Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
45 Cards in this Set
- Front
- Back
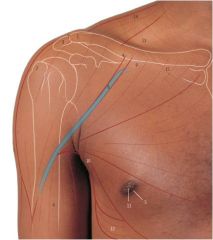
What is number 8, and what is its significance?
|
Cephalic vein running through delto-pectoral groove
- Significant as can put in IV fluids here and an important place for incisions into the shoulder |
|

What are the significance of these marked places?
|
- Sites of veins used for blood taking and intravenous cannulae
|
|
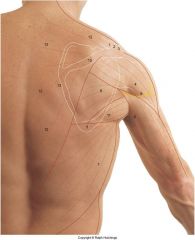
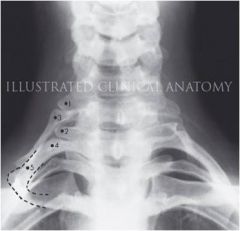
Label this diagram
|
1 - Clavicle
2 - Acromioclavicular joint 3 - Acromion 4 - Deltoid 5 - Inferior angle scapula 7 - Latissimus dorsi 8 - Axillary nerve 9 - Triceps brachii 10 - Spine of scapula 11 - Teres major 12 - Trapezius |
|
|
Describe the areas and reasons for injecting into the arm
|

1. Intramuscular / subcutaneous injections = e.g. for vaccinations. Carry out on anterolateral arm → important not to go too posteriorly as may hit axillary nerve, causing deltoid problems
2. Intra-articular injections = fluid removal, steroids insertion e.g. in treatments of arthritis. Important to angle needle laterally rather than medially to make sure brachial plexus is not involved. May also be used as site of athroscopy e.g. in ligament repair |
|
|
Describe the arterial supply to the scapula and why it is clinically significant
|
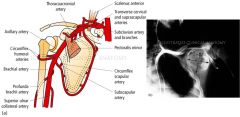
- Shoulder forms anastomsis aorund the borders of the scapula
- Branches of the subclavian artery = subscapular, and the axiallary artery = circumflex scapular artery |
|

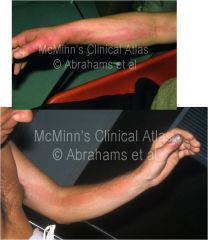
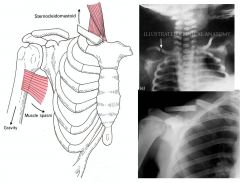
What is this indicative of?
|
Axillary vein thrombosis → blockage of axillary vein pumps blood around the anastomsis around the scapula, producing a swollen scapula
- Hands clearly show a slower venous return as more congested and redder |
|
|
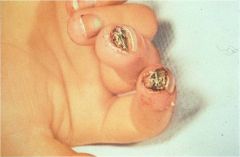
Describe the lymphatics of the upper limbs
|
- Drain towards into the supratrochlear node, which drains into the lateral axillary node (→ central → apical)
- Lymphodema = occurs following mastectomy → blockage of lymph up arm as no drainage and swelling - Lymphangitis = thumb/hand infection. Inflammation of the lymphatic tubes due to infection, draining up the arm to the lateraly axillary nodes → red line of rash following duct - Malignant melanoma of nail often presents first by enlarged axillary nodes |
|
|
Why is the clavicle an exceptional bone and what happens when it is not formed?
|

Exceptional because:
- No medullary cavity - Ossified during the 5-6 week ofter conception and first to do so in the embryo - Develops in membrane in contrast to other long bones which have an endochondral ossification - The most fractured bone in the body, and often caused by a fall on outstretched hands • When clavicle is missing = clap shoulders → no significant problems |
|
|
Describe the dynamics of a clavicle fracture
|
- The weakest point in the clavicle is where the middle and lateral thirds join and the bone usually fractures at this point
- The subclavian vessels and brachial plexus lie posterio to middle third of the clavicle and can be damaged - However, the large vessels and nerves are separated and protected from clavicle fractures from subclavius - After fracture, the sternocleidomastoid can pull the medial fractured end upwards, so that there is no longer apposition - Consequently, even if they are reset, there may always be a lump after healing of the bone |
|
|
Describe the anterior peripheral nerves of the arms
|
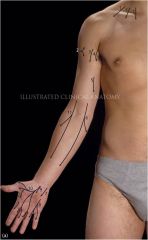
Named “mixed” nerves of
upper arm: - Supraclavicular ns. - Upper lat cut n. - Intermediate cut n. - Intercostobrachial n. - Medial cut n. - Medical cut n of Forearm - Palmar br Ulnar n. - Ulnar n. - Palmar br of Median - Median N. |
|
|
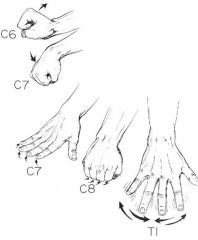
Describe the dermatomes of the arms
|

