasping for air, dropping BP, depressed cardiac function, hypoxia, seizures, DIC Call 911, treat for shock, O2 If mother has given birth transport in supine position and do bimanual compression to avoid a massive, uncontrollable PPH |
|
|
What are the components of the APGAR?
|
heart rate, respirations, muscle tone, reflexes, color |
|
|
What are the physical characteristics of a baby born with Trisomy 18? |
small head, flattened forehead, receding chin, low-set and malformed ears, often a cleft palate. Short sternum, fingers may overlap and the feet have the rocker bottom |
|
|
What are the physical characteristics of a baby born with Trisomy 13? |
small stature with microcephaly, limb defects, midline facial defects (cleft palate, cleft lip) brain, renal and cardiac defects |
|
|
What are the physical characteristics of a baby born with Trisomy 21? |
widely set, obliquely slanted eyes, small nose, rough thick tongue, small head with flat occiput, simian crease |
|
|
Signs of a congenital heart defect in a newborn? |
pallor, transient tachypnea and central cyanosis, bounding or diminished pulses, variation of pulse from lower to upper extremities |
|
|
Ventricular septal defect is the most common CHD, what is it? |
is a defect in the ventricular septum, the wall dividing the left and right ventricles of the heart. may be heard via a murmur at 2-3 weeks may also hear loud, harsh, blowing pan-systolic murmur on the 2nd or 3rd day |
|
|
What are the components of the neuromuscular evaluation for gestational age? |
Posture: infant should crease at elbows, knees and feet (good tone) Square window Arm recoil: fully flex forearm for 5 sec and fully extend, release, elbow should flex at 90 degrees Scarf sign: draw infants hand over the neck as far over the opposite shoulder as possible Heel to ear should go to about navel at full term |
|
|
What are the components of the physical evaluation for gestational age? |
Skin Lanugo Plantar surface - creases Breast buds, raised 1-2/3-4mm buds Ear: pinna formed and firm, instant recoil genitals: testes down, good ruggae, labia majora larger than minora |
|
|
What is anencephaly? |
the cranial vault does not form |
|
|
What is an encephalocele? |
a myelomeningocele at the base of the skull that may contain brain tissue |
|
|
What is spina bifida? |
failure of the vertebral column to fuse |
|
|
What supplement is recommended to mums to prevent CNS disorders? |
methyl folate |
|
|
Herpes Zoster, Varicella, CMV and Toxo are all examples of what kind of infections that might affect a newborn? |
Congenital |
|
|
What are the two most common bacterial infections in newborns? |
GBS and E.Coli |
|
|
What would be the signs of sepsis in a newborn? |
ABNL body temp, vomiting, lethargy, poor milk intake, hypoxia, acidosis, dehydration |
|
|
What is the upper limit NL amount of blood lost after the birth of baby and before the placenta? |
2 cups, 500 cc |
|
|
What would be signs of hidden bleeding with a retained placenta? |
increased fundal height, signs of shock in mother |
|
|
What's the difference between placenta accreta, increta and percreta? |
|
|
|
What is normal PP blood loss in first two hours? |
1.5 soaked pads is normal with up to 3 soaked pads being OK, each pad contains 100ml blood |
|
|
How would you respond to a PP trickle bleed caused by uterine atony? |
- fundal massage, oxytocic herbs, IM pit, 911, bimanual compression |
|
|
Describe external bimanual compression |
grasp and lift the uterus firmly with both hands, then press together firmly -- one hand is dipped down as far as possible behind uterus while other is placed flat on abdomen. Uterus is compressed between the 2 hands and pulledupwards in the abdomen. This ensures the bleeding area of placental site iscompressed while uterine veins are straightened out to alow free drainage,relieve congestion and decrease bleeding |
|
|
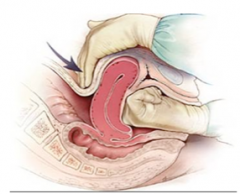
Describe internal bimanual compression |
one hand is inserted into the vagina and is made into a fist, pressure is exerted anteriorly, at the same time the other hand pushes deeply into the anterior vaginal fornix and towards the body of the uterus |
|
|
Did you get that? Here's a photo... |
|
|
|
Pitocin |
