![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
121 Cards in this Set
- Front
- Back
|
1. Age related changes in pulmonary structure and physiology |
|
|
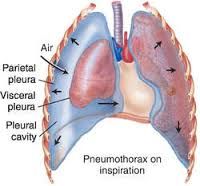
3. Pneumothorax: the presence of air or gas in the pleural space caused by: |
rupture in the
|
|
|
3. Primary (spontaneous) pneumothorax:
|
|
|
|
3. Clinical Manifestations of both Primary and Secondary Pneumothorax: |
|
|
|
3. Secondary (traumatic) pneumothorax Caused by: |
|
|
|
3. Iatrogenic pneumothorax is most commonly caused by: |
transthoracic needle aspiration |
|
|
3. Open (communicating) pneumothorax: Air pressure in the pleural space = barometric pressure b/c: |
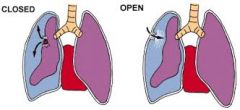
air drawn into pleural space during inspiration is forced back out during expiration |
|
|
3. Tension pneumothorax
|
|
|
|
4. Pulmonary edema |
Excess water in the lung from disturbances of capillary hydrostatic pressure, capillary oncotic pressure or capillary permeability. |
|
|
4. Most common cause of pulmonary Edema |
#1-Left side heart disease-Left ventricle fails ----->increase pulmonary capillary hydrostatic pressure. *ARDs (injury to endothelium)-->increased capillary permeability---->movement of fluid & plasma protein into alveoli/interstitial space. *Blockage of lymphatic vessels--->inability to remove fluid from interstitial space. |
|
|
4. Pulmonary Edema s/s |
dyspnea, orthopnea, hypoxemia, increased breathing work |
|
|
4. Acute respiratory distress system: |
Spectrum of acute lung inflammation and alveocapillary injury. Most survivors have almost normal lung function one year after acute illness but may have other health problems including neurocognitive disorders up to five years later. |
|
|
4. Acute respiratory distress system: Pathophysiology |
Alveoli capillary membrane producing massive pulmonary inflammation --->increases capillary permeability, severe pulmonary edema, surfactant inactivation, shunting, VQ mismatch, atelectasis and hypoxemia. ***Hallmark-Increased capillary permeability |
|
|
4. Acute respiratory distress system 3 phases 1st |
exudative-initial injury damages alveolar/capillary membrane-->inflammatory mediators--->cause damage--->increase capillary permeability-allow fluids, proteins and blood cells to leak into the alveoli--->pulmonary edema and loss of lung compliance |
|
|
4. Acute respiratory distress system 3 phases 2nd |
Proliferative-1-3 weeks after injury; edema resolution-->proliferation of pneumocysts, fibroblasts, and myofibroblasts. Intra-Aveolar hemorrhagic exudate--->cellular granulation tissue appearing as hyaline membranes--->progressive hypoxemia. |
|
|
4. Acute respiratory distress system 3 phases 3rd |
Fibrotic-2-3 weeks after injury. Remodeling and fibrosis occurs-obliterates the alveoli, respiratory bronchioles and interstitum ---->decreased functional residual capacity--->continuing VQ mismatch with sever R to L shunt--->acute respiratory failure. |
|
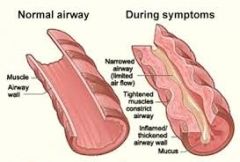
5a. Asthma |
Chronic inflammatory disorder of the bronchial mucosa that causes bronchial hyper-responsiveness, constriction of the airways, and variable airflow obstruction that is reversible.
