![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
Pain described as "Cramping and Aching" could be indicative of ... |
Muscle pathology |
|
|
Pain described as "Sharp, Shooting, Numbness, and Tingling" could be indicative of ... |
Nerve Root Pathology |
|
|
Pain described as "Sharp, Bright, Electric, Numbness, and Tingling" could be indicative of ... |
Peripheral Nerve Pathology |
|
|
Pain described as "Deep, Nagging, and Dull" could be indicative of ... |
Bone Pathology |
|
|
Pain described as " Throbbing and Diffuse" could be indicative of ... |
Vascular Pathology |
|
|
How is Radicular Pain different from Referred Pain? |
Radicular Pain follows a dermatomal pattern and usually travels distal to the site of compression. Referred pain is related to neurological "wiring" and presents away from the site of pathology but does not follow a dermatome and may be proximal. |
|
|
What should be last in your examination and why? |
Palpation and Special tests because they are meant to localize and reproduce painful symptoms. |
|
|
Pain before Resistance |
Acute |
|
|
Pain at Resistance |
Subacute |
|
|
Pain after Resistance |
Chronic |
|
|
Elasticity |
The ability of a material to return to its original length after the removal of force |
|
|
Plasticity |
Property of a material demonstrated by remaining permanently deformed after the removal of force |
|
|
Viscosity |
Extent to which a material resists deformation during loading (Cold Molasses) |
|
|
Viscoelasticity |
Extent to which a material resists deformation during loading but returns to its original shape during unloading (Silly Putty) |
|
|
Arthrokinematics Convex on Concave |
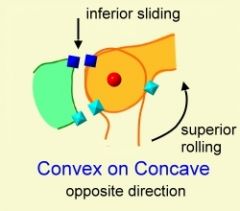
Roll and Glide go in opposite directions |
|
|
Arthrokinematics Concave on Convex |
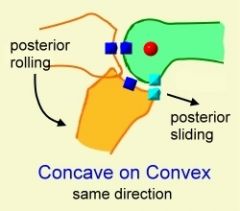
Roll and Glide go in the same direction |
|
|
Wolffs Law |
Internal architecture of bone is remodeled in response to external stress |
|
|
Bone response to immobilization |
-69% reduction in stiffness after 8 weeks of immobilization -Bone atrophy most notably in the cortical bone **Bones are more brittle and at greater risk of fracture after immobilization |
|
|
Bone response to aging |
-Loss of density (osteoporosis) -Osteoclast activity > Osteoblast -50% decrease in Strain Resistance **Greater fragility and risk of fracture |
|
|
Bone fracture type Tension |
Transverse Fracture |
|
|
Bone fracture type Compression |
Oblique Fracture |
|
|
Bone fracture type Bending |
Butterfly Fracture |
|
|
Bone fracture type Torsion |
Spiral Fracture |
|
|
Bone Healing Stages |
-Impact -Inflammation -Soft Callus - Cartilage and vessels laid down -Hard Callus - Bone weave -Remodeling - lamellar bone |
|
|
Skeletal Muscle response to immobilization |
-Shortened position = decrease in sarcomeres -Lengthened position = increase in sarcomeres -Lower levels of ATP and Glycogen leading to more rapid depletion -Disorganization and Dissolution of myofibrils -More atrophy in Type I fibers (Slow Oxidative) |
|
|
What are the 3 zones of Type II Collagen fibers in Articular Cartilage and what forces do they resist? |
1. Tangential/Superficial = Fibers are oriented parallel to the surface which resists Shear Forces 2. Transitional/Intermediate = Fibers are arranged randomly which resists forces in a variety of directions 3. Radial/Deep = Fibers are oriented perpendicular to surface which resists tensile or compressive forces |
|
|
Articular cartilage response to immobilization |
It Thins and Softens due to the lack of compressive forces which provide the synovial circulation of nutrients |
|
|
Articular Cartilage response to Aging |
Diminished thickness due to the loss of proteoglycans Increase in stiffness, decrease in elasticity |
|
|
Tendon response to immobilization |
-A Decrease in the number of cross links leads to a weakened structure -Protein degradation > synthesis = Decreased Collagen |
