![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
126 Cards in this Set
- Front
- Back
|
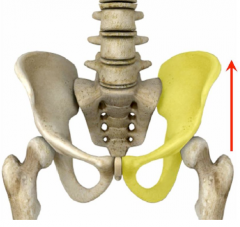
Seated Flexion / Forward Bending Test |
Evaluate mobility of sacrum on ilium (Sacroiliac) Pt sits with feet supported on ground .Ischia stabilized on table. Palpate PSIS as pt bends forward Side that moves first or most superiorly is the Hypomobile side |
|
|
A Patient is found to be hypomobile on the Right side during a seated forward flexion test. What Axis is hypomobile? |
Left Oblique Axis (LOA) |
|
|
Sacroiliac joint The Ilium is Con____ and the Sacrum is Con____ |
Ilium is Convex, Sacrum is Concave Movement is vex on cave but motion is not conventional and is very minimal |
|
|
In infants, the sacroiliac joint is ____. |
Planar. Ridges and bumps develop throughout lifespan increasing the irregularity and decreasing motion at this joint |
|
|
What level of inequality in palpation of the ASIS and PSIS is considered pathological? |
Greater than 1 cm Reports Pain! |
|
|
Sacrococcygeal Joint |
Cartilagenous May fuse with age Passive Flexion and Extension motions |
|
|
Symphysis Pubis |
Articular cartilagenous joint with interpubic disc Resists compressive forces |
|
|
Nutation |
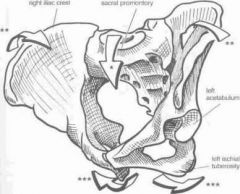
Sacral Flexion: Base moves anterior, Pelvic Rim Reduced, Pelvic Outlet Increased FORM CLOSURE |
|
|
Counternutation |
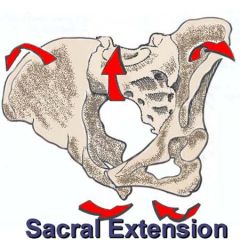
Sacral Extension: Base moves posterior, Pelvic Rim Increased, Pelvic Outlet Recduced |
|
|
Gait causes asymmetrical shear forces through the SIJ but will put more force through ____. |
The pubic symphysis. |
|
|
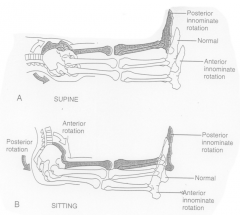
Hip Flexion causes _____ Innominate Rotation |
Posterior Innominate Rotation |
|
|
Hip Extension causes _______ Innominate Rotation |
Anterior Innominate Rotation |
|
|
Standing Forward Bendings will cause Sacral ______ and ______ Pelvic Tilt |
Sacral Nutation and Anterior Pelvic Tilt End range in full flexion may cause counternutation |
|
|
SI Belts use compression to induce ______ Closure |
Form Closure |
|
|
Form Closure |
State of pelvic stability that is dependent on anatomy (**Passive Stability) Articular surfaces, friction, and sacral wedging Integrity of the ligaments |
|
|
Force Closure |
State of pelvic stability dependent on muscular contraction and coordination (**Active Stability) Pelvic Floor, Transverse Abdominis, Multfidus, Gluteus Max, and Diaphragm |
|
|
Hamstring tightness may cause ____ Pelvic Tilt |
Posterior Pelvic Tilt |
|
|
Tight Hip Flexors may cause _____ Pelvic Tilt |
Anterior Pelvic Tilt |
|
|
What symptom presentations would lead you to believe a patient has a SIJ pathology? |
Sharp pain localized over SI Pain refers to buttock but not below knee or into low back Discomfort with most activities Pain is usually Unilateral No neurological symptoms |
|
|
Testing reveals Hypomobility in the Right SI joint but the patient reports pain in the Left. Why? |
The Left is hypermobile to compensate for the hypomobile joint. the hypermobility causes more pain than the other side **Patient Education |
|
|
Ankylosing Spondylitis "Bamboo Spine" |
Males <35 yo Progressive ossification of ligamentous and joint capsule tissues in the spine **Begins in the SIJ with Bilateral Pain (Diff Dx) Dx with X-ray and bloodmarker tests HLA-B27 Treat with ROM exercises into spinal extension Rib Dysfunction can cause reduced lung capacity |
|
|
Systemic Differential Diagnoses for SIJ Pain? |
