![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
147 Cards in this Set
- Front
- Back
|
benign bone tumor which settles with aspirin at night |
osteoid osteoma |
|
|
Are osteoid osteomas typically large lesions? |
N. |
|
|
osteoid osteoma
|
|

|
osteoid osteoma |
|

|
osteoid osteoma |
|
|
FEGNOMASHIC:F =E = G =
|
fibrous dysplasia,enchondroma / eosinophilic granuloma,giant cell tumour
|
|
|
FEGNOMASHIC: NO
|
nonossifying fibroma, osteoid osteoma
|
|
|
FEGNOMASHIC: M= A= S= |
metastasis/myeloma, aneurysmal bone cyst, solitary bone cyst.
|
|
|
FEGNOMASHIC: H= , I= , C= .
|
hyperparathyroidism, infection, chondroblastoma. |
|
|
When determining differential diagnosis for bone tumors, what are the first things you ask yourself? |
1. morphology 2. age
|
|
|
what 4 arthropathies are associated with subchondral geodes?
|
RA, DJD, CPPD, AN.
|
|
|
osteoid osteoma tends to arise in which age group? {__-__} years.
|
10-20
|
|
|
where is osteoid osteoma most commonly found? {proximal/distal cortex/medulla of ____ or _____}
|
proximal cortex of femur or tibia |
|
|
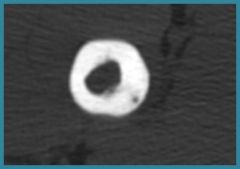
describe the typical appearance of osteoid osteoma {focal area of ___ ____ with a central _____ _____}
|
focal area of cortical thickening with a central radiolucent nidus.
|
|
|
Fibrous displasia looks like
|
can look like almost anything.
|
|
|
What syndrome is fibrous dysplasia associated with? (other than Mazabraud syndrome)
|
McCune-Albright Syndrome
|
|
|
What is the classic triad defining McCune Albright syndrome
|
polyostotic fibrous dysplasia, endocrine dysfunction, cutaneous hyperpingmentation.
|
|
|
the other name for cutaneous hyperpigmentation
|
cafe au lait spots
|
|
|
What is the typical symptom of endocrine dysfunction in Maccune Allbright syndrome?
|
precocious puberty.
|
|
|
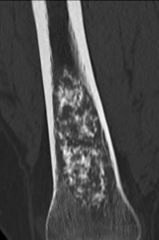
The most common cystic lesion of the phalanges
|
enchondroma
|
|
|
this is a
|
osteochondroma
|
|
|
It is difficult to differentiate between an enchondroma and a {___ ____}
|
Bone infarct
|
|