Pitocin- 10 IU intramuscularly Stimulates intermittent UC Little to no effect on BP if woman is having little heavy bleeding and is hypertensive, Pit will likely suffice |
|
|
Methergin |
Methergin- .2 mg/mL intramuscularly or .2mg/tablets Stimulates sustained, titanic UC May cause BP increase If woman is bleeding excessively as a result of uterine atony and her BP has been and is normal, Methergine is drug of choice Intramuscularly is warned against as it may cause sudden hypertension andcerebrovascular accident .2mg tablet may be repeated in 2-4 hours if needed |
|
|
Why would you not give shepards purse until after the placenta has been delivered? |
it causes clots |
|
|
What are the signs of shock again? |
decreasing BP, rapid pulse and respirations, cold/ clammy skin |
|
|
What might an elevated maternal BP indicate at 1 day PP? |
preeclampsia |
|
|
What is a first degree tear? |
degree of laceration involves the vaginal mucosa, posterior fourchette, and perineal skin First degree perineal tears do not require suturing |
|
|
2nd degree tear? |
tear in vagina, mucosa, posterior fourchette, perineal skin and perineal muscles Close lacerations in layers: muscle, fascia, skin |
|
|
Third degree tear? |
tear in vaginal mucosa, posterior fourchette, perineal skin, perineal muscles, and external anal sphincter |
|
|
Fourth degree tears include what? |
tear in vaginal mucosa, posterior fourchette, perineal skin, perineal muscles, external anal sphincter, and anterior rectal wall |
|
|
What is normal for newborn urine and stool output??? |
Mec is passed w/in first 24hrs and up to 72hrs, then 3-5 days of transitional stool, after the milk comes in the stool is bright yellow and 1-4 x/day Voiding should happen before first 24hrs, and at least 4-6 more wet diapers /day (clear or pale yellow) |
|
|
What are the components of a CBC |
Hematocrit; hemoglobin; mean corpuscular volume (MCV); mean corpuscular hemoglobin (MCH); mean corpuscular hemoglobin concentration (MCHC); red cell distribution width (RDW); percentage and absolute differential counts; platelet count (RBC); red cell count; white blood cell count (WBC) |
|
|
What would be signs of hypoglycemia in a newborn? |
defined as blood glucose 45 mg/dl or lower lethargy, poor feeding, hypotonia, irritability, resp problems, seizures, tachycardia, temp instability, apnea, emesis, pallor/ cyanosis |
|
|
What would circumoral cyanosis (blue ring around the mouth) lead you to suspect? |
linked to heart, circulatory, or intracranial pathology |
|
|
A bright red newborn could indicate what two things? |
prematurity and polycythemia (excess RBCs) |
|
|
What is a hematoma in a newborn skull?
|
an effusion of blood under the peristeum that covers the skull bones, does not cross suture lines
|
|
|
What is a cephhalhematoma? |
not present until 12hrs pp, will subside over time (may take weeks) will not pit with pressure |
|
|
What is caput and when would you expect it to disappear? |
swelling noted overlying the presenting part as a result of pressure from cervical os, it is moveable and not fixed, will disappear within 24 hrs |
|
|
What is crepitus, felt when palpating from sternum to shoulder on a newborn? |
the crinkling sensation of a broken clavicle |
|
|
What is erythema toxicum? |
Very NL newborn rash that looks a bit like flea bites and is apparent on the trunk area 24-48hrs after birth
|
|
|
Where should the uterus be on day 1 PP? |
1 fb below U, firm and not tender |
|
|
How soon after birth can ovulation occur? |
6 weeks |
|
|
What foods increase breast milk supply? |
oats, beets, almonds, carrot juice, apricots, pease, pecans, brewers yeast |
|
|
herbs to increase milk supply? |
blessed thistle, fennel, borage, red raspberry, fenugreek, hops, marshmallow root |
|
|
What is appropriate management for a woman with a vaginal hematoma? |
< 4cm and not enlarging-ice 24hrs., then heat, iron supplement,good nutrition, rest. >4cm or enlarges-refer consult |
|
|
What are symptoms of a uterine infection PP? |
fever over 101, pelvic pain and subinvolution of uterus, chills, foul smelling lochia, high pulse, achy/flu like |
|
|
What percent of women experience baby blues? |
70% |
|
|
What percent of women develop PPD? |
8-15%, occurring 10+days PP and worsening with time |
|
|
How can you confirm thrombophlebitis? |
