![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
172 Cards in this Set
- Front
- Back
|
What are some of the underlying causes of a non-healing/delayed healing fracture? |
Metabolic disease Aging Obesity Open wounds Complexity Locations Breeds |
|
|
What is the name of the precursor cells that develop into chondrocytes, osteoblasts, adipocytes, myotubes and fibroblasts? |
Mesenchymal Stem Cells |
|
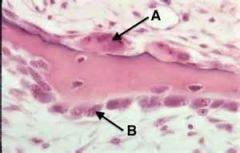
Identify: What is cell A? cell B? What are their functions? |
A: Osteoblast. These pillowy cells are responsible for making osteoid which will then mineralize to bone. *Note the cuboidal/columnar shape and location to bone B: OsteoClast: These more flatter cells are usually found in Howship's Lacunae forming a border around the bone |
|
|
Name the 4 things that osteoid is composed of |
Collagen, type I Proteoglycans Glycoproteins Noncollagenous proteins |
|
|
Name the 3 things that the cartilage matrix, made by chondrocytes is made of |
Proteglycans (especially aggrecan) Type 2 collagen Type 10 collagen |
|
|
What is the precursor cell of an osteoclast? |
Granulocyte and Macrophage precursors |
|
|
What are the two types of bone growth? |
Intramembranous (appositional) Endochondral |
|
|
Explain the process of appositional bone growth and where in the body would you find this type of growth? |
Osteoblasts lay down osteoid directly which is immediately bone. This type of growth is found in skull and flat bones |
|
|
Explain what happens in endochondral bone growth. Where would this type of growth be found in the body? |
Chondrocytes lay down a cartilage matrix which then undergoes proliferation, hypertrophy and mineralization. The osteoblasts then replace that cartilage matrix with osteoid, making bone. Then, vascularization happens and the cartilage matrix is digested, leaving just the bone in its place. This happens in rapid longitudinal growth and also in growth plates. |
|
|
Define and differentiate between the two types of fracture healing |
Primary- Appositional bone growth over a bone fracture. The parts of the bone have to be well opposed and the fix has to be relatively uncommon. *LIMITED inflammation Secondary- A combination of intramembranous and endochondral growth. The fracture fix is more complicated and you get *EXTENSIVE inflammation |
|
|
What are the 6 stages of fracture healing? |
Hematoma Inflammation/Debridement Mesenchymal Influx- Angiogenesis Mesenchymal Differentiation Bone Growth Remodeling |
|
|
What are the functions of the hematoma found in fracture healing? |
Stops bleeding, provides stability, releases pro-inflammatory signals |
|
|
In fracture healing, what happens in step 2, inflammation/debridement? What happens if this stage is interrupted? |
There is an influx of inflammatory cells making the initial matrix, cleans up debris in the area and releases growth factors If interrupted, you get a reduction in healing |
|
|
In the stage of fracture healing deemed "mesenchymal influx- Angiogenesis", what is formed? |
The soft callus (the "granulation tissue" of the fracture healing process" |
|
|
What happens during mesenchymal differentiation when it comes to fracture healing? What is the importance of vasculature in this stage? |
Mesenchymal stem cells are stimulated to differentiate from the periosteum. (Periosteum must be intact in order to have this step) You start to get intramembranous growth at the periphery of the callus, forming a bridge. If you don't have blood flow, you don't get healing. Blood is needed to bring O2, progenitor cells and clear waste from the healing site. |
|
|
During the remodeling phase of fracture healing, what three important things happen? |
1. Osteoclast resorption of the bone 2. Secondary bone formation, making a more sturdy/mature bone 3. The original bone shape gets restored |
|
|
What is the single most important thing that regulates the rate of fracture healing? |
Mechanical Stability! Some loading is needed but too much or not at the right apposition leads to delayed healing. |
|
|
What are the two growth factors important in fracture healing? |
1. Bone Morphogenetic protein (BMP) 2. Wnt signaling |
|
|
What is the function of Bone Morphogenetic protein (BMP) |
It is needed for osteoblast and chondrocyte differentiation and regulation |
|
|
What is the function of Wnt signaling in fracture healing? What is the Wnt inhibitor and what is its function? |
Wnt signaling regulates the bone mass Sclerostin is the inhibitor that will shut off bone formation (shut off Wnt signaling) If you have too much sclerostin, you get weak very thin bone. |
|
|
Overall, what are the 4 things you need to describe to fully name a fracture? |
1. Bone affected (with L/R) 2. Open v. closed 3. Location in the bone (meta, dia, epiphysis) 4. Fracture geometry (simple/communited) 5. Displacement of the distal segment |
|
|
If you have no obvious break in the skin but you are questioning if a fracture is open or closed, what is one thing you can look for that will tell you if you have an open fracture? |
Look for gas at the fracture site. If you have gas at the fracture site, you have an open fracture. |
|
|
Distinguish the difference between and how would you treat each of the following situations? Type 1 open fracture Type 2 open fracture Type 3 open fracture |
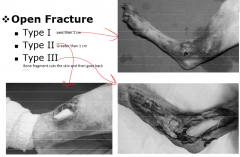
Type 1- open spot is less than 1cm in size, treat like a closed fracture Type 2- open spot is greater than 1cm. You can treat like an open or closed fracture depending on the tissue Type 3- You have major tissue loss, the fragment may have also pierced the skin and then went back into the body. Treat these as open wounds. Do not close, consider wound management before closing |
|
|
What is the goal of fracture stabilization? |
To provide temporary support, maintain functional rehabilitation and maintain proper anatomical position |
|
|
What is the definition of a simple fracture? |
Only two pieces at the fracture site |
|
|
Draw pictures/distinguish between a simple incomplete fracture and a simple, complete fracture |