Metastases from the Breast, Lung, or Prostate Rheumatoid Arthritis Psoriatic Arthritis (Psoriasis - Skin Lesions) Chrohn's Disease Visceral Pain Referral (Colon, rectum, bladder, prostate, urethra) |
|
|
Sign of the Buttock |
Serious pathology present posterior to the axis of flexion / extension of the hip Restricted passive unilateral SLR, PT flexes the knee to slack the hamstrings and rechecks hip flexion, **Positive: Hip Flexion does not increase with knee flexed** Immediate referral to MD!!! |
|
|
Coccydynia |
Injury to the coccyx resulting from childbirth or trauma (fall) Movement issues with walking uphill or upstairs, sitting, defecating, coitus |
|
|
Possible Causes of Sign of the Buttock |
Osteomyelitis, Infectious sacroilitis, Fracture of the sacrum or pelvis, Septic Bursitis, ischiorectal abscess, gluteal hematoma, gluteal tumor, and rheumatic bursitis |
|
|
Sacrotuberous Ligament |
PSIS to Ischial Tuberosity Limits Nutation |
|
|
Sacrospinous Ligament |
Side of Sacrum to the Ischial Spine Limits Nutation |
|
|
True Leg Length Discrepency |
Structural Bony difference in the leg lengths Measure ASIS to Medial Malleolus |
|
|
How do you clear the Lumbar Spine and Hip before evaluating SIJ? |
Active ROM and overpressure Lumbar spine: Flexion, Extension, Side Bending, and Rotation Hip: Flexion, Internal Rotation, and External Rotation |
|
|
Functional Leg Length Discrepency |
Alteration of hip innominate rotation Measure from Umbilicus to Medial Malleolus |
|
|
To Functionally Lengthen a shortened limb a patient may: |
Anterior Pelvic Tilt Hip Depression, Extension, and Lateral Rotation Knee Extension Foot Supination |
|
|
To Functionally Shorten a lengthened limb a patient may: |
Posterior Pelvic Tilt Hip hiking, medial rotation, and flexion Knee Flexion Foot Prontation |
|
|
Describe a Piriformis Stretch |

Do a figure 4 stretch and bring the knee on top towards your opposite shoulder |
|
|
The Oblique axes of Sacral motion are named for... |
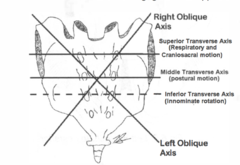
The corner of the Sacral Base that they pass through **Sacral base is the Superior Border of the sarum |
|
|
Nutation and Counternutation happen around which axis? |
Transverse Axis of the Sacrum |
|
|
Sacroiliac Joint and Pelvic Testing fall into 3 general categories: |
1. Static Alignment (Palpation of PSIS, ASIS, and Pubic Tubercles) 2. Dynamic Mobility Tests (Flexion and Gillet) 3. Pain Provocation (Laslett 5) **In this order |
|
|
What are the Laslett 5 Pain Provocation Tests? |
Distraction Compression Thigh Thrust Sacral Thrust Gaenslen's Torsion Must be positive on at least 3 out of 5 to be positive for SIJ Dysfunction Must Rule out lumbar through McKenzie Repeated Motions |
|
|
SIJ Distraction Test |
Pt is supine as therapist pushes the ASIS's apart with crossed arms Distracts the Anterior Aspect of the SIJ (Compresses posterior aspect) Targets Anterior Ligaments |
|
|
SIJ Compression Test |
Pt is sidelying or supine as the therapist pushes the ilia together Compresses the Anterior structures of the SIJ Targets Posterior Ligaments |
|
|
Thigh Thrust Test |
Pt Supine, Hip flexed to 90°, therapist hand stabilizes sacrum, vertical force is applied through the femur Produces Shear force of ilium on sacrum |
|
|
Gaenslen's |

Produces Sacral Torsion Posterior Rotation at Flexed Hip Anterior Rotation at Hanging Leg |
|
|
Sacral Thrust |
Pt is prone while therapist applies a vertical P-A force on the midline of the sacrum Produces Anterior Shearing of Sacrum on both Ilia |
|
|
FABER Test / Patrick's Test |
