![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
100 Cards in this Set
- Front
- Back
|
What are 9 key points of clinical anesthesia monitoring?
|
airway/respiratory - circulatory/volume - depth of anesthsia - neurological - muscle relaxation - temperature - electrolytes/metabolic - coagulation - intake/output
|
|
|
What is the ultimate mandate for clinical behavior?
|
the standards of care :-) do you remember them? I-XI . . . name them!
|
|
|
What could lead to contraindications for using a blood pressure cuff on a limb?
|
renal dialysis shunts - IV lines - lymph node dissection - mastectomy
|
|
|
What is the Harvard Standard for blood pressure monitoring?
|
every 5 minutes
|
|
|
What does blood pressure tell us?
|
indicates organ perfusion, although not a direct measure
|
|
|
What is important about the diastolic blood pressure?
|
it's an important variable in coronary perfusion, its the variable in determining hypertension
|
|
|
What is paradoxical blood pressure?
|
A difference in blood pressures between right and left arm - normal is less than 10mmHg difference - greater than 10mmHg may indicate pulmonary or cardiac compromise |
|
|
How do you calculate MAP?
|
[systolic BP + (2 * diastolic BP)] divided by 3
|
|
|
How do you calculate the pulse pressue?
|
systolic - diastolic
|
|
|
What are the proper dimensions of a blood pressure cuff?
|
-cuff width should be 20-50% wider than limb diameter -bladder length should extend at least halfway around the extremity |
|
|
What can cause a falsely high blood pressure?
|
a too narrow cuff -a too small cuff - a loose cuff - an extremity below the level of the heart - uneven compression transmitted to the underlying artery - obesity
|
|
|
What can cause a falsely low blood pressure?
|
too wide cuff - too large cuff - an extremity that is above the level of the heart - quick deflation
|
|
|
What are some complications of non-invasive blood pressure monitoring?
|
petechiae, edema, thrombophlebitis, skin avulsion, nerve palsies, compartment syndrome, mechanical problems
|
|
|
Which patients need continuous ECG monitoring?
|
ALL of them!
|
|
|
Which patients should have a pre-op 12 lead ECG?
|
any patient over age 50 any patient with risk factors over age 40 any other patient with s/s of cardiac disease patients with hx of cardiac ischemia, dysrhythmias, or pacemaker |
|
|
What disorders can be diagnosed by the ECG?
|
cardiac dysrhythmias, MI, electrolyte imbalances, HR, pacer function
|
|
|
What do you know about Lead II?
|
-axis parallels the atria = greatest P wave voltage RA to LL -allows for diagnosis of dysrhythmias and inferioir wall ischemia -most common monitoring lead |
|
|
What do you know about Lead V5?
|
-lies over 5th intercostal space at anterior axillary line -allows you to monitor 7 different leads: I, II, III, AvR, AvL, AvF, V5 -detects anterior and lateral wall ischemia |
|
|
What do you know about a modified V5? |
-used if only 3-lead monitoring available -place left arm lead at V5 location -select lead I or AvL on monitor -detects anterior or lateral wall ischemia |
|
|
Which leads should be monitored ideally?
|
leads II and V5
|
|
|
What kind of monitoring should be done in a healthy ASA 1 patient?
|
3-lead monitoring
|
|
|
Which leads should be monitored in patients with cardiac history?
|
Leads II or V5 5-lead specific to their areas of ischemia |
|
|
Which leads may be the best for detecting maximal ST segment changes?
|
Leads III and V3
|
|
|
Why does ischemia cause changes in the ST segment?
|
the ST segment is usually isoelectric, ischemia causes a loss of intracellular potassium which results in a current of injury
|
|
|
What does a subendocardial injury look like in the ST segment?
|
the ST segment is depressed
|
|
|
What does an epicardial or transmural injury do to the ST segment?
|
the ST segment is elevated
|
|
|
List the acceptable ECG criteria for ischemia
|
>/= to 1mm horizontal ST-segment depression >/= to 1mm upsloping or downsloping ST-segment depression measured 60ms to 80ms from the J point >/= to 1mm ST-segment elevation |
|
|
Where is the J point?
|
at the end of the QRS complex, the ST segment begins at the J point
|
|
|
What do changes in leads II, III, aVF suggest?
|
inferior wall (RCA) ischemia/infarction
|
|
|
What do changes in leads I, aVL, V4-V6 suggest?