|
|
|
5b. Athma- Etiology |
Familial disorder, more than 100 genes identified that may play a role in the susceptibility and pathogenesis
|
|
|
5c. Asthma- Patho |
Epithelial exposure to antigen initiates both an innate and an adaptive immune response in sensitized individuals. Many cells and cellular elements contribute to persistent inflammation of the bronchial mucosa and hyper responsiveness of the airways: (macrophages, T helper2 lymphocytes, B lymphocytes, mast cells, neutrophils, eosinophils, basophils) |
|
|
5d. Asthma - Clinical manifestations |
|
|
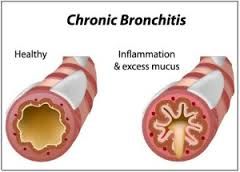
5e. Chronic bronchitis |
Etiology: hyper-secretion of mucus and chronic productive cough that continues for at least 3 months of the year for 2 consecutive years Pathophysiology: inspired irritants > airway inflammation with infiltration of neutrophils, macrophages, and lymphocytes into the bronchial wall. Continual bronchial inflammation > bronchial edema and increases the size and number of mucous glands and goblet cells in the airway epithelium. Thick mucous is produced and cannot be cleared because of impaired ciliary function. Clinical manifestations: decreased exercise tolerance, wheezing, SOB. Typically have productive cough and evidence of airway obstruction shown by spirometry |
|
|
5f. Emphysema |
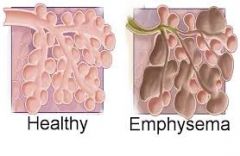
abnormal permanent enlargement of gas exchange airways accompanied by destruction of alveolar walls without obvious fibrosis |
|
|
5g. Emphysema - Etiology |
Primary emphysema :1-3% of all cases is commonly linked to an inherited deficiency of the enzyme a1-antitrypsin. Secondary emphysema: major cause is inhalation of cigarette smoke, although air pollution, occupational exposures and childhood respiratory tract infections are known to be contributing factors. |
|
|
5h. Emphysema - Patho |
destruction of alveoli through the breakdown of elastin within the septa by an imbalance between proteases and anti-proteases, oxidative stress, and apoptosis of lung structural cells. Alveolar destruction also produces large air spaces within the lung. Air trapping causes hyper-expansion of the chest, this puts the muscles of respiration at a mechanical disadvantage. Results in increased work of breathing, hypoventilation and hypercapnia (CO2 retention, excessive CO2 in the blood.) |
|
|
5i. Emphysema - Clinical Manifestations |
|
|
|
6.Pneumonia- |
Inflammatory reaction in the alveoli and interstitial. Most pathogens that enter the lungs are expelled or immune system destroys. Most important guardian of the lower respiratory tract is the alveolar macrophage- activating T-Cells and B-Cells. |
|
|
6.Pneumonia-Patho- |
*most common-aspiration of oropharyngeal sections in the lower respiratory tract. *inhalation of microorganisms from sneezing, talking *bacteria spreading from blood to lungs-bacteremia |
|
|
6.Pneumonia- Bacterial, atypical, viral |
Most common bacterial-streptococus PN; gram+ staph and streph, gram neg- Klebsiella Atypical-mycoplasma-small bacteria seen in summer and fall; school age children and young adults (dorms, colleges, barracks). Viral-RSV, influenza (little mucous) |
|
|
6.Pneumonia- S/S- |
S/S-increased tactile fremitus, dull percussion, decreased breath sounds, CXR-consolidation Bacterial-chills, fever, malaise, productive cough, purulent or blood tinged sputum Viral-cold symptoms-preceded by URI, fever, non-productive cough, hoarseness, wheezing, fine rales, |
|
|
6.Pneumonia- Risk factors Community Acquired bacterial PN |
Young, old Immunocompromised-(more likely to have opportunistic PN-fungal pneumocystic jerokeke-HIV, CA) Underlying lung disease ETOH Smoker |
|
|
6. Tuberculosis etiology risk factors tests |