Homan's sign: have mother sit in bed with leg straight and gently press on knee and dorsiflex her foot, if pain in calf, test is positive |
|
|
Pathological jaundice usually manifests within the first 24 hrs and is caused by what? |
liver disease, obstructed bile duct, infection or PH hemolytic disease |
|
|
how many times a day do most newborns feed? |
8-12 |
|
|
How to treat thrush without nystatin? |
applications of acidophilus solution three times a day by swab (not interferingw/ nursing), 1% Gentian violet 2X/day with cotton tip swap |
|
|
What is Gestational Diabetes Mellitus? |
presence of carbohydrate intolerance (with varying degrees of severity) with onset being noted during pregnancy. |
|
|
What are risk factors that make a woman more likely to have gestational diabetes? |
Older than 25 years marked obesity Non white race diabetes in first degree relatives previous infant >4000 grams Recurrent glycosuria poor obstetrical hx (congenital anomalies, spontaneous abortions) |
|
|
Where is insulin produced? |
in the pancreas |
|
|
How does the HPL produced by the placenta affect insulin? |
The HPL increases cellular resistance to insulin, resulting in hyperglycemia |
|
|
How is insulin potentially responsible for nausea and vomiting in some women before 20wks? |
The hormonal changes of pregnancy alter the cells to make them more receptive to insulin, which can result in hypoglycemia if the mother is not eating frequently |
|
|
What is phenylketonuria (PKU)? |
A birth defect that causes an amino acid called phenylalanine to build up in the body. |
|
|
PKU is very rare...how many cases in the US each year? |
10,000-20,000 |
|
|
What does classic PKU look like? |
The most severe form of this disorder is known as classic PKU. Infants with classic PKU appear normal until they are a few months old. Without treatment, these children develop permanent intellectual disability. Seizures, delayed development, behavioral problems, and psychiatric disorders are also common. |
|
|
What is congenital adrenal hyperplasia |
People have 2 adrenal glands, one located on top of each of their kidneys. These glands make hormones, cortisol and aldosterone, that are essential for life. People with congenital adrenal hyperplasia lack an enzyme the adrenal gland needs to make the hormones. At the same time, the body produces more androgen, a type of male sex hormone. This causes male characteristics to appear early (or inappropriately). Congenital adrenal hyperplasia can affect both boys and girls. About 1 in 10,000 to 18,000 children are born with congenital adrenal hyperplasia. |
|
|
What does hyperplasia mean? |
the enlargement of an organ or tissue caused by an increase in the reproduction rate of its cells, often as an initial stage in the development of cancer. |
|
|
What is hypothyroidism? |
abnormally low activity of the thyroid gland, resulting in retardation of growth and mental development in children and adults. |
|
|
What is galactosemia? |
a rare disorder that affects the body's ability to break down a food sugar called galactose (found in milk and other dairy products). The body breaks down lactose into galactose and glucose and uses these sugars for energy. |
|
|
Define hemoglobinopathies |
Hemoglobinopathy is a kind of genetic defect that results in abnormal structure of one of the globin chains of the hemoglobin molecule.Hemoglobinopathies are inherited single-gene disorders; in most cases, they are inherited as autosomal co-dominant traits. Commonhemoglobinopathies include sickle-cell disease. |
|
|
What is maple syrup urine disease? |
Maple syrup urine disease is an inherited disorder in which the body is unable to process certain protein building blocks (amino acids) properly. The condition gets its name from the distinctive sweet odor of affected infants' urine and is also characterized by poor feeding, vomiting, lack of energy (lethargy), and developmental delay. If untreated, maple syrup urine disease can lead to seizures, coma, and death. |
|
|
What population has a higher incidence of maple syrup urine disease? |
Maple syrup urine disease affects an estimated 1 in 185,000 infants worldwide. The disorder occurs much more frequently in the Old Order Mennonite population, with an estimated incidence of about 1 in 380 newborns. |