Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
78 Cards in this Set
- Front
- Back
|
what is attention? a good analogy?
|
The process that enables us to focus on a single source of sensory stimuli (the ability to sustain focus on one activity and block out all the other things). Analogous to a funnel
|
|
|
what is an interoceptive stimulus?
|
relating to stimuli produced within an organism, especially in the gut and other internal organs. e.g. hunger
|
|
|
what is an exteroceptive stimulus?
|
stimuli from outside e.g. mosquito buzzing in your ear
|
|
|
Before attention can be assessed, what must you determine?
|
the level of arousal e.g. a comatose patient cannot be attentive but a person can be alert yet not attentive
|
|
|
Attention may be ____ or _____
|
Intentional or Reactive
|
|
|
what is intentional attention?
|
When one deliberately focuses there attention on something (i.e. goal-directed). e.g. this lecture!
|
|
|
what drives intentional attention?
|
Frontal systems drive intentional attention.
|
|
|
what is reactive attention?
|
Shift in attention in response to internal or external stimuli. (older evolutionarily)
|
|
|
what is an example simple reactive attention? what parts of your brain mediate it?
|
when something grabs your attention immediately. e.g. reacting to insect crawling on your skin. Mediated largely through brainstem and thalamic systems (older)
|
|
|
what is required for complex reactive attention? e.g.?
|
when you are not focusing a priori on a stimulus and it grabs your attention; requires sensory association, polymodal and supra modal cortices in temporal and parietal lobe. e.g. passing of an enemy while walking down a street deep in thought.
|
|
|
what is the “Orienting response”
|
a movement (eyes and/or head and/or body) towards the stimulus
|
|
|
what structures does the “orienting response” depend on?
|
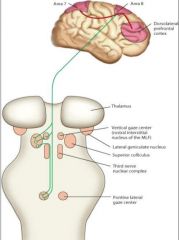
the brainstem, midbrain and cortical structures. only one synapse back to the cortex.
|
|
|
what is selective attention?
|
Our conscious awareness processes only a small part of all that we experience. We intuitively make use of the information we are not consciously aware of.
|
|
|
Humans have superb ____ attention abilities
|
selective attention abilities e.g. Cocktail party phenomenon; Can attend to one conversation among many
|
|
|
what is “inattentional blindness”
|
refers to the inability to see an object or a person in our midst. Simons & Chabris (1999) showed that half of the observers failed to see the gorilla-suited assistant in a ball passing game
|
|
|
what is “change blindness”
|
a form of inattentional blindness in which two-thirds of individuals giving directions failed to notice a change in the individual asking for directions.
|
|
|
in general, what do psychoactive drugs do?
|
they offer pharmacological control of consciousness
|
|
|
what is “substance abuse”?
|
when use leads to negative consequences and when drugs are overused and relied on to deal with everyday life.
|
|
|
DSM-V criteria for substance use disorders include (3):
|
1) The person has used a substance for one month, 2) Use has caused legal, personal, social, or vocational problems, 3) The person repeatedly uses the substance even in situations when doing so is hazardous**
|
|
|
in substance use disorders, what happens if use is decreased or stops?
|
withdrawal symptoms will occur if use is decreased or stopped; typically the opposite of a drug’s effects, and typically unpleasant
|
|
|
what alleviates withdrawal symptoms?
|
Can be stopped by taking more drugs; Doing so constitutes addiction
|
|
|
what brain system do “drugs of abuse” hijack?
|
the dopaminergic system. all of your attention is now directed at the use of the drug
|
|
|
taking drugs to prevent withdrawal symptoms is an example of ____ ____
|
negative reinforcement
|
|
|
psychoactive drugs result in what?
|
changes in consciousness that can affect behavior
|
|
|
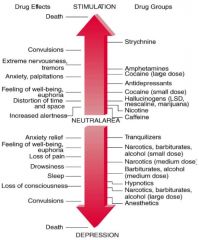
describe the range of drugs from depressants to stimulus
|
|
|
|
what is a big health risk with barbiturates?
|
increased potency / potentiation when combined with alcohol (basically giving two depressants)
|
|
|
what two stimulants have a “very wide window of safety” (in terms of overdose)
|
caffeine and nicotine
|
|
|
when might you see a severe, short period of stereotypic movement behavior?