Note: the dermatomes are variable and overlap
|
|
What nerve has been damaged here
|
Median nerve → if lesions are in hand it is important to examine all the way from the neck (cold fingertips in just a few fingers may also be indicative of nerve problem)
|
|
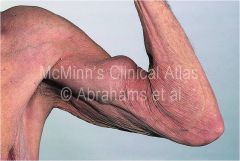
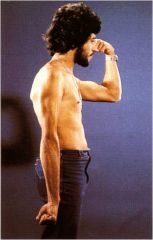
What is this?
|

- Rupture of the long head of biceps brachii
- Often in individuals who have used steroids which weaken muscles, or are elderly |
|
|
What are the muscles that cause lateral and medial rotation of the arm?
|
- Lateral rotation (backhand = external) → infraspinatus, teres minor, posterior deltoid
- Medial rotation (forehand = internal) → subscapularis, latissimus dorsi, teres major, pectoralis major, anterior deltoid |
|
|
What is supraspinatus syndrome?
|
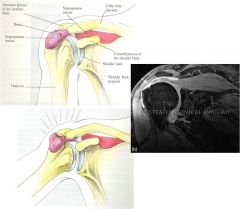
- Tear in the supraspinatus tendon
- Causes painful arc on abduction - Commonly damaged in sports that involve lots of lateral rotation and runs under the acromion |
|
|
What is subacromial bursitis?
|

- Subacromial bursa sits between the supraspinatus tendon and the acromion
- Can become inflammed by rubbing of the tendon, causing inflammation of the tendon - This inflammation can be seen using a subacromial bursagram with contrast medium - Treat with drainage of exudate and injection of steroids into bursa |
|
|
Describe the effects of lower brachial trunk injury
|
- Klumpke's paralysis
- May be caused by a cervical rib, which compresses the inferior trunk and the T1 nerve root (thoracic outlet syndrome) - T1 goes to all intrinsic hand muscles so these are particularly affected, causing the wasting for the 1st dorsal interosseous muscle visibly |
|
|
Describe upper brachial trunk injury
|
- Commonly caused by speedway motorcycle accidents or to newborns during differcult breach deliveries (here innervation usually returns in under a year)
- Damage to upper trunk of brachial plexus = C5/C6 - Produces Erb's point/palsy, permanently flexing the wrist in the 'waiter's tip' position |
|
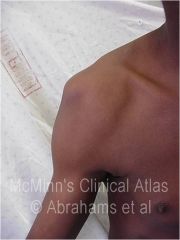
What is this and what may be its cause?
|
- Flattened deltoid
- Caused by damage to the axillary nerve - Caused by fracture/dislocation of the neck of the humerus - Consequently, it's vital to check the abduction of the arm and the sensory innervation over the regimental patch area |
|

What is this and what causes it?
|
- Damage of the radial nerve → unable to extend wrist or fingers and lose control of opposition = wrist drop
- Caused by mid-shaft fracture as the radial nerve runs in the spiral groove - Only sensory loss to a small area of skin on the dorsum of the hand near the thumb → over first dorsal interosseous muscle (so grip impaired) |
|

What is this and what is its cause?
|
- Damage to ulnar nerve → claw hand by unable to extend medial 2 fingers
- Also lose sensory innervation of the medial 1 1/2 fingers on both anterior and posterior surfaces |
|

What is this and what is the cause?
|

- Median nerve damage
- Median nerve runs along with the brachial artery and enters the carpal tunnel where it gives off a recurrent median nerve branch for LLOAF muscles - Causes thenar wasting, inability to open a bottle etc as cannot oppose nor abduct thumb - Also lose sensory innervation to 3 1/2 fingers |
|
|
Why are lumbricals atypical muscles?
|
- No attachment to bones = origin on the 4 tendons of FDP and inserts in to the extensor expansions of the fingers
|
|
|
Which myotome would you test if you suspected lumbrical and interossei weakness?
|
- All hand intrinsic muscles e.g. lumbricals and interossei are innervated by T1 myotome (although these may be transported in different nerves)
- Interossei and lumbrical weakness may present with weak abduction and adduction of the fingers, and may suggest a cervical rib |
|
|
Where do the palmar digital nerves lie and why is this important when anaethetizing?
|

- Palmar digital nerves lie down equators of the fingers on either side, medial to digital arteries
- This is important as inject too medially and you may damage the flexor tendon, but inject too laterally and may hit artery - Remember that must inject bilaterally |
|
|
Where does the ulnar nerve run in the forearm and what does it innervate?
|

- Arises medial to the brachial artery and pierces the medial intermuscular septum to run deep to the medial head of triceps
- Runs in ulnar groove, posterior of medial epicondyle - Enters the forearm between the 2 heads of FCU - Runs deep to FCU on FDP with the ulnar artery on its lateral side - Lies lateral to the tendon of FCU at the wrist and passes superficial to the flexor retinaculum - Divides into its terminal bracnhes at the pisiform - Can be enlarged and tender in leprosy - Innervates all the muscles of the hand except “LLOAF” ie. most intrinsic hand muscles |
|
|
Whjat is Froment's test / sign
|

- Guttering due to loss of interossei
- Indicative of right ulnar nerve damage - Unable to hold a piece of paper in abduction of thumb = positive |
|
|
Describe the path of the median nerve
|