Flexion Abduction External Rotation of hip Lateral Malleolus on opposite knee. Opposite ASIS stabilized and down pressure on knee of side to be tested Similar to SIJ Distraction test but catch all for hip as well |
|
|
Resisted Hip Abduction Test |
SIJ Pain Provocation Test (**Good for Hip and Knee TKR Patients) Stresses cephalic aspect of the SIJ Pt can be supine or sidelying as PT resists the hip abduction to ~30° Leg acts as a long lever |
|
|
Active Straight Leg Test |
SIJ Pain Provocation Test Weight of leg causes torsion load on the pelvis Scored from 0 to 5 (unable to perform) Identifies severity of posterior pelvic pain after pregnancy Use to Differentiate between Form and Force closure issues |
|
|
How do you confirm Form Closure issue with SIJ testing? |
Manually Stabilize pelvis or have patient wear an SI belt during the Active SLR If this eliminates symptoms, we can confirm that it is a Form Closure instability causing SI Pain |
|
|
How do you confirm Force Closure issue with SIJ testing? |
Have patient contract TA, Butt, and Pelvic Floor while performing ASLR If this eliminates symptoms, we can confirm that it is a Force Closure instability causing SI pain |
|
|
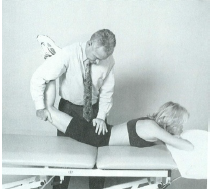
Standing Forward Fold Test |
Iliosacral Motion: Ilium on Sacrum *Must normalize leg length difference first Therapist palpates PSIS and asks pt to bend forward The PSIS that moves first or furthest superior is the Hypomobile Side |
|
|
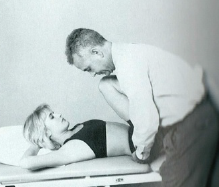
Gillet Test (March Test) |
Iliosacral Motion: Ilium on Sacrum (Open Chain) Therapist palpates PSIS and S2 then asks pt to raise knee flexing hip Normal: PSIS moves inferior with posterior tilt Hypomobile: PSIS does not move inferior or moves superior with hip hiking |
|
|
Seated Forward Flexion Test |
Sacroiliac Motion: Sacrum on Ilia Ischia stabilized on table and feet stabilized on floor Therapist palpates PSIS and asks patient to bend forward The PSIS that moves first or furthest superior is the Hypomobile Side |
|
|
Palpation: Right PSIS is higher than Left PSIS Left ASIS is Higher than Right ASIS Standing Forward Flexion: Right is Hypomobile Name the rotation. |
Right Anterior Rotation |
|
|
Supine to Sit Test |
Assess Leg Length Discrepancy Ant Rot: Long in supine and short in sitting Post Rot: Short in supine and long in sit |
|
|
Forward Flexion Test: Hypomobile on Left Palpation: Left Sulcus is Shallower or more posterior than Right Name the Torsion. |
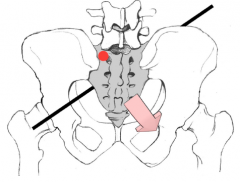
L on R Sacral Torsion Left Facing on R Oblique Axis Axis opposite Hypomobility |
|
|
Forward Flexion Test: Hypomobile on Left Palpation: Left Sulcus is Deeper or more Anterior than Right Name the Torsion. |
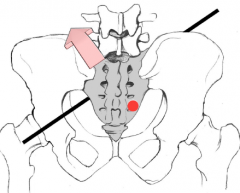
R on R Sacral Torsion Right Facing on R Oblique Axis Axis opposite Hypomobility |
|
|
Forward Flexion Test: Hypomobile on the Right Palpation: Right Sulcus is Shallower or more posterior than Left Name the Torsion. |
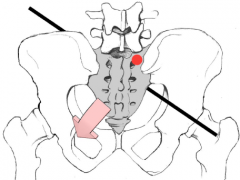
R on L Sacral Torsion Right Facing on L Oblique Axis Axis opposite Hypomobility |
|
|
Forward Flexion Test: Hypomobile on the Right Palpation: Right Sulcus is Deeper or more anterior than Left
Name the Torsion. |
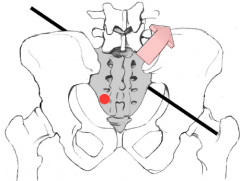
L on L Sacral Torsion
Left Facing on L Oblique Axis
Axis opposite Hypomobility |
|
|
Ilio-Sacral Upslip |
Large force through entire LE Length Discrepancy and Palpation all superior Use Gillet Test to name side |
|
|
How do you name Sacral Torsion? |
The way the Sacrum is facing and The Axis it is stuck on Ex. Right Facing Sacrum on a Left Oblique Axis "R on L Torsion" |