(Simple incomplete = greenstick) |
|
|
What types of forces would result in the following fractures: Transverse Oblique (both short and long) Spiral (draw pictures demonstrating each fracture) |

Transverse = separation or pressure from the side Oblique and spiral = from torsion forces |
|
|
Define a comminuted fracture How are these fractures classified? |
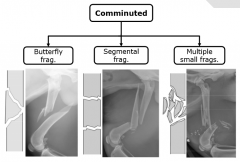
A fracture with more than two pieces at the fracture site Mild, moderate, severe |
|
|
Define and be able to identify a: Butterfly fragment fracture Segmental fragment fracture |
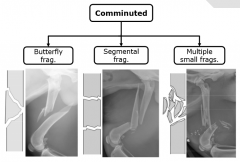
Butterfly- one intact cortex with a wedge shaped piece Segmental Fragment- fragment is 360 degrees |
|
|
What are the 3 ways you classify a fracture by the displacement of the distal segment?
|
1. Lateral/medial (movement L/R) 2. Cranial/Caudal (cr/cd in relation to the animal) 3. Proximal distal (closer/farther away from the rest of the limb) |
|

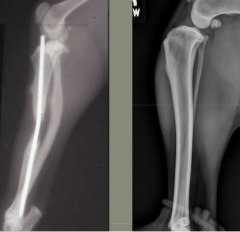
Classify this fracture |
Simple, incomplete (greenstick) fracture of the right mid-diaphyseal radius with a minor lateral displacement |
|

Classify this fracture |
Simple, complete transverse fracture of the left radial mid-diaphysis with a caudal displacement of the distal segment |
|

Classify this fracture |
Simple, complete short oblique fracture of the left tibial diaphysis with a cranial displacement of the distal segment |
|

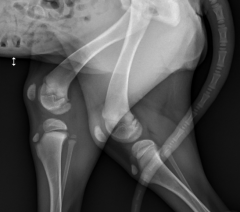
Classify this fracture |
This is a comminuted, long oblique fracture of the Right proximal ulna diaphysis with a cranial displacement of the distal segment (there is also a spiral fracture in the ulna right underneath the long oblique fracture) |
|

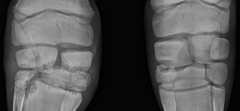
Classify this fracture |
This is a salter-Harris fracture type 1 of the right medial digit, proximal physis of the first phalanx |
|

Classify this fracture |
This is an open right Salter-Harris type II fracture of the distal femoral physis |
|

Classify this fracture |
This is a Salter-Harris Type III fracture of the capital physis and femoral head seen on the right limb |
|

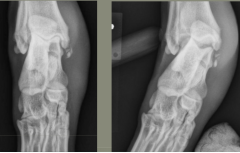
Classify this fracture |
This is a Salter-Harris Type 4 fracture of the left distal radial physis. |
|
Classify this fracture |
This is a Salter-Harris type 5 fracture of the right proximal tibial physis |
|
|
Define an avulsion fracture |
Fracture at the origin/insertion of a tendon, causing tension at the fracture site |
|
|
What is the relation between Kvp and contrast in imaging? |
Increase kVp, decrease contrast |
|
|
Describe the ranges of kVp and mAs that we use to radiograph bone |
68-80kVp 5-10+ mAs |
|
|
What are the three types of joints found in the body? |
Synovial Suture (flat bones, skull) Cartilaginous (Hyaline- physis, Fibrocartilagenous- pelvic/mandible) |
|
|
Describe the sesamoid bones found in the following locations Stifle Elbow Carpus Digits |
Stifle- fabelial (gastrocnemius), popliteal Elbow- supinator Carpus- abductor pollicis longus Digits- metocarpal/metatarso |
|

