Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
207 Cards in this Set
- Front
- Back
|
Semantic content of language; related part of brain
|
semantic content refers to language's ability to convey meaning; left temporal area. Prefrontal cortex also hypothesized to play role in semantic processing. Left temporal injury associated with Wernicke's aphasia
MSE 53 |
|
|
Motoric aspects of language; related part of brain
|
include proper articulation and assembly (according to rules of grammar), of the building blocks of words (phonemes and morphemes), facial and gestural (e.g. sign language) expressions and writing. Left frontal lobe important in this. Injury here associated with Broca's aphasia
MSE 53 |
|
|
Pragmatics; related brain region
|
aspect of langage concerned with its overall communicative value. While dominant (usually left) hemisphere controls most aspects of langage, right side contributes to its communicative value; plays important role in allowing person to use metaphor, to abstract; example of R hemisphere's integrative functions
MSE 53 |
|
|
Disorders of language fluence - Nonfluent - (6)
|
Broca's aphasia
Transcortical motor aphasia Global aphasia Stuttering Cluttering Scanning Speech MSE 56 |
|
|
Which aphasia is:
Fluent Intact Comprehension Intact repetition |
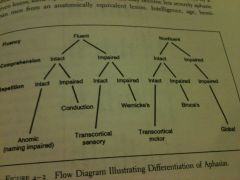
Anomic (naming impaired)
MSE 56 |
|
|
Which aphasia is:
Nonfluent Intact comprehension Impaired repetition |
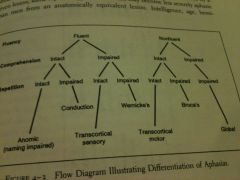
Broca's
MSE 56 |
|
|
Which aphasia is:
Fluent Impaired Comprehension Intact repetition |
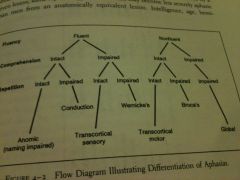
Transcortical sensory
MSE 56 |
|
|
Which aphasia is:
Nonfluent Impaired comprehension Impaired repetition |
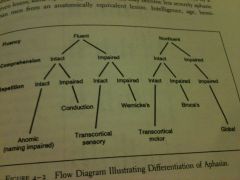
Global
MSE 56 |
|
|
Which aphasia is:
Fluent Intact comprehension Impaired repetition |
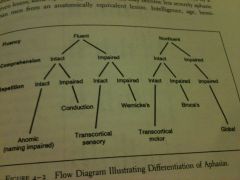
Conduction
MSE 56 |
|
|
Which aphasia is:
Fluent Impaired comprehension Impaired repetition |
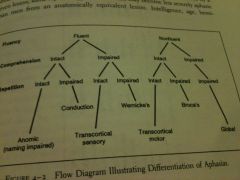
Wernicke's
MSE 56 |
|
|
Which aphasia is:
Nonfluent Intact comprehension Intact repetition |
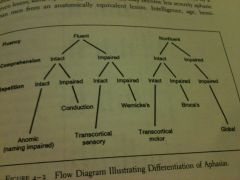
Transcortical motor
MSE 56 |
|
|
Disorders of Language Fluency - Fluent - (3)
|
Wernicke's aphasia
Conduction aphasia Transcortical sensory aphasia MSE 56 |
|
|
Broca
SPEECH COMPREHENSION REPETITION NAMING GRAMMAR PROSODY PARAPHASIAS SEMANTICS |
Broca
SPEECH nonfluent COMPREHENSION normal REPETITION impaired NAMING +/- GRAMMAR impaired PROSODY impaired PARAPHASIAS some SEMANTICS meaningful MSE 58 |
|
|
Wernicke
SPEECH COMPREHENSION REPETITION NAMING GRAMMAR PROSODY PARAPHASIAS SEMANTICS |
Wernicke
SPEECH fluent COMPREHENSION impaired REPETITION impaired NAMING impaired GRAMMAR +/- PROSODY normal PARAPHASIAS yes SEMANTICS empty MSE 58 |
|
|
Conduction aphasia
SPEECH COMPREHENSION REPETITION NAMING GRAMMAR PROSODY PARAPHASIAS SEMANTICS |
Conduction
SPEECH fluent COMPREHENSION normal REPETITION impaired NAMING impaired GRAMMAR +/- PROSODY normal PARAPHASIAS yes SEMANTICS meaningful MSE 58 |
|
|
Global aphasia
SPEECH COMPREHENSION REPETITION NAMING GRAMMAR PROSODY PARAPHASIAS SEMANTICS |
Global
SPEECH nonfluent COMPREHENSION impaired REPETITION impaired NAMING impaired GRAMMAR impaired PROSODY impaired PARAPHASIAS yes SEMANTICS empty MSE 58 |
|
|
Anomic aphasia
SPEECH COMPREHENSION REPETITION NAMING GRAMMAR PROSODY PARAPHASIAS SEMANTICS |
Anomic
SPEECH fluent COMPREHENSION normal REPETITION normal NAMING impaired GRAMMAR +/- PROSODY normal PARAPHASIAS yes SEMANTICS +/- MSE 58 |
|
|
Transcortical Motor aphasia
SPEECH COMPREHENSION REPETITION NAMING GRAMMAR PROSODY PARAPHASIAS SEMANTICS |
Transcortical Motor
SPEECH nonfluent COMPREHENSION normal REPETITION normal NAMING impaired GRAMMAR impaired PROSODY impaired PARAPHASIAS some SEMANTICS meaningful MSE 58 |
|
|
Transcortical Sensory aphasia
SPEECH COMPREHENSION REPETITION NAMING GRAMMAR PROSODY PARAPHASIAS SEMANTICS |
Transcortical Sensory
SPEECH fluent COMPREHENSION impaired REPETITION normal NAMING impaired GRAMMAR +/- PROSODY normal PARAPHASIAS yes SEMANTICS empty MSE 58 |
|
|
Aphasia vs. language difficulty in psychiatric d/o - in general
|
Language alterations resulting from psych causes tend to be less severe than aphasias; are associated with other Sx of the particular Dx.
