Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
33 Cards in this Set
- Front
- Back
|
Describe the mechanical and physiological functions of bones and the skeleton
|
- Mechanical
1. Support 2. Protection 3. Movement = joints, motor power, neurological control - Physiological 4. Haematopoiesis = long bones, pelvis and ribs 5. Mineral homeostasis = Calcium and phosphate |
|
|
What are the 2 major types of bone?
|
1. Cortical = dense bone built for strength. Arranged in Haversian systems
2. Cancellous bone = spongy, trabeculated bone, light weight |
|
|
Describe the classification of bone by shape and their significance
|
Bones may be:
- Long - Short - Flat - Irregular - Sesamoid - Accessory and heterotrophic bones - Shape is significant as shows bones role e.g. clavicle is long and curved to act as a bone strut, connecting the axial and appendicular skeletons. Also signifies the forces running along that bone |
|
|
Describe the structural and functional classification of joints
|
1. Fibrous joints = surfaces jointed together by fibrous tissue
- Sutures = occur only in the skull where adjacent bones are linked by a thin layer of connective tissue termed a sutural ligament - Gomphosis = occur only between the teeth and adjacent bone-in these joints, short collagen tissue fibers in the periodontal ligament run between the root of the tooth and the bony socket - Syndesmosis = joints in which two adjacent bones are linked by a ligament, for example, the ligamentum flavum, which connects adjacent vertebral laminae, or by an interosseous membrane, which links, for example, the radius and ulna in the forearm 2. Cartilagenous joints - Synchondrosis (primary cartilagenous) = where two ossification centers in a developing bone remain separated by a layer of cartilage, for example the growth plate that occurs between the head and shaft of developing long bones, or costal cartilages connecting to the sternum - Symphysis (secondary cartilagenous) = where two separate bones are interconnected by cartilage-most of these types of joints occur in the midline and include the pubic symphysis between the two pelvic bones, and intervertebral discs between adjacent vertebrae 3. Synovial joints = elements involved connected by a narrow articular cavity - The joint is surrounded by a joint capsule = dense connective tissue - Lined by synovial membrane - Producing synovial fluid for nutrition and reduction in friction - The joint has a joint cavity - The articular surfaces are covered in hyaline cartilage |
|
|
Describe the 2 layers of the synovial membrane
|
1. Intima (closest to joint cavity) = cells phagocytic or secretory → secretes proteoglycans and enzymes
2. Sub-intima = highly vascular loose connective tissue. Produces synovial fluid from filtered plasma seeped from the blood vessels |
|
|
Describe the classification of synovial joints
|
Classified by shapes and movements:
- Plane = permits gliding movements e.g. acromioclavicular joint - Pivot = permits rotation e.g. atlanto-axial joint - Hinge - permits flexion and extension e.g. humero-ular joint - Condyloid - permits 360 degree movement in a single plane (biaxial) e.g. metacarpophalangeal joint - Saddle = can move up and down with limited movement e.g. trapezo-metacarpal joint - Ball and Socket - permits a full range of movement in all planes e.g. hip joint |
|
|
What is the origin and insertion of a muscle?
|
- Origin = End of a muscle usually remaining fixed during contraction (usually proximal attachment)
- Insertion = end of a muscle usually moving during contraction (usually distal) |
|
|
Define agonist and antagonist
|
- Agonists = prime mover i.e. the main muscle causing a movement
- Antagonists are muscles producing the opposite movement to the agonist |
|
|
What is a synergist?
|
Assists prime mover in achieving the specific movement in a situation where prime mover is capable of activating more than one movement.
|
|
|
What is a fixator?
|
Steady proximal parts of a limb while movements occur in distal parts
|
|
|
Describe 7 ways of naming muscles
|
1. Location e.g. tibialis anterior
2. Size e.g. gluteus maximus 3. Number of origins e.g. biceps brachii 4. Shape e.g. serratus anterior 5. Origin and insertion e.g. sternomastoid 6. Action e.g. adductor longus 7. Direction of fibres e.g. transversus abdominis |
|
|
What are the roles of the clavicle?
|
1. Strut = allows movement
2. Attachments for muscles 3. Transmits force from the upper limb - The only horizontal bone in the body - Subcutaneous in whole length |
|
|
Where are fractures most likely on the clavicle?
|
- Most commonly fractured long bone
- Fractures usually along weak point = between lateral and middle thirds |
|