|
Lateral wall (left circ) ischemia/infarction
|
|
|
What do changes in leads V1-V3 suggest?
|
anteroseptal ischemia/infarction
|
|
|
What do changes in leads V1-V6 suggest?
|
anterolateral wall ischemia/infarction
|
|
|
What do changes in leads I, aVL, V1-V4 suggest?
|
anterior (LCA) ischemia/infarction
|
|
|
What EKG changes do you see with hyperkalemia?
|
prolonged PR widened QRS peaked T waves |
|
|
What EKG changes do you see with hypokalemia?
|
prolonged PR prolonged QT interval flattened T-wave U waves |
|
|
What is used to continuously monitor heart and lung sounds?
|
a weighted precordial or esophageal stethoscope *the esophageal stethoscope is inserted 28-32cm from teeth* |
|
|
What patients need urinary output monitoring?
|
Pts with CHF, renal failure, advanced liver disease, shock *Dependent on procedure: long cases, cardiac, aortic, renal, craniotomy, major abdominal* U.O. is a reflection of kidney perfusion and function |
|
|
What is the urinary output goal during surgery?
|
> 0.5ml/kg/hour
|
|
|
What does pulse oximetry measure?
|
the ratio of oxyhemoglobin to deoxyhemoglobin, expressed as a percentage
|
|
|
What is plethysmography?
|
a test used to measure changes in blood flow or air volume in different parts of the body - the presence of a pulsatile signal generated by arterial blood - uses a light-emitting diode and a photoelectric cell to detect changes in finger volume |
|
|
What does oximetry depend on?
|
the observation that oxygenated and reduced hemoglobin differ in their absorption or red and infrared light
|
|
|
What is the Beer-Lambert Law?
|
combination of 2 laws Beer's Law: intensity of transmitted light decreases exponentially as the concentration of a substance increases Lambert's Law: intensity of transmitted light decreases exponentially as the distance traveled through the substances increases |
|
|
Red light at 660nm is absorbed by what?
|
Deoxyhemoglobin
|
|
|
Infrared light at 940-990nm is absorbed by what?
|
Oxyhemoglobin
|
|
|
Why is pulse oximetry important?
|
allows for early detection of hypoxemia allows administration of the lowest concentration and flow of oxygen allows for monitoring of circulation |
|
|
Describe methemoglobin
|
an oxidation product of hemoglobin that forms a reversible complex with O2 and impairs the unloading of O2 to tissues - contains ferric instead of ferrous - can be congenital or acquired (from ntg, nipride, prilocaine, lidocaine, sulfas) - absorbs light equally at the red and infrared wavelengths - will be falsely low for O2 sat >85% - will be falsely high for O2 sat < 85% *treatment is 1-2mg/kg methylene blue over 5 minutes - reduces ferric to ferous |
|
|
Describe carboxyhemoglobin
|
occurs in high concentrations from smoke inhalation has an absorption spectrum similar to oxyhemoglobin so most pulse oximeters will overestimate the true SaO2 patients will look cherry red look for acidosis to diagnoses treat with 100% O2 |
|
|
What are some things that can cause inaccurate pulse oximetry readings?
|
stray or flickering light motion artifact nail polish electrical interference prominent pulsations of venous blood high airway pressures during artificial ventilation SaO2 < 80% |
|
|
What does pulsus paradoxus look like in your pleth? What is it a sign of?
|
you have a decreased pleth during inspiration, it's a sign you patient is "dry"
|
|
|
What does capnography measure?
|
Ventilation
|
|
|
What is capnography?
|
the graphic display of instantaneous CO2 concentration versus time or expired volume during a respiratory cycle
|
|
|
What does capnography monitor?
|
alveolar ventilation CO2 production pulmonary perfusion respiratory patterns early indicator of esophageal intubation or airway disconnect |
|
|
What law do CO2 monitors follow?
|
The Beer-Lambert Law
|
|
|
Which light does CO2 absorb?
|
infrared light with a wavelength of 4.3mm
|
|
|
What are the 2 types of CO2 sensors?
|
Nondiverting: adds dead space, adds weight, prone to fluids blocking sensor, located between ETT & breathing circuit Side-stream: no added dead space, possibility of tubing obstruction from vapor, some delay in measurement, suctions gas from breathing circuit into sample, located at ETT T-piece |
|
|
What is the microstream CO2 sensor?