MSE 60 |
|
|
Language alterations in schizophrenia/mania language deficits
|
schizophrenics or manics are most likely to have only temporary abnormalities of speech, which occur during acute episodes of illness. When more persistent, they tend to be associated with Sx like delusions, hallucinations, and mood disturbance
MSE 60-1 |
|
|
Degenerative dementia-associated language deficits
|
In degenerative dementias, like Alzheimer's, the language defects tend to be insidious, progressing over a relatively long period of time
MSE 60 |
|
|
Frontal lobe dementia-associated language deficits
|
Frontal lobe dementias, such as Pick's dz, can lead to a nonfluent aphasia.
MSE 61 |
|
|
Parietotemporal dementias - language deficits
|
In parietotemporal dementias (Alzheimer's), syntax and motor speech fluency are usually spared, but semantics and comprehension are not. Naming and word-finding difficulties are some of the earliest findings in AD, as semantic information is lost; semantic paraphasias are common.
MSE 61 |
|
|
What aphasia does each stage of dementia resemble?
Mild? Moderate? Severe? End-stage? |
Mild - anomic
Moderate - transcortical sensory Severe - Wernicke's End-stage - global MSE 61 |
|
|
Demented patients have which language dysfunctions (2)?
|
perseveration, palilalia
MSE 61 |
|
|
Late stage AD vs. Wernicke's - differentiation
|
In AD, there is likely to have been a preceding period of gradual deterioration. Also, language impairment in dementia is but one of a constellation of symptoms (wandering, memory loss, etc.), whereas it is the most prominent disturbance in aphasia
MSE 61 |
|
|
Delirium - language deficits
|
language deficits in delirium may be primary or related to cognitive defecits. Responses often irrelevant and include paraphasic or articulation errors. Syntax/comprehension also impaired. Writing frequently impaired, confrontational naming may be deficient. Usually cannot pay attention to tasks and have concentration deficits that affect broad range of cognitive tasks (vs. aphasics - goo attention to tasks).
MSE 61 |
|
|
Schizophrenia language deficits vs. aphasias - similarities
|
Loose associations of schizophrenia may resemble fluent aphasia. Word salad (rare) resembles severe fluent aphasia (distorted grammar, incoherent speech, neologisms, semantic paraphasias). Pts. usually seem unaware of incoherence/peculiarity of speech. May switch between in-/coherent in same conversation. Pts. have loose associations, bizarre content, focus on semantic/phonemic aspects of language.
MSE 61-2 |
|
|
Schizo vs. aphasia - learning deficits - contrasts
|
Aphasia>schizo: word-finding difficulties, impaired confrontational
Schizo (vs. fluent aphasics) usually have intact repetition, naming, syntax, writing ability, comprehension (except in most severely psychotic cases). Schizophrenics are usually able to write to dictation, name objects, and, except in word salad, use syntax correctly (though this may deteriorate as schizophrenia progresses) MSE 62 |
|
|
Causes of anomia
|
s/p closed head injury, AD, sleep deprivation, anxiety, delirium, encephalitis, brain trumors, aphasias
MSE 62 |
|
|
Circumlocution
|
talking around the intended word
MSE 62 |
|
|
When naming of objects is deficient, check for...
|
When naming of objects is deficient, check for pt's ability to recognize the identity of the objects or their use/function
MSE 62 |
|
|
Nominal (anomic) aphasia
|
type of fluent aphasia
patient cannot name things, either spontaneously in speaking or when confronted can repeat, has only mild impairment in comprehension pt is usually aware of difficulty (vs. Wernicke's), which he may try to conceal (although later in dementia, there may be no insight into deficits) MSE 62 |
|
|
Nominal (anomic) aphasia - associated brain region damaged?
|
damage located to left anterior temporal cortex can produce an isolated naming deficit without associatd language impairment - depending on precise area affected, differentially affects retrieval of proper nouns vs. common nouns
MSE 62 |
|
|
Prosody of speech
|
refers to variations in rate, rhythm, stress in speech. Includes musicality, intonation, phrasing, and intervals. It adds an emotional dimension to conversation and can alter meaning.
MSE 62 |
|
|
Prosody of speech - localization
|
R cerebral hemisphere - major role in production of emotional prosody
L hemisphere - variations in pitch and rhythm MSE 62 |
|
|
Impairment of prosody leads to...
|
Effects in both expression of speech as well as comprehension of meaning of others' speech. Aprosodic patients have difficulty expressing/interpreting affective communications.
MSE 62-3 |
|
|
Aprosody - associated lesions
|
Anterior R hemisphere - more expressive deficits in prosody
Posterior R hemisphere - more receptive deficits Analogous to aphasia pattern with L hemisphere lesions) MSE 63 |
|
|
Aprosody - clinical associations
|
Prosody affected in aphasia, e.g. Broca's (rate and rhythm). In Wernicke's, prosody generally preserved. Dementia, R hemisphere lesions, Parkinsonism. Regional differences in dialect must be considered (e.g. Southern dialect more musical, may sound dramatic or expressive)
MSE 63 |
|
|
Rate of speech; clinical associations
|
varies from slow to rapid. Anxious - rapid; depressed - slow. Alcohol - may speak quickly and forcefully
MSE 63 |
|
|
Pressured speech
|
large amount of speech at quicker pace; trying to squeeze many words in a given time period; difficult to interrupt; often accompanied by greater loudness and intensity.
