Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
What are the 3 main injuries that occur to bones of the legs?
|
1. Subluxation = 2 component parts of the joint stetch apart but return again
2. Dislocation = part of joints come apart and do not return. 3. Sprain = in between - stretching of the ligaments |
|
|
Why are acetabular fractures serious?
|
Intra-articular fracture to acetabulum very serious = necessary for integrity of joint and thus leads to arthritis and therefore will always be put back together surgically.
|
|
|
Give 3 possible complications of pelvic fractures
|
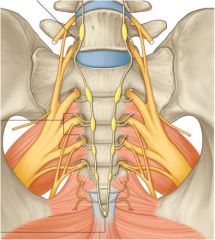
1. Considerable blood loss = high potential from both arteries and veins. Tends to occur at the back of the pelvis as vessels are adherent to bone and have less freedom of movement.
2. Abdominal injury = especially if crushing force → caecum and sigmoid colon. Bladder and urethra in male adherent to the pelvis so can be ruptured if anterior fracture 3. Nerve injuries common associated with pelvic fractures = especially in sacral fractures as femoral nerve runs on front of psoas major. |
|
|
Describe fractures of the ilium
|
• Ilium usually shattered by force laterally and causes significant blood loss.
• Occurs in side-impact car accidents (although many cars have side-impact airbags now). • Falls onto side by elderly most common |
|
|
Describe fractures of the pubis
|

• Fracture either one or both rami by anterior force.
• Most fractures close to the pubic symphysis but not too serious. • However, if disrupt pubic symphysis both sides of pelvis completely disrupted = can injure pelvis, diaphragm, sacro-iliac joint etc by direct blow into midline |
|
|
What is an open-book fracture dislocation?
|

• Normal sacro-iliac joint is a thinnish curvy line, but in this injury there is a large gap = open-book fracture dislocation of the sacro-iliac joint.
• Foot externally rotated. Found in conjunction with a disruption of the pubic symphysis • Can cause damage to sciatic nerve and sacral spinal nerves which are pulled. • Put large sling around to cut off bleeding and pull wings in initially. Later surgically use external fixator laterally and metal plate anteriorly (potentially with a bone graft at the PS) |
|
|
Describe acetabular fractures
|
• Intra-articular fracture
• Like a hammer and anvil femoral head can be driven into depth of socket due to a lateral impact (car accident) • Falling onto straight legs = vertical blow which causes vertical split into acetabular roof |
|
|
Describe the prevalence of neck of femur fractures
|
• 20% of all orthopaedic bed occupancy
• 1998 38,000 • 2015: 120,000. • Rehab difficult so high mortality rates in elderly patients = 80% of >75 years die within 18 months |
|
|
How is osteoporosis related to neck of femur fractures?
|
• In osteoporosis bones are weakened so normal amount of force will fracture an elderly bone as trabeculae in cortex thinned.
• Fracture may be caused by a fall but can simply give way as a stress fracture. • Often occurs bilaterally so important to check both sides. • Stress lines rise through centre of neck of femur so common place for break |
|
|
Describe the blood supply to the head of the femur
|
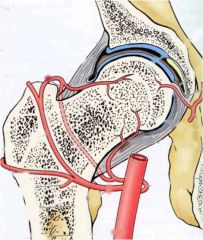
Blood supply of femoral head precarious, mostly arising inferiorly and stuck to the side of bone. So if get fracture to neck will disrupt supply, causing avascular necrosis
|
|
|
What are the 2 classifications of neck of femur fractures?
|
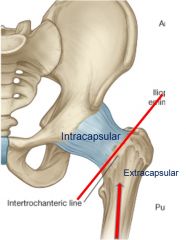
1. Intracapsular = presdisposition to injury of blood supply. Must be fixed and screwed but in many cases better simply to put in prostheses immediately = hemi-arthoplasty. However, bone is quite soft and may migrate through, and so in younger elderly give a whole hip replacement
2. Extracapsular = less likely to result in avascular necrosis. Need counter-balance along bone to hold shaft in place |
|
|
What are the 2 types of intracapsular fractures?
|
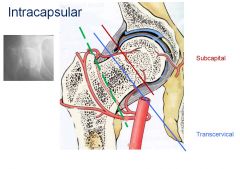
1. Subcapital 2. Transcervical
|
|
|
What are the 2 types of extracapsular fractures?
|
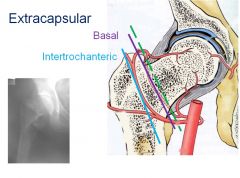
1. Basal (base of neck) 2. Intertrochenteric
|
|
|
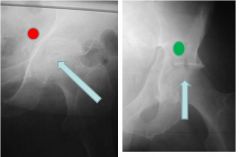
Describe the position of the lower limb in neck fractures and who is most at risk from this type of fracture?
|
• Leg shortened and externally rotated (nothing holding head into socket so muscles pull leg externally as no opposition). This can also occur in hip dislocation.
• The younger the patient the greater the risk of neck fractures to the blood supply and greater the risk of AVN as greater force required to break the bones (especially serious in children) |
|
|
Describe how traumatic hip dislocation can occur
|