|
a modified sidestream sampling method -has a microbeam IR sensor that isolates CO2 waveform -needs low flow rate (50mL/min) -CO2 molecules absorb IR radiation |
|
|
How is the concentration of CO2 in alveoli determined?
|
perfusion/ventilation (Q/V)
|
|
|
How does EtCO2 correlate to PaCO2?
|
EtCO2 is usually 2-5 torr lower than PaCO2 (reflecting alveolar dead space)
|
|
|
What increases the gradient between EtCO2 and PaCO2?
|
V/Q mismatch alteration in distribution of pulmonary blood flow pts with pulmonary disease |
|
|
What is the first line monitor for detecting malignant hyperthermia?
|
EtCO2 - the increase occurs early, before the rise in temperature
|
|
|
What is needed to generate a CO2 waveform?
|
1) body tissues must generate CO2 2) blood must carry CO2 to the lungs 3) CO2 must be exhaled from the lungs |
|
|
What increases EtCO2 levels?
|
shivering - MH - increased CO - bicarb infusion - tourniquet release - bronchospasm tx - decreased minute volume (hypoventilation)
|
|
|
What decreases EtCO2 levels?
|
decreased muscle activity - hypothermia - decreased CO - PE/cardiac arrest - bronchospasm - increased minute volume (hyperventilation)
|
|
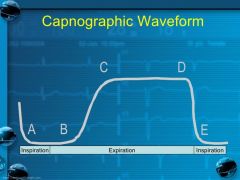
Where is early expiration? Where is end expiration? Where do you measure EtCO2?
|
B is early expiration D-E is end expiration you measure EtCO2 at D |
|
|
Where in the respiratory tract is CO2 zero?
|
in the more proximal respiratory tract, it gets higher the more distal
|
|
|
What part of the lung is more perfused but less ventilated?
|
the alveoli in the lower lung
|
|
|
What could be the reason you no longer have an EtCO2 reading?
|
esophageal intubation disconnect plugged ETT arrest/PE |
|
|
What are some patient conditions that change CO2 production and lead to increased EtCO2?
|
hyperthermia - sepsis - hyperthyroidism - MH - muscular activity
|
|
|
What are some patient conditions that change CO2 production and lead to decreased EtCO2?
|
hypothermia hypometabolism |
|
|
What are some patient conditions that change CO2 elimination and lead to increased EtCO2?
|
hypoventilation - rebreathing - partial airway obstruction - exogenous CO2 absorption - tourniquets - cross clamp removal - bicarb administartion
|
|
|
What are some patient conditions that change CO2 elimination and lead to decreased EtCO2?
|
hyperventilation - hypoperfusion - embolism
|
|
|
What is the anesthesia machine standard?
|
requires that the anesthesia machine be equipped with an O2 analyzer with a high priority alarm that is activated when the measured O2 level is below the user-set alarm threshold (usually set at 30%)
|
|
|
Discuss the standards associated with O2 analysis
|
-O2 readings shall be within plus/minus 3% of actual level -inclusion of humidity and volatile agents shall not cause the O2 readins to vary from actual level by more than 5% -low O2 alarm limit shall not be adjustable or preset below 15% - must be a visual indicator if alarm limit is below 21% |
|
|
What are the standards for measuring volatile anesthetic agents?
|
-readings must be accurate -mandatory high concentration alarms -operator adjustable alarm settings |
|
|
How do we monitor the degree of NMB?
|
by delivering an electrical stimulus near a peripheral motor nerve and evaluating the evoked response of muscles innervated by that nerve
|
|
|
Describe a phase 1 blockade
|
seen with depolarizing NMB - muscle fasciculation followed by relaxation - absence of fade following tetanic or TOF stim - absence of post-tetanic potentiation - potentiation of the block by anticholinesterases - antagonism of the block by non-depolarizing agents |
|
|
Describe a phase 2 blockade
|
seen with non-depolarizing NMBs (or repeated doses of sux) -absence of fasciculations -fade during tetanic and TOF stim -post-tetanic potentiation -antagonism of block by depolarizing agents and anticholinesterases -potentiation of block by other non-depolarizing agents |
|
|
What is fade?
|
when the twitch amplitude decreases from the 1st stimulation, each twitch is weaker than the last, the last twitch is the first to disappear *happens only with NDMB* |
|
|
What are the common monitoring sites for neuromuscular blockade?