MSE 63 |
|
|
Pressured speech - often accompanied by what in manic patients
|
tend to be loquacious and have racing thoughts. Often accompanied by flight of ideas
MSE 63 |
|
|
Pressured speech - clinical associations
|
in mania and severe anxiety, this urge to speak occurs without a filter; nearly all thoughts are verbalized
MSE 63 |
|
|
Latency of speech
|
length of pauses between phrases or before beginning sentences. If these are long, speech latency is said to be prolonged
MSE 63 |
|
|
Speech latency - depression
|
depressed patients often speak slowly, sometimes softly, with longer than normal pauses between words, phrases and sentences
MSE 63 |
|
|
Speech latency - parkinsonism
|
Parkinsonian patients are slowed in a number of motor functions, including speaking rate
MSE 63 |
|
|
Speech latency - nonfluent language disorders
|
hesitance, difficulty initiating speech increase latency
MSE 63 |
|
|
Slow speech - differential
|
MR, severe dementia, intoxication with drugs that suppress the CNS (e.g. barbiturates)
MSE 63 |
|
|
Autism - speech
|
autistics can have difficulty initiating speech and may exhibit aprosodia
MSE 63 |
|
|
Rhythm - disorders
|
In cluttering, rhythmicity is disturbed; autistics have idiosyncratic stress and rhythm; stutterers interrupt normal rhythm when they get stuck
MSE 63 |
|
|
monotony - clinical associations, brain lesions
|
depression (lack animation, have sparse interest or energy for socializing or pursuing pleasurable activities). Alexithymic pts speak aprosodically, as do pts with parkinsonism and right frontal lobe lesions
MSE 64 |
|
|
Quality of speech - elements (7)
|
amount, loudness, phonation, pitch, amount, articulation, spontaneity
MSE 64 |
|
|
Loud speech - clinical associations
|
manic pts behaving w/o social sensitivity - yell, raise voices inappropriately. Demented - may scream uncontrollably. Delirious - may yell b/c confused, may mumble unintelligibly. Pain - appropriate yelling. Psychotic pts in seclusion. Angry/irritated. Deaf/hard of hearing.
MSE 64 |
|
|
Soft speech - clinical associations
|
Depressed pts may be soft-spoken; suspicious persons may whisper. Conversion d/o - whisper. Persistent hoarseness - vocal cord injury/dysfunction, recent intubation, influenza, hypothyroidism. Straining/tremor - motor dysfunction, including extrapyramidal d/o such as parkinsonism
MSE 64 |
|
|
Amount of speech
|
ranges from sparse to talkative. Also, mutism.
MSE 65 |
|
|
Loquacious speech - DDx
|
manic, anxious, attempting to control interview, Wernicke's
MSE 65 |
|
|
Sparse speech - clinical associations
|
Depression - may be socially avoidant
MSE 65 |
|
|
Mutism
|
Absence of speech. Can be caused by neurologic d/o such as complex partial seizure, mesial frontal infarction; or due to psychiatric d/o such as schizophrenia, other psychoses, delirium, autism, severe depression, catatonia, end-stage dementia, conversion d/o, factitious d/o
MSE 65 |
|
|
Spontaneity of speech - clinical associations
|
degree to which patient initiates and engages in conversation. Depressed - decreased, paucity, slow rate, imparied prosody, reduced loudness. Manics - usually eager to speak, do so loquaciously. Paranoid/suspicious - may be hesitant to initiate. Demented/delirius - may have reduced spontaneity of speech
MSE 65 |
|
|
Dysarthria - types (5)
|
poorly articulated speech. spastic, flaccid, ataxic, hypokinetic, hyperkinetic
MSE 65 |
|
|
Dysarthria - causes
|
Broca's pts - articulation probs, esp if associated paresis of facial/oropharyngeal mm. Slurring may = EtOH intox or motor dysfunction of oral-pharyngeal area inc tongue. Chorea/TD can alter articulation through abrupt interruptions of coordinated mm. activity. Drug side effects may impair articulation, e.g. dry mouth 2/2 anti-Ch drugs or sedation related to analgesics/hypnotics.
MSE 65 |
|
|
Phonation/resonation - abnormalities
|
abnormalities in resonance (quality of speech contributed by oral cavity in relation to palate) can reduce intelligibility, e.g. hypernasality 2/2 paralysis of soft palate or cleft palate
MSE 66 |
|
|
Dominant hemisphere - tests for handedness
|
hand - writing (though many left-handers forced to write with R in childhood), simulation of tasks, e.g. striking match, threading needle, dealing cards, brushing hair. foot - simulate kicking ball. eye - instruct pt to peer through 1/2 in hole in paper held at arm's length at instructor's finger. Then tell pt. to open one eye at a time - finger disappears when dominant eye closed. Writing has highest congruence, eye lowest.
MSE 66-7 |
|
|
difficulties/abilities in dysphasic/aphasic pts
|
trouble with propositional speech, but usually capable of nonpropositional (gesture/affective) communications and overlearned verbalizations, inc nonverbal utterances (esp. those that convey affect), simple well-learned words like hello, no, and profanity, a familiar song, and overlearned materials like the days of the week.