Label this diagram and side the clavicle
|
1. Lateral end = articulation with acromion
2. Conoid tubercle 3. Shaft of clavicle 4. Muscle attachment of subclavius 5. Medial end = articulation with sternum - Left clavicle |
|

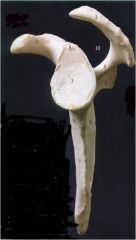
Label this diagram
|
1. Acromial angle
2. Acromion 3. Coracoid process 4. Inferior angle 5. Infraspinous fossa 6. Lateral border 7. Glenoid fossa 8. Medial/vertebral boder 9. Neck of scapula 10. Spine of scapula 12. Superior angle 13. Superior border 14. Suprascapular notch 15. Supraspinous fossa |
|

Label this diagram
|
2. Acromion
3. Coracoid process 4. Inferior angle 6. Lateral border 7. Glenoid fossa 8. Medial border 9. Neck of scapula 11. Subscapular fossa 12. Superior angle 13. Superior border 14. Suprascapular notch |
|
Label this diagram
|
1. Acromion
2. Coracoid process 3. Glenoid fossa 4. Inferior angle 5. Infraglenoid tubercle 6. Infraspinous fossa 7. Subscapular fossa 8. Spine of scapula 9. Supraglenoid tubercle 10. Greater scapular notch |
|
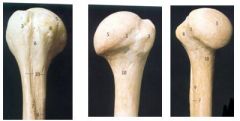
Label this diagram
|
1. Anatomical neck
3. Greater tuberosity 5. Head 6. Bicipital / intertubercular groove 7. Lateral lip of bicipital groove/Deltoid tuberosity 8. Lesser tuberosity 9. Medial lip of bicipital groove 10. Surgical neck |
|

Label this diagram and note the position of the radial groove
|
1. Antero-medial surface
2. Capitulum 3. Coronoid fossa 5. Lateral epicondyle 6. Lateral epicondylar ridge 7. Medial epicondyle 8. Medial epicondylar ridge 10. Olecranon fossa 11. Posterior surface 12. Radial fossa 13. Trochlea |
|

Label this diagram
|
1. anterior border
2. oblique line 3. anterior surface 4. head 5. interosseous border 6. lateral surface 7. neck 8. posterior border 9. posterior surface 11. radial tuberosity |
|

Label this diagram
|
1. anterior border
9. interosseous border 12. styloid process 13. ulna notch |
|

Label this diagram
|
1.anterior border
2.anterior surface 3.coronoid process 4.interosseous border 5.medial surface 6.olecranon 7.posterior border 8.posterior surface 10.supinator crest 11.trochlear notch 12. tuberosity of ulna |
|