|
when cocaine floods your patient’s basal gangs with dopamine -> stereotypies
|
|
|
what is strychnine?
|
one the most potent psychomotor stimulants; small window of safety; almost invariably causes convulsions
|
|
|
list the most commonly used psychoactive substances
|
(in order): Caffeine, Nicotine, Alcohol, Tranquilizers, Illegal drugs
|
|
|
what is the most commonly used depressant?
|
alcohol
|
|
|
what is the overall physiological effect of alcohol? like what NT?
|
(and other depressants) -> general slowing of the central nervous system; mimics GABAergic activity in the brain
|
|
|
contrast dose effects of alcohol
|
low doses produce general sense of well being (BAC ~.05) vs. higher doses (BAC > .1) -> More aggressive behavior (T, sexual response, more common in men); Severe cognitive impairment; Severe physical impairment vs. extremely high does (BAC > .7) can result in death (due to respiratory arrest)
|
|
|
what is the treatment for a patient with alcohol poisoning?
|
you flush the patient’s stomach with activated charcoal with (via esophageal catheter)
|
|
|
what is the most commonly accepted mode of action for alcohol?
|
may act as an allosteric modulator of GABA-A receptors (but unknown) to allow increased Cl- conductance -> hyperpolarization -> lower firing rate and slows down the CNS
|
|
|
what often happens with barbituates?
|
Can produce physical addiction; Withdrawal produces physical symptoms; range from mild (valium) to strong (anesthetics);
|
|
|
what is tachyphylaxis?
|
Rapid appearance of progressive decrease in response to a given dose after repetitive administration of a pharmacologically or physiologically active substance.
|
|
|
what happens with chronic use of many psychoactive?
|
you see receptor desensitization; receptors are firing and then get down-regulated. then you will need a larger dose of the agonist to achieve the same effect. e.g. people need to boost the same dose of valium (diazepam) or Xanax (alprazolam) to achieve the same effect.
|
|
|
what class of drugs are opiates?
|
depressants;
|
|
|
why are opiates such a problem?
|
1) they are some of the most potent narcotics; very small dose -> very large pharmacodynamic effect; so physical addiction is a big risk as is overdose risk (can be lethal)
|
|
|
withdrawal can cause ____
|
death
|
|
|
morphine and heroin work on ___ receptors
|
mu opioid receptors (very common in your brainstem)
|
|
|
why is heroin such a risk?
|
act on the brainstem which controls HR, breathing patterns, life-sustaining patterns; if you go just a little outside that region -> you’re toast
|
|
|
where does the expression “cold turkey” come from?
|
cold and goosebumps -> pilo erection and huge change in core body temp -> decreases by .5 to 1 degree C
|
|
|
cocaine used to be a treatment for _____
|
depression
|
|
|
examples of stimulants (3):
|
Nicotine, caffeine, cocaine
|
|
|
what are the overall physiologic effects of stimulants?
|
produce general increase in both somatic and autonomic nervous system; BP, heart rate, digestion, all increase. blood diverted to muscles
|
|
|
what are some side effects you may see with stimulant use?
|
Jitters and other physical manifestations, stereotypies (due to dopaminergic action)
|
|
|
what is one positive use of mild stimulants?
|
Mild stimulants (nicotine [alone*], caffeine) can have beneficial effects on performance; cognitive enhancers for older adults often based on nicotinic pharmacology -> Improved concentration, awareness, better performance
|
|
|
what is the NT affected by Ecstasy or MDMA?
|
affect the brain cells that produce serotonin (5-HT)
|
|
|
what is a big health risk with Ecstasy / MDMA?
|
affect areas involved in thermoregulation -> ecstasy-induced hyperthermia
|
|
|
what type of drug is Ritalin? (NT)
|
5-HT / serotonin and DA re-uptake inhibitor
|
|
|
why are people using Ritalin without prescriptions?
|
stimulant effects that decrease distractibility and improves concentration through dopaminergic mechanisms e.g. drug misused the most by medical students, residents, grad students, overworked people -> almost like getting cocaine
|
|
|
what is the addictive potential of stimulants?