MSE 68 |
|
|
Examination clues to fluency
|
First listen to spontaneity - ask open ended questions. Is speech telegraphic or monosyllabic (suggesting nonfluency)? Are conjunctions/ connectives omitted (suggesting the same)? Rules of grammar followed? Substantive content to communication? Prolonged latency b/w words (>3s). Amount of words (<50/min - severe depression, nonfluency, catatonia, mutism; normal - 100-150. >200 - fluent aphasia, mania). Reduced phrase length suggests nonfluency. Expletives - nonfluent aphasia or Tourette's or antisocial. Poor articulation - nonfluent, frustration, effortfulness in speaking, dementia, delirium, catatonia, significant MR, autism, severe psychosis
MSE 68 |
|
|
Repetition - examination - 5 steps
|
1) simple, familiar words - dog, school
2) multisyllabic - hospital 3) short phrases - running into the garage 4) simple sentences - The spy fled to Greece. The postal service delivered the package to my neighbor 5) Sentences w/ complex syntax - If the blue boat arrives very soon, we can go fishing for sharks. MSE 69 |
|
|
Repetition - inappropriate (perseveration)
|
these patients will continue to repeat the task even after it is no longer requested
MSE 69 |
|
|
Repetition difficulties - clinical correlation in aphasias
|
conduction, Wernicke's and Broca's aphasias impair even simple repetition
MSE 69 |
|
|
Repetition - inappropriate (echolalia) - clinical correlations
|
pts. w/ schizophrenia, frontal dementias, transcortical aphasias, and autism may have echolalia during interviews when they are not asked to repeat things
MSE 69 |
|
|
Repetition - inappropriate due to sarcasm/lack of cooperation - clinical correlation
|
May be seen in manics who may keep repeating just to annoy the examiner
MSE 69 |
|
|
Repetition - difficulty repeating long/complex phrases b/c of attentional deficits and confusion - clinical correlation
|
delirium
MSE 69 |
|
|
Repetition - verbigeration vs. perseveration - clinical correlation
|
in verbigeration, words, phrases and even entire sentences, which were not previously part of a normal conversation (as in perseveration) are repeated. e.g. in schizophrenia and catatonia
MSE 69 |
|
|
Repetition - Palilalia - clinical correlation
|
repetition of one's own words at an increasingly rapid pace with progressively poorer articulation. Rare, occurs in delirium, schizophrenia, Tourette's, aphasias, basal ganglia d/o (e.g. Parkinsonism), pseudobulbar palsy, encephalitis, transcortical aphasias
MSE 69, 79 |
|
|
Comprehension testing - first things to establish
|
Establish adequate hearing, esp. in elderly. Because tests have motor component, impaired patients should be checked for apraxia or paresis
MSE 69 |
|
|
Comprehension testing - after establishing hearing/motor ability, test how?
|
Increasingly complex sets of commands.
Single step - Point to your eyes. Are you wearing a ring? Is it raining today? Two-stage - Touch your left hand to your right ear. Put the pencil under the paper Three-stage of unrelated activities - Pick up the paper clip, put it on the table, and cross your arms MSE 69 |
|
|
Comprehension - clinical correlation of relative deficiency
|
Comprehension may be deficient for some, but not other, verbally related tasks. It is usually not completely deficient even in aphasia, though it may be in extreme cases, e.g. delirium, severe dementia, word deafness
MSE 69-70 |
|
|
Comprehension deficiency - basic vs. abstract/advanced
|
comprehension may be intact for basic things or for concrete thinking, but not for more abstract thinking about complicated relationships and judgments. Presence of significant psychiatric d/o, inc. dementia, severe depression, psychosis, severe anxiety, delirium, can prevent full comprehension of subtle, abstract, or conceptual, words or phrases (e.g. peace, justice, truth, love)
MSE 70 |
|
|
Comprehension testing - advanced/abstract
|
test ability to comprehend statements that involve comparisons and relational concepts. "If you buy an orange for 40 cents and give clerk a dollar, how much change?" "If Joe is taller than Richard and shorter than Harold, who is the tallest?" Can ask pts to read a paragraph from newpaper or magazine and quiz on content
MSE 70 |
|
|
Naming - types of testing
|
Confrontational (single objects, objects within a picture, parts of an object), Boston Naming Test (line drawings), list generation
MSE 70-1 |
|
|
Confrontational naming - methods
|
ask for names of objects, then smaller parts of those objects. If using line drawings, they usually range from easy drawings to less common objects
MSE 70 |
|
|
Naming - what to do when a patient can't name an object - three steps
|
First, give semantic clue (e.g. for camera, "It is used to take photographs"). Then, give phonemic clue "It begins with a ka sound." Then give a short list of words to choose from. Note down how much cuing was needed, as it correlates to impairment level.
MSE 70 |
|
|
Cookie Theft Picture
|
Example of confrontational test drawing. Ask pts to name people, objects and actions. Can use this as a stimulus for spontaneous speech.
MSE 70-1 |
|
|
List generation - methods
|
Ask pt to generate as many words as possible in 60 seconds from same category (e.g. wild animals, types of fruit, things in a grocery store) or starting with same letter. Normals produce >20/min.
MSE 71 |
|
|
List generation deficiency - Alzheimer's
|
May perseverate
MSE 71 |
|
|
List generation deficiencies - Aphasics + pts with L prefrontal lesions vs. pts w/ poor motivation
|
typically more impaired on letter than category fluency. Pts w/ poor motivation perform similarly on both.
MSE 71 |
|
|
list generation deficiencies - bifrontal lesions
|
Bifrontal lesions produce severe deficiencies.
MSE 71 |
|
|
list generation deficiencies - anomics
|
Anomics may circumvent intended word and purposefully retrieve a related word that doesn't fit category/letter (this is not true semantic paraphasia)
MSE 71 |
|
|
Writing ability - clinical correlation
|
Usually writing problems mirror those in speech. Reading/writing impaired by range of d/o, inc. aphasias, dyslexia, visuospatial deficits, movement d/o (chorea, etc.)