|
enchondroma
|
|
|
well defined, densely sclerotic serpinginous boarder without scalloping is a characteristic of a {_}, not a {_}
|
bone infarct, enchondroma
|
|
|
What differentiates an enchondroma from a chondrosarcoma? |
pain
|
|
|
Is histology useful for differentiating chondrosarcoma from enchondroma? What could be reassuring? {_}. {_}.
|
no. MRI.
|
|
|
Multiple enchondromas is called {_________'s} disease.
|
Ollier's
|
|
|
What four bony lesions occasionally have bone sequestra?
|
Osteomylitis, lymphoma, fibrosarcoma, eosinophilic granuloma.
|
|
|
What is the typical age of a patient with eosinophlic granuloma? { __.}
|
< 30.
|
|
|
To where do giant cell tumors rarely metastasize? {_.}
|
lung.
|
|
|
Where do giant cell tumours occur?
|
epyphysis |
|
|
Are giant cell tumors usually large or small?
|
large. |
|
|
for GCT: the zone of transition is {_}, T/F - the boarder is sclerotic {_}
|
narrow. F.
|
|
|
What is the most common benign bone lesion encountered by radiologists?
|
Nonossifying fibroma |
|
|
What is the typical age of a patient with a nonossifying fibroma? {_} and what is the penetrance? {__%}
|
young. 20%. |
|
|
Do nonossifying fibromas typically involve the cortex?
|
Y
|
|
|
Describe the boarder of a nonossifynig fibroma
|
sclerotic, thin.
|
|
|
Is periostitis associated with a non-ossifying fibroma and is the lesion painful? {_, _.}
|
N, N.
|
|
|
Is osteoblastoma a common lesion?
|
N.
|
|
|
Diffuse calvarial hyperostosis can be caused by which drug?
|
phenytoin
|
|
|
What are the 4 subtypes of fibrous dysplasia
|
monostotic polyostotic craniofacial fibrous dysplasia cherubism (mandible and maxilla affected only)
|
|
|
Malignant differential of fibrous dysplasia in the tibia or mandible
|
adamantinoma
|
|
|
What is a langerhans cell?
|
antigen presenting cell (dendritic cell) found in the skin and mucosa.
|
|
|
what differentiates a Langerhans cell from a histiocyte?
|
Birbeck granules. (looks like a tennis raquet).
|
|
|
unifocal langerhans cell histiocytosis is also known as?
|
eosinophilic granuloma
|
|
|
What is the Hand-Schuller-Christian triad?
|
diabetes insipidus, exopthalmos, lytic bone lesions
|
|
|
What is Letterer-Siwe disease? {multi/uni focus, system, _ _}
|
multifocal, multisystem Langerhans histiocytosis.
|
|
|
What is pulmonary langerhans cell histiocytosis?
|
A not-completely seperate disorder almost always (95%) seen in adult smokers (20-40 years old) and sometimes resulting in progressive pulmonary fibrosis.
|
|
|
How do you differentiate benign or malignant GCT?
|
recurrence.
|
|
|
How many appearances does eosinophilic granuloma have and is it associated with pain?
|
many, sometimes
|
|
|
what is one useful descriminator and two less useful descriminator for EG? {__, __stotic. _ _}
|
age, monostotic. Bony sequestrum.
|
|
|
What is the other common presentation of enchomdroma ?
|
Irregular speckled calcification in the distal femur.
|
|
|
What is the age prediliction of enchondroma? {_ age, but usually _}
|
Any age, but usually adults.
|
|
|
What is "benign fibrous cortical defect synonomous with?.
|
non-ossifying fibroma
|
|
|
DDx for a lesion with no periostitis or pain
|
fibrous dysplasia enchondroma NOF SBCEG (sometimes has pain)
|
|
|
DDx for an epiphyseal lesion
|
geodeinfectionchondroblastoma GCT
|
|
|
DDx for multiple bone lesions
|
fibrous dysplasia EG enchondroma mets / myeloma HPT infection
|
|
|
In what location are solitary bone cysts found?
|
Invariably central, never epiphysial, often proximal humerus or proximal femur.
|
|
|
What is the age prediliction for SBC?
|
< 30.
|
|
|
What featre of HPT must be seen to diagnose a brown tumour?
|
subperiostial resorbtion: phalanges, distal clavicles, medial aspect of proximal tibias. Looser's zone fractures.
|
|
|
An aneurysmal bone cyst is virtually always . . . {_ or _}
|
aneurysmal or expansile
|
|
|
What is the characteristic appearance of an ABC on MRI?
|
multiple cavities with fluid levels. (almost pathognomonic)
|
|
|
What is the age prediliection for an ABC?
|
less than 30 years old.
|
|
|
Are ABC's associated with pain?
|
yes.
|
|
|
What is a typical location of an ABC and where can they occur?
|
Typically posterior elements of the spine, but can occur anywhere.
|
|
|
What are ABC discriminators?
|
must be expansile patients must be younger than 30 years of age.
|
|
|
does a non-ossifying fibroma involve the cortex?
|
yes, it will replace it with fibrous tissue.
|
|
|
where do non-ossifying fibroma's occur?
|
usually around the knee but can occur in any long bone.
|
|
|
What is the DDx of a lytic bone lesion in the epiphysis of a young patient (< 30 years)
|
infection (most common) chondroblastoma GCT rare - ABC and EG
|
|
|
what diseases are associated with subchondral cysts (geodes)
|
degenerative joint disease (must be associated with joint space narrowing, subchondral sclerosis and osteophyte formation) rheumatoid arthritis calcium pyrophosphate dihydrate deposition disease (CPPDDD) avascular necrosis
|
|
|
Chondrobastoma discriminators
|
patient must be younger than 30 years must be epiphyseal.
|
|
|
What can never be excluded in a patient younger than 30 years?
|
Eosinophilic granuloma infection
|
|
|
What can never be excluded in a patient over 40 years old?
|
metastatic disease infection
|
|
|
What are 4 useful radiologic criteria for determining whether a lesion is malignant or benign?
|
cortical destruction - not really periostitis - difficult to differentiate "aggressive" from "benign" orientation of the lesion - not helpful at all zone of transition - yes!
|
|

|
osteoid osteoma
|
|

|
osteoid osteoma |
|
|
Salient features of osteoid osteoma |
* nidus (meshwork of dilated vessels and osteoclasts) * fibrovascular rim * surrounding reactive sclerosis |
|
|
Can a non-ossifying fibroma involve the cortex
|
yes, the cortex may be replaced by benign fibrous tissue. |
|

|
fibrous dysplasia |
|

|
fibrous dysplasia - polystotic form |
|

|
Fibrous dysplasia - monostotic |
|

|
Giant Cell Tumour |
|

|
Giant cell tumour |
|

|
non-ossifying fibroma
|
|

|
Giant cell tumour of bone |
|

|
Aneurysmal bone cyst |
|

|
healing non-ossifying fibroma |
|
|
Other name for a solitary bone cyst
|
unicameral bone cyst
|
|

|
simple bone cyst (unicameral)
|
|
|
T2 weighted. Lesion returns low signal on T1. |
unicameral (simple) bone cyst
|
|

|
unicameral (simple) bone cyst
|
|
|
T2 image. T1 signal was low also
|
non-ossifying fibroma |
|
|
What are the MRI appearances of non-ossifying fibroma? |
T1 low signalT2 variable. intermediate to high initially, then low as the lesion ossifys.
|
|