|
Ulnar nerve - adducts thumb Facial nerve - closes eyelid, furrows brow Posteriori tibial nerve - flexes big toe |
|
|
What is a single-twitch stimuli?
|
delivery of single impuses separated by at least 10 seconds -clinical use limited by necessity of establishing a baseline response -transmission failure commences when 70% of receptors are occupied and is completed when 90% are occupied |
|
|
What is the train of four?
|
consists of 4 stimuli applied at 2 Hz - with increasing NDMB, the height of the twitch response decreases and each twitch has a smaller height than the one before it - each train repeated every 10 minutes *the availability of Ach is depleted with each successive stimulus* *no fade with sux, the height of twitches is just less* |
|
|
What percentage of receptors can still be blocked with full train of four?
|
70%
|
|
|
When is the third twitch of TOF abolished? the second twitch? The first twitch?
|
80-85% 85-90% 90-95% |
|
|
What is the goal for adequate surgical relaxation for abdominal surgery?
|
80% blockage or 1-2 twitches
|
|
|
What is the TOF ratio?
|
the last twitch divided by the first twitch -should be >0.9 at the end of surgery -must have 4 twitches to get a ratio |
|
|
What is double-burst stimulation?
|
two short trains - 3 stimuli each train at 50Hz -magnitude of the response is 3x greater than TO4 -the response to the 2nd burst is reduced |
|
|
What is tetanic stimulation?
|
consists of repetitive, high-frequency stim at frequencies of 50Hz or greater -usually applied for 5 seconds -more sensitive for residual blockade than single twitch *applying this stim changes the response of the NMJ to further stim for up to 30 minutes* |
|
|
What is post-tetanic facilitation and post-tetanic count?
|
Post-tetanic facilitation: 50 Hz tetanus applied for 5 seconds, 3 second pause, then stimulation at 1 Hz -number of twitches observed is inversely related to the degree of blockade and related to time until return of first response in TOF - 4/4 twitches = maybe about 5 minutes - 0/4 twitches = "it's gonna be awhile" |
|
|
Where do the electrodes get placed during NMB stimulation? How do they work?
|
there is a positive and negative electrode *the negative (black) electrode is placed distal - it generates its AP by depolarizing the membrane *the positive (red) electrode is placed more proximal - it hyperpolarizes the membrane |
|
|
There are several ways to evaluate NMB responses. What are they?
|
-visual assessment -tactile assessment -mechanomyography -electromyography -accelerography |
|
|
What nerve/muscle used to monitor NMB more closely reflects the blockade of larynx?
|
the ophthalmic branch of the facial nerve, monitors the contraction of the orbicularis oculi muscle -recovers early -causes contraction of the eyebrow |
|
|
What nerve/muscle used to monitor NMB recovers relatively late?
|
ulnar nerve - monitors contraction of the adductur pollicis -has increased sensitivity and slower time course |
|
|
Which nerve do you monitor to determine if your patient is ready for extubation?
|
the ulnar nerve
|
|
|
Which nerve do you monitor to determine if your patient is ready for intubation?
|
the facial nerve
|
|
|
What percentage of receptors are still blocked when tidal volume and vital capacity return to normal?
|
75% - TOF 4/4
|
|
|
What percentage of receptors can still be blocked when patient is able to head lift and has sustained hand-grip?
|
30%
|
|
|
List some things that potentiate neuromuscular blockade
|
volatile agents - local anesthetics - CCBs - beta blockers - aminoglycosides - magnesium - lithium - hypocalcemia - long term steroids - dantrolene - respiratory acidosis - metabolic alkalosis - hypothermia - hypokalemia - renal/liver dysfunction
|
|
|
What criteria is there to deep-extubate a patient?
|
-sustained tetany -TOF 4/4 -good tidal volume -regular respiratory rate |
|
|
What criteria is there to perform awake-extubation?
|
-the criteria needed for deep-extubation and... -nods yes/no -opens eyes -can lift head x5 seconds |
|
|
How does a pulse oximeter probe read the O2 saturateion?
|
1) two light-emitting diodes produce beams at red and infrared frequencies 2) there is a photo detector on the other side 3) the diodes flash about 30x/sec 4) the diodes are switched on in sequence with a pause where both ar off 5) the microprocessor analyzes the change in light absorption during arterial pulsatile flow and ignores non-pulsatile component of signal |