MSE 72 |
|
|
Writing examination - first step
|
Check that vision is intact
MSE 72 |
|
|
Writing examination - if visuospatial deficits are suspected (e.g. R hemisphere lesion)
|
Have pt copy some sentences and check for perceptual distortions, such as the shapes of letters, difficulty with spatial positioning of lines in reference to margins, writing off the edge of the page, etc.
MSE 72 |
|
|
Writing examination
|
After checking visual acuity, test writing through spontaneous, dictated, and assigned narrative tasks. Signature is overlearned - insensitive screening test. For repetition, beging with familiar things, e.g. home address or months of year. Check visuospatial distortions if applicable. Next have pt write sentence of own choosing for one minute. Check these for grammar, spelling, penmanship, semantics and paraphasic errors. Sentences should contain subjects, verbs, and objects.
MSE 72 |
|
|
Writing - Broca's aphasia
|
Write large, messy letters, misspell, omit connecting words
MSE 72-3 |
|
|
Writing - paretic dominant hand or use of non-dominant hand
|
poor penmanship
MSE 73 |
|
|
Writing - Wernicke's
|
write more neatly than Broca's, but use wrong words and have misspellings
MSE 73 |
|
|
Writing - Parkinsonism
|
write with progressively smaller letters (micrographia) as disease advances.
MSE 73 |
|
|
Writing - Interictal temporal lobe epileptics
|
May write pages of detailed idiosyncratic material - hypergraphia
MSE 73 |
|
|
Writing - frontal lobe damage
|
may perseverate certain letters, e.g. mmmother, booook. In these pts, letter substitutions may be phonemic, e.g. b for p, whereas other letters may bedeleted; entire words may be incorrectly substituted, e.g., tiger for house, with words that may/may not have any meaningful relationship to correct word
MSE 73 |
|
|
Writing examination - for subtle deficits
|
Examiner can dictate several sentences, have the patient copy sentences, or ask the patient to write a narrative summary about a hobby or favorite activity
MSE 73 |
|
|
Reading examination - considerations
|
type should be large enough, first check pt's vision, difficulty of material should be adjusted to age and education
MSE 73 |
|
|
Reading examination - determining comprehension - does reading aloud indicate comprehension?
|
comprehension evaluated by asking patient to describe what he or she just read. Evaluate accuracy of words and sentences as patient reads. Ability to read aloud does not necessarily indicate comprehension, but does suggest an intact phonologic output system.
MSE 73 |
|
|
Dyslexia vs. acquired alexia
|
acquired alexia - may be associated with aphasia.
dyslexic children have difficulty reading, particularly with comprehension, but other aspects of language are intact. MSE 73 |
|
|
Types of dyslexia
|
There are many types, which correspond to particular deficits, such as difficulty w/ perceiving shapes of letters, reversing letters, etc.
MSE 73 |
|
|
Difficulties with reading aloud vs. with silent reading with comprehension - Transcortical motor aphasia and Broca's
|
Aphasias - similar deficits in reading aloud as in speaking
Broca's/transcortical motor aphasia - may not be able to read aloud, but can comprehend written material read silently. MSE 73 |
|
|
Difficulties with reading aloud vs. with silent reading with comprehension - Alzheimer's
|
Alzheimer's - reading aloud may be less impaired than reading comprehension, b/c phonology and syntax usually remain intact relatively longer than other aspects of language.
MSE 73 |
|
|
Difficulties with reading aloud vs. with silent reading with comprehension - Alexia with agraphia - corresponding lesion?
|
Reading difficulties are dissociated from writing difficulties, usually due to lesion of posterior corpus callosum and left occipital lobe. Such patients can write meaningfully (spontaneously or to dictation), but are unable to read even their own production.
MSE 73-4 |
|
|
Difficulties with reading aloud vs. with silent reading with comprehension - alexia with agriaphia - corresponding lesion?
|
Unable to read aloud or write. Lesion of left angular gyrus of inferior parietal lobe.
MSE 74 |
|
|
Prosody assessment
|
Prosody is assessed in the musicality and intonation of words and phrases and in the relationship of the intonations to the meaning of sentences.
MSE 74 |
|
|
Prosody assessment - monotonous speech
|
Monotonous speech is a clue to R hemisphere dysfunction, depression, or alexithymia
MSE 74 |
|
|
Prosody assessment - overall rate of speech and variations in rate relating to specific topics of conversation
|
These may indicate anxiety or difficult issues
MSE 74 |
|
|
Prosody assessment - increased response latency
|
occurs in depression and parkinsonism
MSE 74 |
|
|
Prosody assessment - unusual rhythms or cadences
|
Suggestive of cluttering or other nonfluencies
MSE 74 |
|
|
Prosody assessment - lesions that alter affective prosody of speech
|
Lesions of R frontal and parietal lobes. Evaluate other neurologic functions of these areas.
MSE 74 |
|
|
Quality of speech assessment - initial considerations
|
begin with observations of patient's facial appearance. Asymmetries of cheeks or mouth at rest or with smiling might suggest unilateral paralysis of a facial nerve or a stroke. The protruded tongue should be in the midline and free of choreiform movements. Note condition of teeth - edentulousness can contribute to dysarthria.
MSE 74 |
|
|
Quality of speech assessment - articulation
|
Have patient repeat phrases that do not have the expected subject-verb-object grammatical structure. E.g. "No ifs, ands or buts", "Methodist Episocopal"
MSE 74 |
|
|
Quality of speech assessment - phonation/volume
|
Respiratory rate and ease of breathing can affect these. Whispering may be due to pt tiring easily as opposed to depression. Hoarseness may be a clue to distinguish aphonia from mutism.
MSE 74 |
|
|
Agrammatism
|
Inability to string words together in phrases or sentences using rules of grammar. May occur in speech or writing
MSe 74 |
|
|
Syntax - what is it?
|
Proper sequencing/heirarchy of words in accord with grammatical rules. This and the meaning of each word determines the meaning of a sentence.