Mycobacterium tb (acid fast aerobic bacilli) -infect lungs but may infect other organs. malnourished, immunosuppressed, living in crowded environments, incarcerated, elderly Mantoux (tb skin test)-best, doesn't differentiate active from latent. Blood tests interferon gamma release assays -Quantiferon-TB GOLD -T spot Sputum culture-takes 3 weeks-definitive CXR-Ghon tubercles- infiltrates in apex, lymph nodes |
|
|
6.Pathophysiology-TB |
droplet airborne (talk, sneeze, laugh) Lodges in the lungs---->mild puenocystics ----->bacilli migrate to lymph nodes----> T-cell mediated response-neutrophils & macrophages engulf and isolate bacilli. STOP the spread by trapping the bacilli in a granuloma called a ghon tubercle. It becomes dormant and will only show up with CXR or TB test. It may remain dormant for life or reactivation may occur d/t age, poor nutrition or reexposure which leads to active pulmonary disease. |
|
|
6. TB Clinical manifestations |
Latent TB-no s/s, can’t spread Active TB-infective and sick Bad cough-lasts 3 weeks or longer Pain in chest, coughing up blood or sputum Weakness, fatigue, anorexia, weight loss Chills, diurnal fever, night sweats |
|
|
6. Acute Bronchitis etiology Risk Factors Pathophysiology Clinical manifestations |
etiology-viral risk factors-Commonly follows a viral illness Pathophysiology-acute infection or inflammation of airways or brochi. Self limited-tx with diet, good nutrition, cough syrup, fliuds, and rest. Clinical manifestations-Nonproductive cough, occurs in paroxysms-cough, cough and cough and aggravated by cold, dry, dusty air. Mimics PN but no pulmonary consolidation. |
|
|
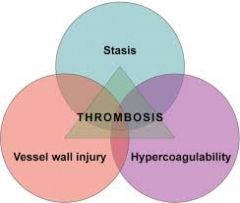
7a. Pulmonary embolism |
The occlusion of a portion of the pulmonary vascular bed by a thrombus, embolus, tissue fragment, lipids, or air bubble. Pulmonary emboli commonly arise (90%) from the deep veins in the thigh. |
|
|
7b. Virchow triad |
|
|
|
7c. Pulmonary Embolism - Clinical Manifestations |
In most cases the clinical manifestations are nonspecific. Depends on size of embolism: symptoms…. restlessness, apprehension, tachycardia, anxiety, dyspnea and then as it worsens=chest pain on inspiration and hemoptysis. |
|
|
7d. Pulmonary Embolism - Patho |
Depends on the size of extent of pulmonary blood flow obstruction, the size of the affected vessels, the nature of the emboli. Pulmonary emboli can result in the following: Embolus with infarction (emboli causes death of lung tissue); Embolus without infarction; Massive occlusion (embolus that occludes a major portion of the pulmonary circulation); Multiple pulmonary emboli (may be chronic or recurrent). The substance enters bloodstream or thrombus is dislodged by trauma, muscle action or changes in blood flow, amniotic embolism displaces blood in the vessel and causes immune response (release of neurohumoral substances such as serotonin, histamine, catecholamines, angiotensin II and inflammatory mediators such as endothelin, leukotrienes, thromboxanes, and toxic oxygen free radicals) that will lead to widespread vasoconstriction, shock, atelectasis, pulmonary edema and pulmonary htn, death. If the clot doesn’t cause infarction, the clot is dissolved by the fibrinolytic system and pulmonary function returns to normal. Risk of recurrent venous thromboembolism is 30% over the next 10 years. |
|
|
7e. COR PULMONALE |
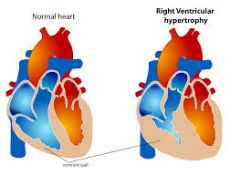
Secondary to Pulmonary Artery Hypertension and will cause signs of right sided heart failure > Right ventricular enlargement…because right ventricle has to work harder to pump blood into the lung. |
|
|
7f. COR PULMONALE - Patho |