|
|
What is the Sequence of Treatment for an SIJ Dysfunction? |
Soft Tissue (Glute Max and Piriformis) Lumbar Spine Hip Pubis (Shotgun Manipulation) Sacrum Ilium Neuromuscular Re-Education and HEP |
|
|
Clinical Prediction Rules for General Lumbar Spine Manipulation |
<16 days No Symptoms Distal to Knee Lumbar hypomobility >35° IR on at least one hip Low Fear Avoidance score |
|
|
Pubic "Shotgun" Mobilization |
Aims to reverse the origin and insertion of the adductors to distract the pubic tubercles and realign them 1. Resist hip abduction to turn off those muscles 2. PT puts forearm between pt knees to resist bilateral adduction 3. Pubic symphysis may cavitate |
|
|
How would you mobilize a L on L sacral torsion? |
Grades I - IV, P to A mobilization,on most superficial aspect Left Inferior Lateral Angle |
|
|
How would you mobilize a L on R sacral torsion? |
Grades I-IV, P to A mobilization,on most superficial aspect Left Sacral Base |
|
|
How would you mobilize a R on L sacral torsion? |
Grades I-IV, P to A mobilization, on most superficial aspect Right Sacral Base |
|
|
How would you mobilize a R on R sacral torsion? |
Grades I-IV, P to A mobilization, on most superficial aspect Right Inferior Lateral Angle |
|
|
Muscle Energy |

Using a voluntary muscle contraction to enhance a mobilization Ex. Mobilizing into Anterior Rotation of the innominate using a quad contraction |
|
|
Ilia Mobilizations to Correct a Posterior Innominate Rotation |
Or the Gaenslen's Muscle Energy mobiliazation Or manually rotating innominate at ASIS and PSIS |
|
|
Ilia Mobilizations to Correct an Anterior Innominate Rotation |
Or manually rotating innominate at ASIS and PSIS |
|
|
Ilial Up-Slip intervention |
SI manipulation Similar to hip distraction manipulation but in closed pack position (IR and ADduction) |
|
|
Froggy Exercise |
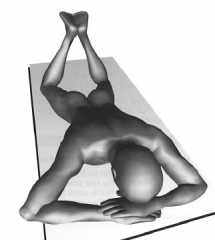
-Excellent SI and Core strengthening exercise -External rotators, Hip extensors, TA, and Pelvic Floor |
|
|
Demifacet |
Rib facets on the vertebral bodies and transverse processes |
|
|
The Facets of the Thoracic Spine facilitate what motions? |
Rotation and Side Bending Mostly vertical facet orientation |
|
|
Costosternal Articulations
Ribs 1, 6, and 7 |
Synchondrosis |
|
|
Costosternal Articulations Ribs 7-10 |
Common Band of Cartilage |
|
|
Costosternal Articulations Ribs 2-5 |
Synovial Joints |
|
|
Costosternal Articulations Ribs 11 and 12 |
No anterior cartilaginous articulation "Floating" |
|
|
Costovertebral Joints |
Ribs connect to 2 adjacent vertebral bodies with hyalinated and synovial joints |
|
|
Costotransverse Joints |
Synovial joint between the posterior neck of the rib and the anterior aspect of the transverse process Stabilized by the costotransverse ligament |
|
|
Normal ROM in the Thoracic Spine |
Limited! by Ribs and orientation of the spinous processes and the facets Flexion 30-40° Extension 20-25° *Less extension than flexion Rotation 30-35° *Limited by Ribs Sidebending 20-25° |
|
|
Fryettes 1st law in the thoracic spine |
Sidebending and rotation happen in opposite directions |
|
|
Pump Handle Rib Motion |
Ribs 1-6 Pulls Sternum anterior and superior Increases A-P Diameter |
|
|
Bucket Handle Rib Motion |
Ribs 7-10 Pulls ribs up and out Increases Lateral Diameter |
|
|
Caliper Rib Motion |
Ribs 11 and 12 Ribs open out Increases Lateral Diameter Prone: Ribs move posterior with inhalation |
|
|
Thoracic Spine Rule of Threes T1-3 |
Spinous Processes are on the same level as the Transverse Processes |
|
|