MSE 74, 80 |
|
|
Syntactical errors - associated with?
|
Broca's aphasia, end-stage dementia
MSE 74, 80 |
|
|
Telegraphic speech - what is it?
|
agrammatical speech lacking small words - e.g. pronouns and prepositions - that are important to grammar
MSe 74 |
|
|
Agraphia - definition
|
A loss of acquired ability to write language. Can happen w/ or w/o impairment in reading. May be part of aphasia constellation.
MSE 75 |
|
|
Agraphia vs. dysgraphia
|
complete vs. incomplete loss of ability to write language
MSE 75 |
|
|
Cerebral functions related to writing which may be lost/disrupted in agraphia
|
intelligence, ability to comprehend written words, praxis, motor function, visuospatial ability
MSE 75 |
|
|
Alexia - definition
|
loss or impairment of ability to read. Comprehension of reading requires not only pronuncaiation of words, but also understanding of meaning of written words (semantics)
MSE 75 |
|
|
Alexia - relationship with aphasias, agraphias. What is alexia w/o agraphia usually a result of?
|
In alexia, comprehension of written language is impaired. If accompanied by impairment in writing (agraphia), it is usually a part of an aphasia. Alexia w/o agraphia often result of a visual-verbal disconnection syndrome
MSE 75 |
|
|
Amusia - definition, clinical associations
|
defect in apreciation or expression of music. Can be associated with Broca's or Wernicke's. May be isolated phenomenon. Some aphasics can use muical tunes to help retrieve words.
MSE 75 |
|
|
Anomia - definition; symptom limited to what?
|
difficulty finding words to label persons or things, or difficulty naming objects when shown them, even though they are recognized as being familiar. Can be limited to certain categories of things, such as colors or sounds. Limited to word-finding difficulty.
MSE 75 |
|
|
Anomias - part of or due to what?
|
Can be part of aphasia or due to other d/o, such as Alzheimer's, increased ICP, delirium, conversion d/o, other nonfocal brain d/o
MSEm 75 |
|
|
Anomia - due to Broca's vs. due to Wernicke's
|
Broca's - word production type (phonemic). Wernicke's - semantic type.
MSE 75 |
|
|
Mild anomia that responds to phonemic cueing - seen in?
|
depression, parkinsonism, delirium, normal-pressure hydrocephalus
MSe 75 |
|
|
Anomia involves a disruption of pathways b/w?
|
between language areas and the particular primary sensory areas
MSe 75 |
|
|
Anomic aphasia - definition
|
inability to name objects and people despite relatively intact speech (except for some paraphasic errors), comprehension and repetition.
MSE 75 |
|
|
Anomic aphasic pts - Are they apraxic? How is their writing? Can they use the objects they can't name?
|
Anomic/nominal aphasia - type of fluent aphasia. Not apraxic. Writing is similarly impaired. Can demonstrate how to use objects.
MSE 75 |
|
|
Anomic aphasia - comprehension, confrontational naming, repetition
|
comprehension is possibly only slightly impaired, confrontational naming is defective, repetition is intact.
MSE 75 |
|
|
Anomic aphasia - caused by lesion where?
|
Often caused by lesions in dominant temporoparietal area, but may result from lesions almost anywhere in L hemisphere or from diffuse brain damage
MSE 75 |
|
|
Aphasia - definition
|
loss or deterioration of ability to comprehend and express ideas through language, including writing, reading, speaking, comprehension
MSE 75 |
|
|
aphasia vs. dysarthria
|
aphasia is a CNS d/o, not due to lesions of vocal cord apparatus, etc.
MSE 75-6 |
|
|
Insight of patients with aphasias
|
variees, e.g. Broca's pts. are aware of their difficulty and frustrated by them. Wernicke's don't know that their speech is nonsensical
MSE 76 |
|
|
Examples of successful speech from aphasics
|
Simple well-learned words may still be intact (hello, yes, no, please). Profanity may be exclaimed while in disinhibited states. During fits of deep emotion, entire phrases may be suddenly and accurately expressed as though impaired circuits have been bypassed.
MSE 76 |
|
|
Causes of aphasia
|
Strokes, tumor, brain surgery, infection, severe head trauma
MSE 76 |
|
|
Aphasia needs to be differentiated from what?
|
difficul.ty with acquiring language in the context of global intellectual impairment, e.g. MR, not aphasia. Language impairment in schizophrenia, delirium, dementia needs to be differentiated from aphasia.
MSE 76 |
|
|
Aprosodia - definition; often accompanied by? Should be differentiated from?
|
loss of prosodic speech. Often accompanied by a decrease in gesturing. SHould be differentiated from alexithymia, in which there is a lack of variation and capacity for recognition of one's various emotional states.
MSE 76 |
|
|
Aprosodia - associated lesions
|
Some pts with R hemispheric lesions may be both alexithymic and aprosodic
MSE 76 |
|
|
Phoneme
|
the smallest units ofspeech that are comprised of vowels and consonants
MSE 76 |
|
|
Articulation - definition
|
the ability to pronounce phonemes clearly and distinctly
MSE 76 |
|
|
What is responsible for articulation?
|
vocal activity is shaped by the actions of the muscles of speech, including the lips, tongue, palate, and cheeks.