|
osteochondroma
|
|

|
Frontal view of the left shoulder shows expansion of the proximal left humeral diametaphysis with a ground glass matrix and adjacent cortical thinning. There is a left proximal humeral bony excrescence as well as a protrusion of the cortex medially. In addition, there is a bony protuberance projecting from the medial mid left scapula. These findings are suggestive of Hereditary multiple exostoses (HME), which is characterized by the presence of multiple osteochondromas. |
|
|
define excrescence |
abnormal outgrowth |
|
identify this lesion |
enchondroma
|
|

p |
enchondroma |
|

p |
enchondroma |
|
|
T1, lesion high signal on T2. Note surrouding |
enchondroma
|
|

|
renal cell carcinoma
|
|

|
chondroblastoma
|
|
|
What is the tissue of origin for chondroblastoma |
-Usually benign, cartilaginous tumor |
|
|
What is the key radiologic feature? |
-Epiphyseal lytic lesion in children and teens
|
|
|
is a chondrobastoma usually painful? |
Yes. |
|
|
osteoid osteoma epidemiology (__ to __ years, M:F) |
10 to 25 years, 3:1
|
|
|
enchondroma is a |
benign tumour of hyaline cartilage
|
|
|
what gives an enchondroma its characteristic "speckled appearance" |
chondroid matrix |
|
|
What disease and what syndrome are multiple enchondromas (and hemangiomas) associated with?
|
Ollier disease, Maffuci syndrome
|
|
|
"automatics" where patient is younger than 30 years old? |
eosinophilic granuloma infection |
|
|
"automatics" if patient is more than 30 years old |
metastasis infection |
|
|
Discriminator for fibrous dysplasia
|
No periosteal reaction |
|
|
If fibrous dysplasia is suspected in the tibia ___ should also be considered
|
adamantinoma
|
|
|
Enchondroma descriminators
|
Calcification, no pain
|
|
|
Eosinophilic granuloma discriminators
|
younger than 30.
|
|
|
Giant cell tumour descriminators
|
epiphyses closed, abuts articular surface, well defined with non-sclerotic margin.
|
|
|
Non ossifying fibroma descriminators
|
younger than 30, no periostitis.
|
|
|
Aneurysmal bone cyst descriminators
|
expansile, younger than 30.
|
|
|
Solitary bone cyst
|
central, younger than 30. |
|
|
Chondroblastoma descriminators
|
epiphyseal, younger than 30.
|
|
|
4 criteria useful for determining malignant nersus benign lesions:
|
cortical destruction, periostitis, axis, zone of transition.
|
|
|
most important descriminator of bone malignancy
|
zone of transition
|
|
|
mallignant tumours will appear to have a ___ zone of transition on MRI
|
narrow
|
|
|
benign periostitis appears as
|
cortical thickening |
|
|
malignant periostitis characterised by {sun___, amo___, co___ ____, o___ s___}
|
sunburst, amorphous, codman triangle, onion skin. |
|
|
The only two childhood malignant tumour of bone
|
osteosarcoma, Ewings sarcoma |
|
|
Common malignant tumours of bone in adulthood
|
metastasis, myeloma, chondrosarcoma.
|
|
|
most common malignant bone tumour
|
osteosarcoma |
|
|
In what circumstances might osteosarcoma be found in an older person?
|
padget's disease, radiation induced
|
|
|
T/F: parosteal osteosarcoma is more aggressive.
|
F
|
|
|
cortical desmoid occures at the insertion / origin of { __ __ of __ or __ __}
|
medial head of gastrocnemius or adductor magnus
|
|
|
benign avulsion injury of distal femur |
cortical desmoid
|
|

p |
myositis ossificans |
|
|
3 "knee jerk" diagnoses for a permeative lesion in a child:
|
Ewing sarcoma, infection, eosinophilic granuloma.
|
|
|
Is Ewings sarcoma usually symptomatic
|
Y |
|
|
Low grade chondrosarcoma appears very similar histiologically to:
|
enchondroma |
|
|
Differentials for lytic lesion with aggressive features in an older patient
|
metastasis, plasmacytoma, fibrosarcoma, malignant fibrous histiocytoma, infection. |
|
|
What are the two most common soft tissue tumours?
|
MFH and liposarcoma
|
|
|
Osteochondroma
|
Cartilage-capped osseous excrescence with continuous cortex and marrow extending from underlying bone.
|
|
|
Chondroblastoma
|
Benign cartilage tumor arising in epiphysis of skeletally immature individuals
|
|
|
parosteal
|
pertaining to the outer surface of the periosteum
|
|
|
Leterer-Siwe Disease
|
Multifocal, multiorgan LCH. |
|
|
3 Types of Langerhans cell histiocytosis
|
1) Leterer-Siwe Disease 2) Uni/multifocal Unisystem. 3) Pulmonary LCH |
|
|
melorheostosis
|
flowing segmental ossification (dripping candle wax sign) |
|

|
periosteal chondroma (juxtacortical chondroma) |
|

What angle is this? |
Bohler angle |
|
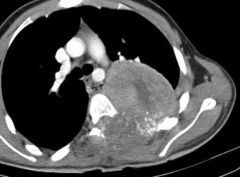
9 year old boy |
Askin tumour |