|
Many stimulants can be physically addicting; Nicotine, caffeine, cocaine
|
|
|
how do stimulants affect your appetite?
|
Most act as appetite suppressors (e.g. a lot of people who quit smoking gain weight because increased appetite)
|
|
|
Most stimulants act how?
|
by increasing action of dopamine: Prevent uptake of DA on presynaptic terminal in an activity-dependent manner. so if blocked, raising tissue levels of DA
|
|
|
how do bath salts and meth affect DA?
|
increase release -> deplete the DA terminals of vesicles / stores
|
|
|
what is the neurobiological basis for addiction?
|
Release of dopamine and pleasure centers* (like rat pressing lever so much); like person addicted to cocaine trying to get more drug
|
|
|
what is the normal DA cycle?
|
DA is released, transduced at DA receptors (acts) and then (re)-uptaken and packaged back into vesicles normally
|
|
|
what is the mode of action for cocaine?
|
cocaine blocks the dopamine transporter (DAT), so DA is released and lingers in the extra-cellualar space -> increased availability of DA
|
|
|
what effect does the increased availability of DA have on a person addicted to cocaine?
|
enhances cue-directed relapse to drug seeking; main problem is not drug consumption itself but the chronic relapse pattern due to heightened DA state -> exteroeceptive triggers count more than they would otherwise
|
|
|
contrast withdrawal symptoms of different drug classes
|
psychostimulants have very mild withdrawal symptoms because not depleting stores vs. opioids and barbituates (can be very severe and lethal)
|
|
|
give 3 examples of hallucinogens
|
Marijuana, LSD, phencyclidine (PCP- “angel dust”)
|
|
|
in general, what do hallucinogens do?
|
Distort (exteroceptive sensory) perceptions
|
|
|
what is the “first thing that goes” when you take LSD or marijuana?
|
ability to perceive time. “how can you be conscious if you can’t tell how time is going by?”
|
|
|
marijuana _____ the internal clock. effect?
|
marijuana accelerates clock -> paradoxical effect of perceived slowing of time
|
|
|
contrast the “mild” vs. “severe” sensory distortions of hallucinogens
|
“mild,” e.g. from marijuana -> general slowing of time, increased attention to sensory input vs. “severe” (e.g., LSD, PCP) -> multi-sensory / multi-modal distortions (e.g., sound produces visual, tactile experience), a ‘bad trip’ from which people may never return
|
|
|
what NTs are affected by hallucinogens?
|
clear effects on GABAergic and Glutamatergic transmission, which are very ubiquitous, and also affects DA
|
|
|
what is a former use of PCP? its effects?
|
phencyclidine, used as anesthetic, Produces severe hallucinations and delusions; if combined with other drugs, particularly dangerous
|
|
|
where does marijuana come from?
|
the hemp, or Cannabis, plant
|
|
|
what is the major psychoactive ingredient in marijuana?
|
delta-9 tetrahydrocannabinol (THC), an organic lipid molecule that binds to (endogenous) cannabinoid receptors in the brain to bring about psychoactive effects
|
|
|
what do marijuana users often experience?
|
An increased sense of well-being/relaxation; Spontaneous laughter, a heightened sensitivity to various stimuli, a distortion of time, and a disconnected flow of ideas.
|
|
|
what is a big risk of consistent high quantity use of marijuana?
|
“amotivational syndrome” may have negative effects on motivation and interpersonal skills; “people just don’t want to get off their rear ends to do things)
|
|
|
what is a big risk of high quantity use of opioids?
|
death (opioids)
|
|
|
why is marijuana intoxication not lethal?
|
because CB receptors are not found in the brainstem despite its very ubiquitous presence elsewhere in the brain
|
|
|
what is the mode of action of marijuana?
|
a little complicated; involves DA release and another terminal either GABA or Glu; normally (re)uptake by the transport but THC blocks the GABAergic terminal
|
|
|
what does it mean that THC is disinhibiting?
|
it inhibits the inhibitor -> DA is amplified; results in excitation. negative times negative
|
|
|
marijuana acts on the ____ of DA neurons
|
the afferents (in particular GABAergic afferents) because dopaminergic neurons do not have CB1 receptors
|