MSE 76 |
|
|
Impaired ability to articulate is termed?
|
dysarthria
MSE 76 |
|
|
Types/examples of sounds
|
labial - b, p, m, w, u, o
Lingual - l, d, n, s, t, x, z Palatal - b, d, m, n, g, k Each of these anatomic areas needs to be functional and coordinated in order to produce the different sounds of speech. MSE 76 |
|
|
Altered articulation - causes
|
Any d/o that affects orophraryngeal musculature, such as paralysis, stroke, MS, Bell's palsy, dystrophies, Friedreich's ataxia, extrapyramidal d/o
MSE 76 |
|
|
Cluttering - definition
|
nonfluent speech abnormality that is jerky and rapid, using phrasing patterns that do not relate to grammar; inappropriate pauses and bursts of words. speech can be unintelligble and is often rapidly paced.
MSE 76 |
|
|
Cluttering - occurs when?
|
this pattern usuallyy begins in childhood and may persist into adulthood.
MSE 76 |
|
|
Conduction aphasia - definition, associated lesions, characteristic errors
|
type of fluent aphasia caused by lesions of association fibers b/w Broca's and Wernicke's areas (including arcuate fasciculus). Many paraphasic errors, impairment of confrontational naming, reflected in both written/spoken language. Inability to repeat words and to read aloud. Comprehension is intact.
MSE 76-7 |
|
|
Coprolalia; seen in?
|
compulsive and explosive profanity or obscenities; most commonly seen in Tourette's, also seen in schizophrenia
MSE 77 |
|
|
Dysarthria - definition, cause
|
speech that is poorly articulated b/c of damage to/dysfunction of anatomically peripheral apparatus used to form words/sounds - tongue, mouth, palate, lips, throat, muscles of face. These mm may be weak or poorly coordinated.
MSE 77 |
|
|
Dysarthria - presentation, errors
|
speech may be slurred, certain consonants enunciated improperly, e.g. b/p substitutions. Errors include distortions, omissions, ssubstitutions, additions.
MSE 77 |
|
|
Dysarthria - differentiate from what?
|
differentiate from aphasia or dysphasia. Can have dysarthria and Broca's if mm of oropharynx are also directly affected, as in stroke in a large area of dominant frontal lobe.
MSE 77 |
|
|
Dysarthria - causative lesions, disorders
|
large stroke causing Broca's and affecting mm of oropharynx; subcortical lesions, as in parkinsonism and brainstem strokes; peripheral damage to nerves or muscles. In children, a host of congenital disorders that affect development of peripheral speech anatomy can cause dysarthria
MSE 77 |
|
|
Dysgraphia - definition
|
impairment in the ability to produce written language
MSE 77 |
|
|
Causes of dysgraphia
|
Motor (praxis) or linguistic defect. Motor defects are evidenced by poor-quality handwriting or visual-spatial abnormalities (such as letters and words not arranged correctly on page or running off edge of page), substitutions of similar letters (b for p), or perseveration of same letter. Deficits typically parallel the deficits in speech, including word-retrieval errors, paraphasias, agrammatism
MSE 77 |
|
|
Dyslexia - definition
|
defect in acquired abilities related to written language, including reading, writing, spelling.
MSE 77 |
|
|
Dyslexia - intelligence, comprehension, motor sensory systems?
|
Most individuals have normal intelligence, can comprehend language, have intact primary motor and sensory systems.
MSE 77 |
|
|
Dyslexia - types/deficits
|
dewficits are in visual or verbal memory
MSE 77 |
|
|
Visually-related dyslexia
|
seem to have a perceptual defect in that they cannot recognize shapes of letters, miss entire sections of sentences, transpose letters, or have difficulty scanning from left to right
MSE 77 |
|
|
Verbally mediated dyslexia
|
Cannot read aloud, make paraphasic errors
MSE 77 |
|
|
Dyslexia – etiology
|
Usually a developmental learning disability, often genetic. May be acquired as part of an aphasic disturbance
MSE 77 |
|
|
Echolalia
|
inappropriate, parrotlike repetition of another person’s spoken words
MSE 78 |
|
|
Echolalia – clinical associations
|
occurs in severe schizophrenia, catatonia, transcortical aphasia, some dementias
MSE 78 |
|
|
Fluent aphasia – most common type
|
wernicke’s
MSE 78 |
|
|
Fluent aphasia – prosody, grammatical structure, meaning
|
Prosody and grammatical structure apparent, cadence and rhythm sound normal, syntax usually correct, but communication is devoid of meaning. Expression contains word retrieval gaps and many paraphasias, and lacks semantic content. Speech rambles, wanders, often in pressured fashion (logorrhea). No insight. Can have neologisms
MSE 78 |
|
|
Fluent aphasias – writing
|
writing affected similarly to speech, with many paraphasic errors
MSE 78 |
|
|
Hypergraphia
|
A tendency to write excessively
MSE 78 |
|
|
Hypergraphia – seen in? Famous example (allegedly)?
|
seen classically in pts with temporal lobe epilepsy. These pts write idiosyncratically on special topics and in great detail. Dostoyevsky’s writing believed to be affected by his epilepsy in this way. Schizophrenics and manics may also exhibit this.
MSE 78 |
|
|
Mutism – definition
|
lack of verbal communication
MSE 78 |
|
|
Mutism occurs electively in?
|
children, deaf people
MSE 78 |
|
|
Mutism – causes
|
catatonia, conversion d/o, locked-in syndrome, end-stage dementia (notably primary degenerative types, e.g. Alzheimer’s, Pick’s). Large L frontal infarctions involving supplementary motor area may also produce this
MSE 78 |
|
|
Nonfluent aphasia – MC type
|
Broca’s, in which expression of language is predominantly impaired, while functional comprehension is mostly intact. They are impaired in tests of syntactic comprehension.
MSE 78 |
|
|
Nonfluent aphasia – characteristics of speech
|
fluency of expressed language severely reduced, grammar (syntax) significantly impaired). Speech somewhat dysarthric, telegraphic, often monosyllabic, with poorly controlled volume, little intonation. Requires great effort to initiate conversation. Pts frustrated by disability.