What disease process is seen in this joint? |
Osteoarthritis Look for deterioration of articular cartilage, periarticular bone formation, joint inflammation Seen on radiographs- osteophytes, joint narrowing and swelling |
|
|
Define and differentiate between intracapsular swelling and extracapsular swelling |
Intracapsular- the tissue on the inside of the joint is swollen. If you have swelling around the entire joint, you have intracapsular swelling. Extracapsular- the tissues outside the joint are swollen. If you have swelling that is eccentric around the joint, you have extracapsular swelling |
|

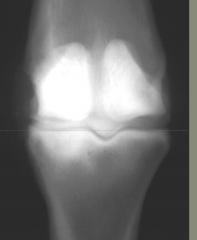
Describe the opacity seen between the femur and tibia |
This is a subchondral cyst seen in the joint area. |
|
On the right side of this fracture, what opacity is seen? |
This is an avulsion fragment, caused by the avulsion fracture |
|

The arrow is pointing to what? What causes this? |
This is an Enthesophyte. This is mineralization where a tendon inserts/originates, due to the damage of soft tissue around the joint. |
|
|
Name the 5 fracture forces |
Tension Compression Bending Shear Torsion |
|
|
What is the most common fracture force? Why is this important when talking about intermedullary implants? |
Bending You want to eliminate the bending force on implants by placing them where there is no bending force (usually in the center of the medullary cavity) |
|
|
Differentiate between Eccentric and Concentric loading |
Eccentric- there is a different spot of force on either side of the bone Concentric- the spot of force is the same on either side of the bone but the bone curves in between the two points |
|
|
In terms of fracture forces, what is the most important force on an IM pin? Why is this important when talking about placing one of these in the bone |
Bending (+++) Must be combined with other implants/stabilizers in order to combat this bending |
|
|
In order from most important to least, what are the fracture forces on an ILN? |
Bending (+++) Tension, Compression, Torsion (++) Shear (+) |
|
|
In order from most important to least, what are the fracture forces on a Plate? |
Tension, Compression (+++) Bending, shearing, torsion (++) |
|
|
In order from most important to least, what are the fracture forces on an ESF? |
Tension, Compression, Shear, Torsion (++) Bending (+) |
|
|
In order from most important to least, what are the fracture forces on a screw |
ALL forces (+) |
|
|
Why should you never stack pins together to fix a fracture? |
Because it is dangerous, it gets close to areas where it could potentially damage nerves |
|
|
What are some of the advantages and disadvantages of using a pin to fix a fracture |
Advantages: Minimal approaches, facilitates 2D alignment, preserves the periosteum, preserves the extramedullary blood supply Disadvantages: Interferes with the intramedullary blood supply and if the pin loosens, it can result in tissue damage |
|
|
Steinman pins: How would you want to put these in a bone? What can happen with a negative thread? what kind of bone can you put these in? The two different tips are called what? |
Across the bone, not at the end of the bone into the medullary cavity. It will fall out of the IM cavity. A negative thread is weak and can snap. Cortical and cancellous bone Trocard tip- for penetration and Chisel tip- for ricochet |
|
|
What is the ideal IM pin size if it is: Placed alone With a plate With an external fixator? |
75% of medullary cavity if alone 50% with an ESF 40% with a plate |
|
|
What are the two things you want to remember when placing a pin? |
Use short, high speed bursts to insert it. Too fast for too long can result in bone necrosis use proper hand control (with an index finger on top of your driver) |
|
|
Define Normograde fracture repair Retrograde fracture repair |
Normograde = from the end of the bone into the middle (from epiphysis to diaphysis) Retrograde = from the middle, where the fracture actually is and back out towards the end of the bone |
|
|
Describe how you would fix a humeral fracture with an IM pin? |
Use a Retrograde distal approach. Start where you want the pin to end up and drill from there as far as you can. Then reverse and do the other side. This helps get it into the medial condyle like you want. Normograde can be done but it is harder and you usually end up in the lateral condyle rather than the medial condyle. |
|
|
Describe how you would fix a radial fracture with an IM pin? |
You can't. Never pin the radius. |
|
|
Describe how you would fix a ulnar fracture with an IM pin? |
Use a normograde approach, use a pin and an ESF to properly fix |
|
|
Describe how you would fix a Femoral fracture with an IM pin? |
Normograde is preferred (retrograde has a higher chance of hitting the sciatic) Use a pin/plate combo, not an ESF (avoid puncturing through the muscle) You want to OVER reduce, make the pin very long and leave a slight gap in order to make the curved femur as straight as possible so the pin isn't bent. Dull the end of the pin so you don't go through the end of the bone. |
|
|
Describe how you would fix a tibial fracture with an IM pin? |
ONLY use normograde! Hyperflex the stifle to gain access to the tibia Avoid growth plates in young dogs |