- Runs along lateral to the brachial artery in arm, then crosses it to lie medial to it in the cubital fossa
- Passes between the two heads of pronator teres and gives off anterior interosseous nerve - Lies attached to the deep surface of FDS on FDP - Emerges from lateral side of FDS to give off palmar cutaneous branch - Through carpal tunnel between FDS and FCR - In carpal tunnel it divides into terminal branches (muscular and palmar digital branches) - Recurrent median nerve branch for “LLOAF” muscles - Sensory 3 ½ fingers - Thenar wasting “doc I cannot open a bottle” |
|

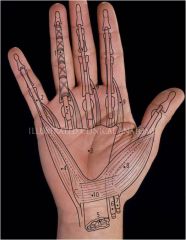
Label this diagram, especially 15, 16, 13, 22, 23, 24
|
15 = Median nerve
16 = Ulnar nerve 13 = Superficial palmar arch 22 = Radial artery 23 = deep palmar arch 24 = Ulnar artery |
|
|
Describe 2 tests for Carpal Tunnel Syndrome
|

1. Tinel's test = Extend wrist and tap retinaculum. If median nerve is restricted will cause pain if CTS
2. Phalen's test = Flex wrists and put dorsum of hands together and will get a nipping pain where median nerve is compressed if CTS |
|
|
What is carpal tunnel syndrome and what is its treatment?
|
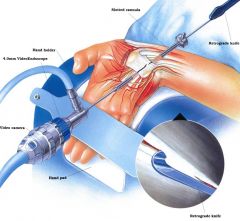
- Carpal tunnel syndrome = decrease in the space in the carpal tunnel e.g. due to infection, hypertrophy of tendons, inflammation → compression of median nerve and pain
- Treatment = mainly drugs, splints etc. Surgery last resort and endoscopic incision of the retinaculum |
|
|
Describe the path of the radial nerve
|
- Descends posterior to the axillary and brachial arteries
- Runs with the profunda brachii in the spiral groove from posterior to anterior (piercing the lateral intermuscular septum) - Enters the cubital fossa and divides into terminal branches of the lateral epicondyle = • superficial terminal branch → lies under brachioradialis and runs with radial artery, passes posteriorly and passes over then tendons of the snuffbox to give cutaneous branches to the hand • Posterior interosseous → passes between the 2 heads of supinator and passes into the posterior compartment to supply muscles here |
|
Label this diagram
|
1 = Synovial sheath
2 = Flexor digitorum profundus tendon 3 = Palmar aponeurosis 4 = Abductor digiti minimi 5 = Carpal tunnel 6 = Flexor pollucis longus 7 = Flexor carpi radialis 8 = Abductor pollucis brevis 9 = Lumbrical 10 = Flexor retinaculum |
|
|
What is a Colles' fracture?
|
- At the distal epiphysis of the radius - may also affect the styloid process of the ulna sa an avulsion fracture
- Common in elderly women who fall - Fibrocartilage attaches the radius and ulnar styloid processes so will break both if detaches |
|
|
Describe the movements at the thumb
|

|
|

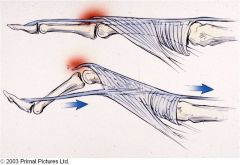
What are the arrows pointing to?
|
Left = Median nerve through the carpal tunnel
Right = Recurrent branch to thenar muscles |
|
|
In radial nerve damage, where does the sensory loss in the hand usually occur?
|
- Although innervates a portion of the hand, there is a degree of overlap with the ulnar and median nerves, so the only real sensory loss is usually over the 1st dorsal interosseus muscle
|
|
What is this?
|
Dupuytren's contracture = tightening of the palmar aponeurosis
- Operative = cut palmar aponeurosis to stop little finger folking down |
|

How are these pictures linked?
|
1st = Paronychia → the funger is infected
2nd = synovial bursitis which may be caused when infection at the finger drains through the synovial bursa (especially in the little finger) |
|

What is this?
|

A ganglion synovial hernia
- A cystic, round, usually non-tender swelling located along tendon sheaths or joint capsules - Frequent sites: dorsum of the wrist, palmar wrist crease, ankle |
|
|
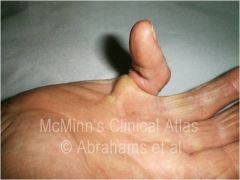
What is gamekeeper's thumb?
|

- Common in skiiers
- Torn 1st MCP ligament |
|

What is this?
|
- Mallet finger
- Common in baseball players (going for base) and bicycle accidents - Avulsion of extensor attachment +/- fracture of terminal phalanx |
|

What is this?
|
Boutonniere deformity
- Avulsion of the extensor median cord, but not of the lateral, so that the phalanx is pulled up like a button hole - Common in RA as tendons are weakened |
|
|
What is Allen's test?
|

- Block the radial and ulnar arteries
- Release ulnar artery and check the blood flow returns (hand turns red) - Recover and so same for radial - Must be done before hand surgery and before injecting into the hand |
|

What is this?
|
= Raynaud's syndrome/disease
- Very common in women - Poor circulation → blue/white hands in winter and in severe cases may lead to ischaemia |