MSE 78 |
|
|
Nonfluent aphasias – intact speech
|
relative preservation of ability to speak automatized, well-learned sequences of words, e.g. months of years. Expletives may also be produced easily.
MSE 78 |
|
|
Nonfluent aphasias – writing
|
similarly affected, with misspellings, omitted words (especially connecting words). Ability to copy written material is intact).
MSE 78-9 |
|
|
Broca’s aphasia – associated lesion
|
located anteriorly, in third convolution of frontal lobe of language-dominant hemisphere (left side in most persons). Paralysis/weakness of limbs may be concurrent, depending on extent of frontal lobe lesion. Writing must often be tested using nondominant hand.
MSE 79 |
|
|
Difference between transcortical sensory aphasia and Wernicke’s? B/w transcortical motor aphasia and Broca’s?
|
In each case, the former has preservation (relative or absolute) of repetition.
MSE 79 |
|
|
Paraphasia – definition, types
|
substitution of a letter or word for an intended letter/word. Can be literal (phonemic) or semantic
MSE 79 |
|
|
Literal (phonemic) paraphasias
|
an unintended substitution of a sound or syllable occurs (m for b, moat for boat), despite proper articulation
MSE 79 |
|
|
Semantic paraphasia
|
the substitution is of a word that is semantically related (wife for mother, clockhand for wristwatch)
MSE 79 |
|
|
Paraphasias occur in?
|
conduction, anomic, Broca’s and Wernicke’s aphasias; dementias, delirium, sleep deprivation, other disorders involving word-finding difficulties.
MSE 79 |
|
|
Phonation – definition
|
production of speech due to vocal cord vibrations and activity of respiratory and laryngeal muscles; these determine loudness, quality and pitch of spoken language. Flow of air past vocal cords forms the sounds of spoken language
MSE 79 |
|
|
Impairment in phonation – What causes speech that is well articulated but whispered?
Hoarseness? Altered pitch? |
well-articulated but whispered – laryngeal cancer
Hoarseness – nodules on vocal cords Altered pitch – flu MSE 79 |
|
|
Aphonia – definition; what does/doesn’t cause it?
|
loss of voice. Not caused by cortical lesion, but by peripheral problem, e.g. involving vocal cords or ability to breathe effectively.
MSE 79 |
|
|
Pragmatics – definition
|
communicative value of language beyond meaning derived from syntax, prosody, phonology, semantics.
MSE 79 |
|
|
Pragmatics – related part of brain
|
R hemisphere involved in appreciation of these more abstract levels of language communications.
MSE 79 |
|
|
Pressured speech – definition
|
speech that is particularly “driven” in amount, rate, and often loudness, as though pt is compelled (pressured) to produce large amounts of speech in a short time.
MSE 79 |
|
|
Pressured speech occurs classically in? Also in?
|
Classically associated with mania or in d/o that include manic Sx, e.g. schizoaffective d/o or mood d/o 2/2 medical illnesses or CNS dz. May be accompanied by flight of ideas.
MSE 79-80 |
|
|
Pressured speech also seen in?
|
Also to some extent in pts who are very anxious, under great stress, and in hyperthyroidism.
MSE 79 |
|
|
Scanning speech – definition
|
Nonfluent speech that is slowed and deliberate, with irregular emphasis on syllables.
MSE 80 |
|
|
Scanning speech – significance
|
reflects cerebellar dysfunction, as in multiple sclerosis, post-trauma, chronic alcoholism
MSE 80 |
|
|
Semantics – definition
|
context/meaning imparted by language.
MSE 80 |
|
|
Semantics determined by?
|
Sentences impart meaning in part through the words that comprise them, but also through their varying grammatical structures (phrases, commas, etc.)
MSE 80 |
|
|
Examples of semantics affected by punctuation
|
Compare Finally, serve the dessert vs The dessert was finally served. Or The steak was well done vs. The steak was done well.
MSE 80 |
|
|
Stuttering – definition
|
Motor speech disorder characterized by involuntary repetition of words or phrases, including part-words, inappropriate prolongation of sounds or syllables, and abrupt halting. Disturbance of normal fluency and timing of speech.
MSE 80 |
|
|
Stuttering – how common? Etiology? Worsened by?
|
Relatively common d/o w/ various etiologies, inc. developmental deficit (most common), stroke, head injury, and psychologic abnormalities. Frequently worsened by anxiety.
MSE 80 |
|
|
Tic, vocal type
|
sudden, brief, unexpected, stereotyped, repetitive, involuntary vocalization of nonlinguistic sound. Inc. coughing, grunting, snorting, variety of guttural sounds. If words uttered - considered verbal type. Common in Tourette's
MSE 80-1 |
|
|
Word deafness
|
Inability to comprehend anything spoken, though speaking, reading and hearing are intact
MSE 81 |
|
|
Word deafness - causative lesion
|
usually due to a lesion in left temporal lobe or b/l superior temporal lobe lesions
MSE 81 |
|
|
Word deafness - differentiate this from what?
|
Wernicke's and deafness
MSE 81 |
|
|
Word-finding difficulty - definition, clinical associations
|
inability to recall words or names of things spontaneously when engaged in conversation or during confrontational naming. Seen in pts suffering from aphasia, dementia, brain damage, anxiety, and sleep deprivation
MSE 81 |
|
|
Word salad
|
term applied to extremely psychotic patients whose communications are incomprehensible and incoherent, as their words do not relate to each other in any meaningful way and may not be in proper syntactical relationships
MSE 81 |
|
|
Word salad - differentiate from?
|
may be difficult to distinguish from fluent aphasia
MSE 81 |