|
|
Kirschner Wires How do you place them in a larger bone? What kinds of tips do these come with? What kind of situations would you use them in? |
Place them across the bone, putting them IM only has very little benefit. Double pointed or Trocard tip Avulsion fractures, Patellar luxation, as IM pins in toy breeds cats and birds, Mandibular and Metagrade fractures |
|
|
Cerclage wires: What type of fixation are they used in? What kind of integrity do they provide? They are used after what? |
Secondary Circumferential After anatomic reconstruction |
|
|
Describe the different knot types done with cerclage wires and what are their tension forces/loads to break of each of them |
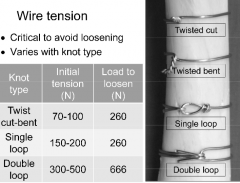
Twisted cut-bent: 70-100, 260 to loosen Single loop: 150-200, 260 to loosen Double loop: 300-500, 666 to loosen |
|
|
How are wires placed relative to the fracture plane? |
Perpendicular |
|
|
Describe the 3 rules and the 2 cautions when placing wires to fix a fracture |
rules 1. put at least 1/2 the bone from the edge to avoid tip fracturing the bone 2. Put at least two wires on (increase resistance to bending) 3. Put 1/2 lb between to increase stability and decrease disturbance Cautions 1. avoid tissue entrapment and 2. preserve blood supply |
|
|
Describe what a tension band is and what types of situations are they used in? |
Tension band = Kirschner and a Cerclage wire together. This turns tension forces into compression forces. Used in Avulsion fractures at apophyses Ostetomies at the greater tubercle, olecranon and the greater trochanter Patellar luxation at the tibial tuberosity |
|
|
Plates and screws eliminate damage to the bone by what 4 things? |
1. Eliminating anatomical reduction 2. Practicing indirect techniques 3. Aligning fragments axially 4. Flexible fixation, allowing indirect bone healing |
|
|
Screws are used in what two situations? |
1. Used to repair a fracture with interfragmentary compression 2. To fix a plate or nail to a bone |
|
|
What is the difference between cortex screws and cancellous screws? |
Cortex- for the diaphysis. Never exceed 40% of the diameter of the bone because the bone will be too weak Cancellous- larger outer diameter, larger pitch. Used for metaphysis and epiphysis in a bone |
|
|
How is the size (ex. 3.5mm) of a screw actually determined? |
The widest part of the pitch is the screw diameter. This is how a screw is named. |
|
|
Differentiate between a self-tapping screw and a non self-tapping screw |
Self-tapping can be screwed in once the pilot hole is dug Non self-tapping has to have a pilot hole and a tap has to be used in order to insert them in. Advantage to these though is that you can insert them and take them out multiple times without worry of creating a new pitch. |
|
|
When would a partially threaded screw be used? A fully threaded? |
Partially threaded are usually used as lag screws Fully threaded are used to fasten plates to bones |
|
|
Define a locking head screw |
They have a head that locks into a plate, making a compression plate. This makes the focus on the screw/plate interface and the screw usually doesn't work its way out However, they can break under the plate so these screws are usually larger in core diameter and have a smaller pitch |
|
|
Describe the steps one would take when placing a lag screw |
1. take a drill bit the same size as your screw and drill through the first cortex 2. take a drill bit one size smaller than your screw and drill through the second cortex 3. take a countersink and create a hole for the screw head to sit 4. measure the depth of the hole to get the right length screw 5. tap the inner cortex to give the screw somewhere to anchor into 6. place your screw Insert one lag screw in the middle of the fragment and another at a right angle to the fracture plane. |
|
|
Describe the steps taken when putting in a position screw When would these screws be used? |
These are used in a situation where a lag screw would result in a piece of bone breaking and ending in the bone. 1. while holding the fragment up, use a drill bit to put a hole in both sides of the cortex 2. tap the far side of the cortex to allow anchoring 3. Screw the screw in using a guide |
|
|
When would you use a plate screw? |
When putting a plate onto a bone |
|
|
Name the uses and how a dynamic compression plate is used |
Used for axial compression by eccentric screw insertion. Bone fragment moves relative to the plate One or two screws are placed on either side of the fracture Screws can be placed eccentrically (in compression) or in the center of a hole (not in compression) Can have up to 4 screws in compression |
|
|
What are some of the characteristics/advantages of using a limited contact dynamic compression plate? |
The area of the bone-plate contact is reduced It has a scalloped underside so there is more even stiffness and the contouring is easier |
|
|
Describe some of the general characteristics of a veterinary cuttable plate |
They are 300mm long, have 50 holes They are relatively weak and cannot be used for compression. Stacking them up on one another and using a plate-rod technique does help increase strength and combat some of the bending forces. |
|
|