|
|
Ligament response to immobilization |
-Bone resorption at Ligament-bone interface -Inability to absorb as much energy -Fails at smaller loads **More Elastic, but weaker |
|
|
Tendon response to Aging |
"Crimp" is less extensible = Stiffer Decrease in elasticity, blood supply, and weaker tendon-bone interface |
|
|
Ligament response to Aging |
More viscous (More collagen, Less Water) Less structurally strong (Decreased Ca content) Cells Less active (slower metabolism) |
|
|
Phases of Healing |
1. Inflammatory: Vasoconstriction, followed by rapid vasodilation to deliver leukocytes and phagocytes -Focus on PRICE 2. Proliferation/Repair: Fibroplasia (Scar formation) and Granulation Tissue (fibroblasts, collagen, and capillaries) -Focus on promoting Tissue Growth 3. Remodeling: Realignment and strengthening of new tissues -Progress to Functional ADLs, Prevent reoccurrence, create Discharge plan |
|
|
Differential Diagnosis Red Flags? |
-Weight change -Fatigue -Paresthesias -Bowel and Bladder -Symptoms do not change with position -Dizziness and SOB -Night Pain -Symptoms change with Visceral Organ function -Poorly localized / Diffuse |
|
|
Differential Diagnosis Yellow Flags? |
- Atypical signs or symptoms - Pain Patterns / Referred Pain - Systemic disease signs or symptoms -Signs improve but No improvement in Symptoms |
|
|
What is a simple test for Appendicitis? |
Right single leg hop test If hopping on right leg increases pain, it is more likely the patient has appendicitis |
|
|
Referred Pain Heart and Lungs refer to... |
Sternum Shoulders Base of Neck Arms |
|
|
Referred Pain Kidneys refer to... |
Upper Lumbar Region Anterior Abdomen lateral to the umbilicus |
|
|
Referred Pain Bladder refers to... |
Lower abdomen Lower Lumbar/ Upper Sacral |
|
|
Referred Pain Pancreas refers to... |
Upper Lumbar / Lower Thoracic Upper Abdomen |
|
|
Referred Pain Stomach refers to... |
Upper abdomen Mid / Lower Thoracic |
|
|
Referred Pain Abdominal Aortic Aneurysm refers to... |
Low Back Lower Abdominal Hip, Groin, or Butt |
|
|
Osteokinematics |
Motion of long bones Within the cardinal planes of the body -Sagittal -Transverse -Frontal |
|
|
Arthrokinematics |
Motion between Articular Surfaces -Roll -Slide/Glide -Spin |
|
|
Arthrokinematic Roll is caused by.... |
Muscular Contraction Generally follows the direction of the Long bone |
|
|
Occipito-Atlantal Arthrokinematics Open Chain |
Convex Occiput moving on Concave Atlas Roll and Glide go in Opposite directions |
|
|
Occipito-Atlantal Arthrokinematics Closed Chain |
Concave Atlas moving on Convex Occiput Roll and Glide go in the Same direction |
|
|
During Sit to Stand, what are the arthrokinematics of the hip? |
Spin |
|
|
Passive Physiologic Intervertebral Motion (PPIVM) |
Assess Quantity, Quality, End-Feel, and Pain-Resistance Sequence Quantity = Normal, hypo, or hypermobile |
|
|
PPIVM / PAIVM Contraindications |
Absolute: -Spinal Fracture -Cauda Equina Lesions -Neoplasm Relative: -Osteoporosis -Rheumatoid Arthritis -Neurological signs -Children |
|
|
Which should you be more cautious with? PPIVM or PAIVM? |
PAIVM |
|
|
Passive Accessory Intervertebral Motion (PAIVM) |
Localize painful segment = Test one joint at a time P to A force on Spinous process or Transverse Processes test Glide of segment Rotation can be tested through unilateral transverse process P to A or Transverse force applied to Spinous Process |
|
|
During PAIVM testing, you perform a unilateral P to A Force on the Right Transverse Process of L4. What are you assessing? |
Left Rotation of L4 |
|
|
Why do you only perform 2-3 thrusts during PAIVM assessment? |
More than that can be a treatment. You do not want to treat during the examination because that may cloud the diagnosis. |
|
|
What are good PAIVM Body Mechanics? |
Arms extended Arms and body in line with the force you wish to deliver |