Label this diagram
|
1. anterior surface
2. groove for muscle (ECU) 3. head *Note this is distal NOT proximal* 4. interosseous border 6. posterior surface 7. styloid process |
|
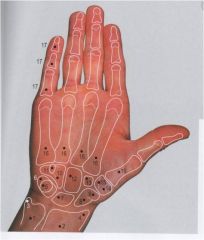
Label this diagram
|
1. ulna
2. radius 3. styloid process ulna 4. styloid process radius 5. pisiform 6. triquetrum 7. lunate 8. scaphoid 9. scaphoid tubercle 10. hamate 11. hook of hamate 12. capitate 13. trapezoid 14. trapezium 16. metacarpals 17. phalanges |
|
|
Describe the prevalence of limb abnormalities
|
- 2/1000 live births
- May have genetics or non-genetic causes e.g. thalodmide - Occur eary = 24-36 days → before a woman necessarily knows she's pregnant |
|
|
What are limb buds?
|
- Form opposite the spinal cord segment that will later innervate them = Upper limbs are C5-T1 and lower limbs are L2-S2
- Outer covering of ectoderm over a core mass of mesenchyme - Upper limb bud develops 1-2 days ahead of the lower limb bud |
|
|
What is the apical ectodermal ridge?
|
- A thickening of ectoderm at the tip of each of the buds
- Synthesises growth factors - Molecules gradually diffuse from the ridge proximally so that there is a gradient of concentration of growth factors from distal to proximal - This triggers differentiation from distal to proximal, so that the hand cartilagenous template forms before the humerus - Thalisomide damges the apical ridge so that there is failed limb development at the point that this occurs |
|
|
Describe 2 abnormalities in limb development
|
1. Amelia = complete absence of whole limb
2. Meromelia = partial absence of limb e.g. hand attached directed onto trunk |
|
|
Describe the formation of the digits
|
1. Flattening of limb buds to form paddle-shaped limbs
2. Formation of 5 thickened and distinct digital rays by rearrangement of cells and selective cell death in the mesoderm 3. Elongation and separation of digits = digits thicken and elongate, and ectodermal cells between them undergo apoptosis, so that almost all disappears except for a small amount at the base of the digit → recognisable hand by 8 weeks 4. Formation of nails = nails form from 8 weeks. Initially forms on the tips of the fingers but migrate backwards onto the dorsal surface → hence why, despite being dorsal they share the palmar nerve supply (nedian and ulnar nerve) |
|
|
Describe 2 congenital abnormalities of the digits
|
1. Polydactyly = too many digital rays form (usually an extra little finger or toe)
2. Syndactyly = fused digits. Of varying severity depending on whether there is incomplete separation of digital rays → complete bony fusion, or incomplete loss of the ectoderm → thin web of skin between the fingers |
|
|
What is pre-axial and post-axial?
|
- The pre-axial border of each limb is cranial and includes the thumb, big toe, radius and tibia
- The post-axial border is caudal and includes the little finger and toe, ulna and fibula |
|
|
Describe the rotation of the limbs
|
- Myoblasts aggregate in each limb bud to form a large muscle mass which separates into dorsal (extensor) and ventral (flexor) components
- To get to anatomical position, the upper limb rotates laterally through 90 degrees on its longitudinal axis. This means that the elbows point posteriorly, the extensors are found posteriorly and the flexors anteriorly - To get to anatomical position the lower limb must rotate medially 90 degrees, so that the knee faces anteriorly, the extensors lie anteriorly, and the flexors lie posteriorly |
|
|
Describe the development of innervation of the muscles and skin of the limbs
|
Skin
- A regular sequence of nerve roots grow out from the developing spinal cord - They supply skin in a regular pattern of strips called dermatomes - Later development distorts this pattern but dermatoms can still be recognised e.g. C5 supplies skin on the preaxial border Muscles - Muscles are innervated in functional groups are nerves grow into the limb and find their muscles - This creates limb plexuses e.g. the brachial plexus - The nerves from the upper limb come from C5 to T1 of the spinal cord, so that the roots of the brachial plexus are C5 to T1 - This regular sequence becomes the brachial plexus: 1. C5 and C6 join to make the upper trunk on the preaxial border 2. C7 remains alone on axis as the middle trunk 3. C8 and T1 join to make the lower trunk on the post-axial border - The muscles are then supplied in anterior and posterior compartments so that each trunk splits into anterior and posterior divisions - These divisions regroup around the axillary artery - All posterior post-axial divisions regroup into the posterior cord - All anterior pre-axial divisions regroup into the medial and lateral cords and |