Name some of the characteristics of a reconstruction plate |
They have deep notches between holes They allow for more complicated contouring of 3D fractures, as long as you have the right pliers |
|
|
What are some of the advantages of using a locking plate/internal fixator? |
The screw and plate can lock together Getting accurate contouring is not as important Blood supply is maintained better More versatility in using these plates |
|
|
What types of screws can you use with a Locking compression plate? |
You can use conventional and locking screws as one part of the hole is normal for conventional screws and the other part is threaded |
|
|
Plates are strongest when place on what side of the bone? What surfaces would you place a plate for the radius, tibia, femur, humerus and mandible? |
Whatever side is in tension loading Radius- cranial or craniomedial Tibia- medial Femur- lateral Humerus- cranial or lateral Mandible- occlusive surface |
|
|
If you were to place a plate on a fracture, what 4 rules would you want to follow? |
Place the plate as long as possible Place a minimum of 4 but ideally 5 screws above and below the fracture Place the screws away from the fracture site Distribute the forces on the plate over the length of the bone |
|
|
What are the 4 different modes you can place a plate in? |
Compression mode Neutralization mode Bridging mode Buttress mode |
|
|
How would you put a plate in compression? What types of fractures do you use them in? |
Contour the plate so it is 2mm above the fracture, then you get axial compression by the plate Used in simple transverse fractures |
|
|
A plate is in neutralization mode when used with what? What is the function of the plate in this situation? |
With a metaphyseal internal fixator Protects the interfragments from all shear, bending and other furces |
|
|
After you do indirect reduction of a fracture, what mode would your plate be in? What is its function in this case? |
Bridging mode Maintains bone length and prevents axial deformities by shear or bending forces |
|
|
In what mode would you use a plate to prevent the collapse of the articular surface of a metaphyseal fracture? |
Buttress mode |
|
|
When contouring a plate, where do you want to bend the plate? |
In between the holes |
|
|
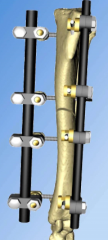
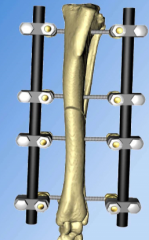
What is the type of external fixator used in the clinic? |
IMEX |
|
|
What are the two different threads on the screws of an external fixator? |
Cortical threads- better for anchoring into bone and better in smaller bones Cancellous threads- threads in the middle |
|
|
What are the three materials that make up the connection bars in an external fixator? Describe the pros and cons of each |
Carbon fiber- strong, radiolucent Titanium- strongest but most expensive *Both of these can be used more than once Aluminum- weak, corrosive Can only be used once |
|
|
What is the use of the clamp in an external fixator? What is the name of the link between the screw and the plate? |
Tighten the clamp, tighten the fracture Tight Stable Link |
|
|
Name 4 indications for an external fixator |
1. where there is less muscle 2. where the soft tissue is compromised 3. where there is an open fracture and/or wound care is needed 4. Where dynamization is needed |
|
|
What is dynamization? |
Where you make a complex frame with external fixators and then you slowly take pieces off to stimulate bone growth |
|
|
Distinguish between closed external fixator surgery and open? |
Closed- hanging leg technique done on the ulna, radius or tibia Open- When open reduction is needed |
|
|
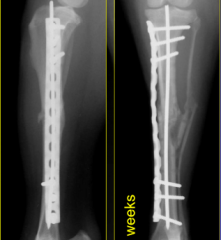
What is clinical union? Bony union? |
Clinical union- where there is enough cortex formed that the implant can be removed Bony union- where there is remodeling of the callus and the medullary cavity starts to re-form (farther along than clinical union) |
|
|
Why do you place release incisions in placement of external fixators? |
To eliminate tension on the skin and to prevent pin track infections |
|
|
How far do you want to place the clamps away from the incision when placing an external fixator? |
1cm Place them closest to the fracture to increase compliance of the clamp |
|
|
Describe how you want to place a pin when using an external fixator |
Pick a pin that is 25% of the diameter of the bone Pre-drill a hole for the pin that extends along 80% of the length of the skin Place the pin in the center, avoiding joints and growth plates Pins should be placed 1cm from the fracture Put 3 pins per segment of bone |
|
|
Describe some ways in which you can dynamize a fracture with an external fixator? |
1. take away pieces of the external fixator 2. move the external fixator farther away from the skin 3. Taking parts of the bandage off when appropriate |
|
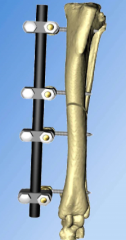
What type of fracture frame is this? What are the pros/cons? |
1A Weakest frame Least invasive |
|
What type of fracture frame is this? What are the pros/cons? |
1B Not very invasive, better mechanics |
|
What type of fracture frame is this? What are the pros/cons? |
2 Higher morbidity, not good for cranial/caudal bending Good for med/lateral bending |
|