Thoracic Spine Rule of Threes T4-6 |
Spinous Processes are a 1/2 level below their transverse processes |
|
|
Thoracic Spine Rule of Threes T7-9 |
Spinous Processes are a full level below their Transverse Processes |
|
|
Thoracic Rule of Threes T10-12 |
T10 SP is one full segment below TP T11 SP is 1/2 segment below TP T12 SP is at the same level as TP **Transitioning to Lumbar |
|
|
Kyphotic posture |
Gradual Progression Increased posterior curve of thoracic spine due to chronic posture and degeneration |
|
|
Gibbus or Hump Back |
Sudden onset due to Anterior Vertebral Body Fracture Wedging (Pelvis not affected) Sharp Posterior angulation of Mid to Lower Thoracic Spine *Lower than Dowager's |
|
|
Dowager's Hump |
Sudden onset due to Anterior Vertebral Body Fracture Wedging *Postmenopausal Osteoporosis (Pelvis not affected) Sharp Posterior Angulation of Upper to Middle Thoracic Spine *Higher than Gibbus |
|
|
Functional Scoliosis |
Caused by soft tissue dysfunctions Lateral Shift due to pain, nerve root irritation, or inflammation Can be caused by contracture, muscle spasm, or leg length discrepency |
|
|
Structural Scoliosis |
Bony deformity Vertebral body is rotated towards the convexity while the spinous process points towards the concavity Diagnosed with Cobb angle Shoulders and Pelvis will be level in scoliosis |
|
|
How can you differentiate Functional and Structural Scoliosis? |
During a forward flexion, patients with structural scoliosis will have a rib hump on one side due to the vertebral rotation but functional scoliosis will not |
|
|
In Idiopathic scoliosis, the Spinous Process points towards the _____ while the vertebral body rotates towards the _______. |
Spinous process towards Concavity Vertebral Body towards Convexity |
|
|
How is scoliosis named? |
Named by the Direction of the Convexity and the Location of the Apex Ex. Right Thoracic Curve |
|
|
Cobb Angle |
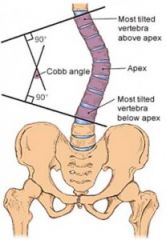
Parallel lines are drawn from the most superior and most inferior vertebral bodies and then a perpendicular line is drawn -The angle between that intersection is the Cobb angle |
|
|
Clinical Measure of Scoliosis Grouping and Prognosis |
Groups 1 + 2 are usually asymptomatic (<30°) Greater than group 3 will progress and should be braced Curves 30-50° will progress 10-15° lifetime Curves >50° progress 1° per year Curves >100° = life threatening Pulmonary complications |
|
|
Pectus Excavatum |
Indentation of the Sternum |
|
|
Pectus Carinatum |
Projection of the Sternum |
|
|
"Barrel Chested" |
Over inflated appearance of the rib cage indicative of pulmonary issues Check RR, Finger clubbing, and lung sounds as well |
|
|
Cafe au lait spots |
May indicate neurofibromatosis or collagen disease >3 cm or >6 in number |
|
|
Fawn's Patch |
Patch of hair along the spine that may indicate Spina Bifida |
|
|
What is peripheralization like in Thoracic Radiculopathy? |
Parasthesia spreading posterior to anterior along the ribs in a Dermatome pattern |
|
|
Fryette's 1st Law |
Neutral Spine: Sidebending to one side causes rotation towards the opposite side |
|
|
Fryette's 2nd Law |
Non-Neutral Spine (Flexed or Extended): Sidebending to one side causes rotation towards the same side |
|
|
Fryette's 3rd Law |
Introducing motion in one plane of motion restricts motion in other planes of motion |
|
|
Thoracic Outlet Syndrome Special Tests |
Roo's Test Adson's Test for Scalene's Pectoralis Minor Test Costoclavicular Test |
|
|
What might cause Thoracic Outlet Syndrome? |