Develops as pulmonary hypertension, creating chronic pressure overload in the right ventricle will cause a back flow into the periphery which causes edema. Acute hypoxemia can exaggerate pulmonary HTN and dilate the ventricle. Right ventricular filling pressures are normal until failure occurs. Right ventricle usually fails when pulmonary artery pressure equals systemic blood pressure. |
|
|
7g. COR PULMONALE - Clinical manifestations |
Heart appears normal at rest. With exercise: Decreased cardiac output, chest pain. Electrocardiogram shows right ventricular hypertrophy. |
|
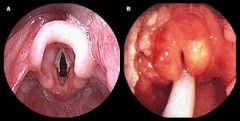
8a. Epiglottis - Etiology |
|
|
|
8b. Epiglottis - Patho |
|
|
|
8c. Epiglottis - Clinical Manifestations |
|
|
8d. Croup - Etiology |
Spasmodic croup - Sudden onset, usually at night, no viral prodrome, resolves quickly, occurs in older children, etiology is unknown and is thought to be associated with viral, allergy, asthma, and GERD. |
|
|
8e. Croup - Patho |
|
|
|
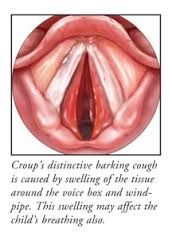
8f. Croup - Clinical Manifestations |
|
|

9. Tonsillar infections |
|
|
|
9. Bacterial tracheitis |
|
|
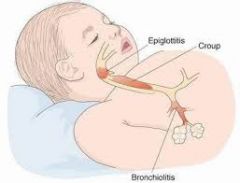
10a. Bronchiolitis -Etilogy |
A common viral-induced lower respiratory tract infection of the small airways in children younger than 2 years of age. Most common pathogen is Respiratory syncytial virus (RSV), but may also be associated with adenovirus, rhinovirus (older children) influenza, strep, pneumococci, and human metapneumovirus. |
|
|
10b. Bronchiolitis - Etilogy |
Peak incidence is during winter (late December) and a spike in February, and tapers off in spring. Major reason for hospital admission of children younger than one and children of lower socioeconomic status. Healthy children usually have a complete recovery. Although about 50% of children who have RSV bronchiolitis before age one will have asthma diagnosed by age 6 |
|
|
10c. Bronchiolitis - Pathophysiology |
|
|
|
10d. Bronchiolitis - Pathophysiology |
|
|
|
10e. Bronchiolitis - Pathophysiology |
|
|
|
10f. Bronchiolitis -Clinical Manifestations: |
|
|
|
10g. Bronchiolitis - Clinical Manifestations: |
|
|
|
10h. Bronchiolitis - Clinical Manifestations: |
|
|
|
10i. Bronchiolitis - Clinical Manifestations: |
|
|

11. SIDS *Etiology |
|
|
|
11a. SIDS *Theories on Etiology |
|
|
|
11b. SIDS *Risk Factors |
|
|
|
11c. SIDS *Risk Factors |
|
|
|
11e. SIDS *Prevention |
|
|
|
12a. Pt c/o of having a nagging cough that just won’t go away. Can’t remember when it started. Productive. Having a hard time exercising and gets SOB easily. |
Chronic Bronchitis |
|
|
12b. Mother comes in with infant who is 8 months old, states infant has come down with a nasal cold and cough, has had a fever for several days now, cough is “barky”, hoarse cry, difficulty sleeping. |
Croup |
|
|
12c. healthy male, 32 years old. Exhibiting tachypnea and difficulty breathing. C/O pain in right side, “inside my ribcage”. On auscultation of right side, lung sounds diminished in UQ and absent in LQ. |
primary (spontaneous) pneumothorax |
|
|
12d. 4 year old presenting with severe respiratory distress. Temp is 103.6, sore throat, not been drinking or eating, positive for strep. Stridor present on inspiration. |
epiglottis |
|
|
12e. Pt complaining of difficulty breathing, “chest feels tight”, audible wheezing, heart rate and respirations are elevated, accessory muscles being used on inspiration. |
asthma |
|
|
12f. Pt was a smoker for 15 years but quit 5 years ago. Pt has a slight non productive cough with dyspnea and elevated respirations. State they used to only have trouble breathing when walking or climbing stairs but now it feels like it won’t go away and that they are always having trouble. Pt states it helps slightly to lean forward and rest arms on their knees. |
Emphysema |