What type of fracture frame is this? What are the pros/cons? |
3 Highest morbidity, most invasive *Use other alternatives, don't use this type of fix |
|
|
When placing a frame, what 3 precautions do you want to follow? |
1. It is better to trade some stability to increase the biological response of fracture healing 2. Preserve the joint and muscle function 3. Don't over fixate- this will increase morbidity and decrease healing |
|
|
Describe how you would bandage a limb after using an external fixator? |
On the pin/skin interface you want to use a sterile compression bandage to decrease skin motion and infection A Robert-Jones bandage goes around the entire fixator The bandages need to be changed at least once a day Take as much of the bandage off as soon as you can to promote motion |
|
|
If you have a healing fracture with no motion, what kind of callus do you get? |
A stress callus, a very slow growing callus |
|
|
What kind of follow-up do you recommend to a client who owns an animal with a new external fixator? |
Do immediate post-op radiographs to look at alignment Repeat the radiographs periodically, every time dynamization is increased Restrict activity |
|
|
How would you know when to remove an external fixator? |
When you see 3-4 cortices bridged by a callus (clinical union is achieved) on radiograph |
|
|
What complications can you have with the placement of an external fixator? |
Pin tract infections Morbidity in the proximal segments |
|
|
What are the 4As in fracture repair? |
Alignment Apposition/Adjacency Apparatus Activity |
|
|
What are the 4 different products available for interlocking nails? What are some of the uses/characteristics of each? |
1. Innovative animal products- sharp/blunt tip, locked with bolt and screw 2. Biomedtrix- IM fixator, angle stable nails- self-centering, eliminates slack, hourglass shaped 3. Small/Targon: small nails for cats 4. Aesdelap 2011- diameter of hole is 56% (too big, too many problems), special tools needed to place |
|
|
What are the advantages/disadvantages of using an interlocking nail? |
Advantages- the intramedullary rod counteracts bending, the locking bolts counteract compression and torsion. These also preserve the fracture hematoma and the fibrin bridges that are formed Disadvantages- Slack is present- meaning that there is more callus formed due to the movement of the bolt within the locking device |
|
|
What are some indications for using an interlocking nail? |
Used in humerus, ulna, femur and tibia (NOT in the radius) Used as an alternative to the plate/rod technique Revision surgeries Repair angular limb deformities |
|
|
When placing an interlocking nail, what are some of the steps that you have to do? |
Positioning Reduction with bone forceps Coupling- attach the alignment guide Fixation- drill, length, bolting, closure |
|
|
What are 3 common roles of external coaptation? |
1. Temporary support/first aid 2. Secondary support after surgery 3. Primary support in certain fractures |
|
|
What fracture forces are easily fixed with external coaptation? |
Bending and Rotation are easily fixed (compression/shear, difficult) |
|
|
What is the reduction rule? |
Reduction is needed in minimally displaced stable fractures Less than 50% reduction in the fracture, it will take much longer to heal and external coaptation may not be the best option |
|
|
Alignment of what needs to be maintained when using external coaptation? |
Proper joint alignment Can cause rotational/angular malunion and gait abnormalities if you don't |
|
|
What are two factors that must be true in order to properly use external coaptation |
Normal standing conformation and weight bearing must occur Joints above and below the fracture must be immobilized |
|
|
Explain why external coaptation is used for pancarpal Arthrodesis |
Fix of the palmar fibrocartilage rupture is a plate that is constant under compression and can break. So, external coaptation is used to reduce these stresses. (place external coaptation 3-5 days after surgery) |
|
|
Describe the different types of external coapation |
Robert Jones- cotton padding w/ hard casting material Modified RJ- less cotton padding Reinforced bandage- splint Full leg/partial leg cast Bivalved- allowing frequent changes without new materials Walking bar- aluminum bar at the end |
|
|
Describe the different layers of an external coaptation bandage |
primary- cover, protect the skin and absorbs discharge Secondary- support, apply pressure and absorption. Can use cotton role of cast padding Layer of conforming gauze for stability Layer of casting tape tertiary- holds other layers together, will become tighter when wet. Elastic conforming bandage most common |
|
|
The two categories that can cause aggressive bone lesions are |
Neoplasia Osteomyelitis Distinguishing between the two can be difficult with radiography alone |
|
|
What are some things that can cause benign bone lesions? |
Bone cysts Healing/healed fractures Osteochondrosis Arthritis |
|
|
Describe the difference in aggressive and benign when looking at periosteal proliferation |
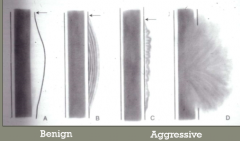
Benign- smooth, laminar (onion) Malignant- lacey, sunburst |
|
|
Describe the difference in aggressive and benign when looking at pattern of lysis |
Geographic- benign (well-confined) Moth-eaten/permeative- malignant (not well defined/discrete) |
|
|
How much bone must be lost before you can see it on a radiograph? |
30-50% |
|
|
Describe the difference in aggressive and benign when looking at zone of transition |
Benign- abrupt change Malignant- not abrupt change |
|
|
What are all of the things you look at to determine if a bone lesion is benign or malignant? |
Periosteal proliferation Pattern of lysis Zone of transition Change over time Number of bones affected |
|