• Very difficult and requires high amount of force as held by strong ligaments, capsule and surrounding muscles.
• When dislocated, requires massive amount of force to put into place as muscles surrounding it go into spasm. • Direct blow e.g. when sitting with knees up pushes the femoral head out of socket and often causes posterior fracture of acetabulum. • If don't reduce hip within 6 hours of dislocation can cause chondrolysis (due to lack of synovial fluid food), avascular necrosis of bone and eventual denerative arthritis |
|
|
Describe the features of a sciatic nerve injury
|

• Can be damaged by stretching alone.
• Supplies hamstrings and all muscles from the knee downwards → lose all movements below the knee (causing foot drop), paralysis of the hamstrings and skin innervation to most of the leg (except for the medial side) if cleaved |
|
|
Describe femoral shaft fractures and their treatment
|

• Children commonly fracture diaphysis and may lose much blood as profunda femoris winds around the shaft.
• Treatment: - Use Thomas splint = effective but must stay in beds for 8-12 weeks and will thus get some loss of fucntion. - Use intramedullary nail = put bone into correct position and patient up and moving within 2-3 days but problems with surgery and can be risky as hard to get correctly aligned. - Can aslo use metal plates or external fixation (but problems with infection) |
|
|
Describe patellar fractures
|

• Usually results from a direct blow.
• Intra-articular fracture. • Will not join spontaneously as quads will pull apart. • Get loss of knee extension and haemoarthrosis. • Use patellectomy so can get moving again but difficult if communited fractures as must align |
|
|
Describe fractures to the tibial plateau
|
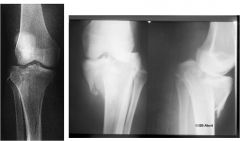
• Blood vessels posteriorly often damaged (posterior tibial artery).
• Leg will collapse and will result in valgus deformation if lateral tibial plateau fracture or varus if fracture of medial tibial plateau. • Can also get meniscal damage and will often lead to early osteoarthritis if don’t fix valgus/varus deformity |
|
|
Describe neck of fibula fractures
|
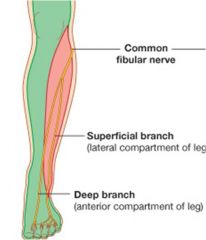
• No knee articulation.
• Common in footballers = due to direct blow or rotation. • Common fibular nerve attached to the head so effects anterior and lateral leg compartments → loss of dorsiflexion and eversion (causing foot drop and inversion) and catch toe on ground so must lift leg to walk (high-stepping gait). • Ask patient to dorsiflex big toe = EHL and check sensation of web of big toe = indicates that at least deep part of fibular nerve damaged and likely to be both (innervates anterior and lateral aspects of the leg and foot = medial supplied by saphenous) |
|
|
Describe tibial shaft fractures
|

• Sporting injuries = direct blow → transverse fracture.
• Rotational strain may cause spiral fracture in tibia, which may cause a fracture in the head of the fibular and tearing of the I-O membrane, causing large bleed. • External immobilisation and internal immobilisation with nails to stabilise |
|
|
What is compartment syndrome are what are the signs and symptoms?
|

• Very important to consider in tibia and fibula fractures.
Finite space in the compartments → If pressure in the compartment exceeds that of the blood being pumped into the compartment, will stop flow, so can get AVN of the muscles in that compartments. • Look for pain, pallor, pulse, pain, paraesethia (5 P's). • Pain most significant symptom = unresponsive to painkillers and not proportionate to procedure done. • If untreated will get permanent dropped foot. |
|
|
Describe ankle fractures and their treatment
|

• Intra-articular fracture.
• Ankle mortice formed by medial and lat mallolus holding in talus, so any damage to one of these can cause OA. • Potts fractures = disruption to both med and lat malleolus with displacement of ankle joint. • Need to put in a plate laterally and screws to hold the joint together. Vital to restore anatomy to allow walking. • Can get compartment syndrome in the foot, or swelling in the ankle can prevent access of the dorsalis pedis = NV complications |
|
|
What is an ankle sprain?
|
• Not really an ankle sprain = inversion and eversion through subtalar joint not ankle joint.
• Occurs usually through inversion = go over foot and stretch ligaments (anterior talofibular ligaments). • Fibular muscles tendons over here and can be stretched on inversion, so this action can fracture 5th MT base where FB inserts |
|
|
Describe an Os Calcis Fracture
|
•• Intra-articular element of injury as forms the subtalar joint superiorly, so if fracture os calcis upwards can become intra-articular = leads to OA in 20 years.
• Can also get extra-articular fractures • Need to fuse joint → stiffness but no pain |
|
|
When do fractures of the 5th metatarsal occur?
|
Fibularis brevis can pull off the base of 5th MT if stretched e.g. In hyper-inversion = common sports injury. If put in plaster can cause DVT
|