Cervical Rib Elevated First Rib Tight Anterior or Middle Scalene Tight Pectoralis Minor Restricted Costoclavicular space |
|
|
What is Thoracic Outlet Syndrome? |
Upper Extremity parasthesias due to and impingement of the Neurovascular Bundle **Independent of any Cervical Spine pathology Pain, tingling, or fatigue with overhead positions May think it is circulatory problem b/c of tingling |
|
|
Roo's Test |
Thoracic Outlet Syndrome - General Test Abduct shoulders to 90° and flex elbows to 90° and retract scapula - "Goal Post" arms and open and close hands for 3 minutes (+) if Hands blanch AND symptoms reproduced |
|
|
Adson's Test |
Thoracic Outlet Syndrome - Anterior and Middle Scalene muscles Th finds radial pulse as pt extends neck and rotates towards side being tested and takes a deep breath and holds it (+) if loss of pulse AND symptoms reproduced |
|
|
Pectoralis Minor Test |
Thoracic Outlet Syndrome th finds radial pulse and passively elevates the shoulder with the nonpalpating arm while the pt retracts their shoulder and exhales completely (+) if loss of pulse AND symptoms reproduced |
|
|
Costoclavicular Test |
Thoracic Outlet Syndrome th finds radial pulse and pt sits in an exaggerated military posture to compress costoclavicular space (+) if loss of pulse AND symptoms reproduced |
|
|
Costochondritis (Tietze's syndrome) |
Inflammation of the junctions where ribs meet the sternum Causes localized chest pain that will go away with time and without treatment **Patient will be fearful of an MI |
|
|
Exhalation Restriction |
Elevated Rib Key Rib is the Bottom of the group |
|
|
Inhalation Restriction |
Depressed Rib Key Rib is the Top of the group |
|
|
Cervical Rotation Lateral Flexion Test |
Therapist passively rotates head and then laterally flexes the head in the opposite direction (+) if restricted ROM Side Opposite rotation is the side being tested |
|
|
Upper Limb Tension Test #1 (ULTT1) |
Median Nerve Bias -Scapular depression -Shoulder Abduction -Forearm Supination -Wrist and finger Extension -Shoulder laterally rotated -Elbow Extension |
|
|
Upper Limb Tension Test #2 (ULTT2) |
Radial Nerve Bias -Scapular depression -Elbow extension -Medial rotation of whole arm -Forearm pronation -Wrist and finger flexion -Shoulder abduction |
|
|
Upper Limb Tension Test #3 (ULTT3) |
Ulnar Nerve Bias -Scapular depression -Elbow flexion -Wrist and finger extension -Forearm pronation -Lateral Rotation at the shoulder -Shoulder Abduction |
|
|
Sensitizing Motions of the Upper Limb Tension Tests |
Cervical Sidebending Contralateral = Worse Ipsilateral = Relief |
|
|
1st Rib Mobilization |
pt in supine Find the first rib and follow it down with the pt exhalation and sidebend head in direction of mobilization |
|
|
1st Rib Manipulation |
Pt sitting with unaffected side propped on therapists knee Therapist passively sidebends the pt head towards rib and rotates away Thrust is applied to first rib towards opposite thigh |
|
|
Self 1st Rib Manipulation |
Hold towel under left axilla and drape over right shoulder. Pull towel taut and side bend head to the right taking up the slack as you go. Feel stretch as you bring head to neutral |
|
|
Upper Limb Nerve Tension treatment |
Can be In-Tension (Symptoms are provoked) or Out-of-Tension (No symptom reproduction) "Flossing" |
|
|
Scheuermann's Disease |
Most common in pubescent athletes Defect of the apophysis of the vertebral body and anterior wedging of the affected vertebrae as a result of flexion overload. End plate can crack causing a Schmorl's node Evidence of kyphosis and pain with thoracic extension or rotation |