If this was a young large breed dog from WI, what disease would you be worried about with this seen on the radiograph? |
Fungal Osteomyelitis caused by blast/coccidiomycoses Can show up in more than one bone because it spreads through the blood |
|

Describe what is seen here in this radiograph. Knowing that there was just a plate removed in this area, what could this lesion be caused by? |
Bacterial osteomyelitis (caused by direct puncture, bone implants or spread from other tissues) Aggressive periosteal response, permeative lysis, extreme tissue swelling (Hematogenous spread is only found in foals) |
|

What lesion is seen in this bone (general category). What types are common in bone? |
Bone neoplasia- osteosarcoma, chondrosarcoma or fibrosarcoma. Found usually in the metaphysis first of those bones that are "away from the elbow, toward the knee" If it is a metastasis to the bone, it is usually near the nutrient foramen |
|
|
In 1989, many advances were made toward the healing of fractures. Describe 4 of the important ones. |
1. More compliant stability is better than rigid stability 2. realignment is better than complete reduction 3. PRESERVE the fracture hematoma! 4. Use bridging plates rather than neutralization plates for repair |
|
|
What does MIO stand for? What are some of the pros of using this technique over some of the others? What bones can it be used in? What is its primary goals? |
Minimally invasive osteosynthesis Indirect reduction, restores alignment, remote and small incisions are made, you get epi-periosteal plating Can be used in all long bones Goal to promote bone healing and promote full recovery |
|
|
Dr. Dejardin's favorite technique to fix a fracture is... |
ILN |
|
|
What is different about the fracture callus formed in young dogs when compared to adult dogs? What are young dog fractures susceptible to? |
Exuberant callus is formed. If too close to the joint, this can lead to decreased joint function Normal plates are susceptible to failing by screw pullout |
|
|
What does EPO stand for? What is its goal? What are some of the pros of using it? How do you apply one? |
Elastic Plate Osteosynthesis Promotes construct of elastic deformation, decreass plate stiffness, increases plate working length Alignment is the goal, NOT reduction- the motion will help heal, gain clinical union in about 2wks |
|
|
Why are articular fractures associated with such high morbidity rates? |
Because they're difficult to manage and there is often more fracture than what the original radiograph shows. (you often have muscle, ligament and tendon involvement, meniscus, blood supply, etc. may all be involved) |
|
|
What are the 6 important steps to fixing an articular fracture? |
1. Accurate diagnosis 2. Treat early 3. Perform surgery for anatomical reduction 4. Use rigid fixation to correct fracture 5. Restore the functional axis of the fracture 6. Post-op rehab and care q |
|
|
How do you go about getting an accurate diagnosis for an articular fracture? |
use stress radiographs to look at the whole joint Use CT or other advanced imaging to make the best surgery plan |
|
|
Define Varus and Valgus |
Valgus- go away from the sagittal plane Varus- going toward the sagittal plane |
|
|
Why is it important that you treat an articular fracture early? |
the pieces in the fracture are sharp and can induce more damage the longer you wait. Also, the earlier the intervention is, the less pain the animal is in, the less ST contraction you get and the less morbidity associated with that fracture |
|
|
Why is it important to be as atraumatic as possible when correcting an articular fracture? |
You want to reduce the ST damage. Example, you can do an osteotomy to look at the surgical site better but this induces damage and many times, you get increased complications. |
|
|
When can you use MIO to correct an articular fracture? |
When the fracture is relatively fresh and the fracture is minimally displaced |
|
|
Can you use an EPO to correct an articular fracture? |
No. You want to use RIGID stabilization only. |
|
|
How would you go about making sure the functional axis is restored in an articular fracture? |
Use a special plate, LCP, or ILN if needed |
|
|
When should rehab start for an animal that underwent surgery to fix an articular fracture? |
As soon as it's tolerated and pain free for that animal |
|
|
What should you do if you see movement of the implant on post-op radiographs of an animal that underwent surgery to fix an articular cartilage fracture a month ago? |
Go back to surgery- movement of the implant suggests movement in the joint meaning that this joint is not properly healing. |
|
Is this a benign or aggressive bone response? |
Benign- this is an adaptive reaction to stress in the bone (Wolff's Law) |
|
What kind of bone response is seen here? |
Sclerosis, this is a benign change in bone, common with osteoarthritis |
|
What type of disease is seen in this picture? What are some possible causes? |
Aggressive joint disease of the bone *note the lysis of the articular margins of multiple bones in this area Causes- infection- septic arthritis, Rheumatoid arthritis, joint neoplasia (synovial cell carcinoma or histiocytic sarcoma) |
|
|
What types of things do you want to look at when evaluating the soft tissue around a bone lesion? |
Look for swelling, usually centered at the pathology, look for disuse atrophy Look for evidence of an open fracture or abscess Look for increased opacity- avulsion fractures, mineralization, foreign bodies, debris |
|
|
What is the principle behind ultrasound? What terminology do you use? |
The transducer emits sound waves that hit the object and then return to the tranducer emiting an image You get a cross-section of anatomy Echogenicity- hyperechoic- more black. Hypoehoic- more white. |
|
|
What are some of the indications for using ultrasound? Limitations? Advantages/Disadvantages? |
Equine distal limb, small animal orthopedics Can't use for air or bone Available, no radiation, no sedation, inexpensive Operator dependent, experience, hair has to be wet down or clipped |
|
|
What is the principle behind CT? Terminology used? |
X-ray tube spins around, emits a fan of rays and emits a slice image of the patient Attenuation. Hyperattenuating- more black. Hypoattenuating- more white |
|
|
What are some of the indications for using CT? Advantages/Disadvantages? |
Trauma (both bone and tissue), best for acute hemorrhage, developmental disease, neoplasia Best for bone, thin slices, fast, 3D image reconstruction Expensive, anesthesia required, not great for soft tissue, radiation used |
|
|
What is the basis of an MRI? What terminology do you use? |
Magnet makes a cross section of the patient, the H2O in the body is stimulated to give off radio waves. Intensity- hyperintense (more black), hypointense (more white) |
|
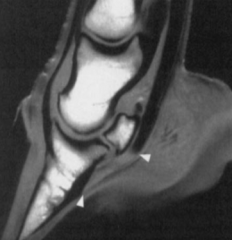
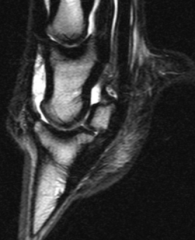
What type of MRI image is this? What are some of the advantages of this type? |
T1 weighted Fluid is dark, good detail (you do get artifacts on tendons, arrows) |
|
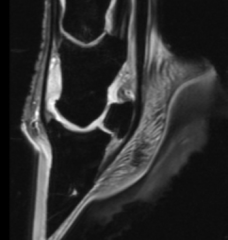
What type of MRI image is this? What are some of the advantages of this type? |
T2 weighted Fluid and inflammation is bright, great for pathology |
|
What type of MRI image is this? What are some of the advantages of this type? |
STIR sequence, fat suppressed Bone marrow dark, shows fluid within the bone, good for bone pathology |
|
|
What are some of the indications of using an MRI? Advantages? Disadvantages? |
Soft tissue imaging that can't be reached with ultrasound, cartilage, Soft tissue imaging, tumor evaluation, neurologic cases No radiation, different planes of tissue, great soft tissue detail Very expensive, anesthesia needed, motion screws up the image, detail not as good, can't do a nose-tail image, not safe |