|
|
12g. 14 year old girl comes into ER after falling off her horse and landing on a rock. Left side of rib cage is bruised, absent lung sounds, pt is tachpnic, severe trouble with breathing and in pain. |
Secondary (traumatic) pneumothorax |
|
|
12h. Mother brings in 15-month old child, with a “bad cold”, runny nose and cough. Exhibits tachypnea, wheezing, Temp is 100.2, dyspnea, O2 sats 90%, rales auscultated. Mother states child is not eating well and is lethargic. |
Bronchiolitis |
|
|
12i. Pt with a history of DVT comes in with difficulty breathing and is highly anxious, also c/o of mild chest pain. HR and resps are elevated. |
pulmonary embolism |
|
|
13a. Pain
|
an unpleasant sensory and emotional experience with actual or potential tissue damage: • A symptom is not a clinical sign, diagnosis or disease • PAIN is always subjective • The inability for an individual to communicate verbally does not negate the possibility that they are experiencing pain and have a need for pain relief |
|

13b. Specificity Theory
|
• Amount of acute pain or specific injuries verses the amount of tissue injury (pin prick is less painful than a cut from a knife) • The activation of specific pain receptors and fibers that project to the brain • Doesn't explain chronic pain, cognitive or emotional elements that contribute to more complex types of pain |
|
|
13b. Specificity Theory
|
Increase: use of alcohol, pain killers, hypnosis, warmth, distraction, and faith. Decrease: repeated exposure to pain-killers |
|
|
13c. Patterning Theory
|
• Explains the role of impulse intensity and re-patterning of the central nervous system. • A limited theory, does not account for all pain experiences |
|
|
13c. Patterning Theory
|
|
|
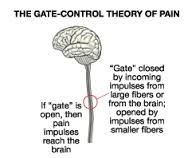
13d. (1) Gate Control Theory (GCT)-integrates builds upon features of other Theories of Pain
|
|
|
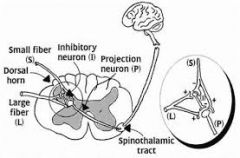
13d. (2) Gate Control Theory GCT
|
• Large myelenated A-delta fibers move the pain signals very rapidly and the brain perceives these signals as stinging and highly localized pain • Small, un-myelinated C fibers move impulses more slowly. Pain transmission is poorly localized dull and aching in nature. Within the internal organs. • Nociceptive transmissions on these fibers “open” the spinal gate and increase the perception of pain |
|
|
13d. (3) Gate Control Theory GCT
|
|
|
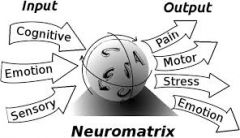
13e. (1) Neuromatrix Theory
|
• Grows out of the gate theory • the brain produces patterns of nerve impulses drawn from various inputs- genetic, psychological and cognitive experiences |
|
|
13e. (2) Neuromatrix Theory
|
|
|
|
13e. (3) Neuromatrix Theory
|
|
|
|
13e. (4) Neuromatrix Theory
|
the Gate Theory idea that the body-self provides a holistic, integrated, dynamic consideration of pain |
|
|
13f. No single theory
|
Adequately explains the complex dynamics of the many different types of pain or the pain experience
|
|
|
14.The three portions of the nervous system responsible for the sensation and perception of pain are: |
1. The afferent pathway begins in the PNS, travels to the spinal gate in the dorsal horn and then ascends to higher centers in the CNS. 2. Interpretive centers located in the brainstem, mid-brain, diencephalon, and cerebral cortex. 3. The efferent pathways that descend from the CNS to the dorsal horn of the spinal cord modulate pain. |
|
|
14.The processing of potentially harmful (noxious) stimuli through a normally functioning nervous system is called.... |
nociception |
|
|
14.Nociception involves four phases: |
transduction-stimulation of nociceptors transmission-fast-delta A fibers (skin & muscles); slow-C-fiber (internal organs) perception-pain awareness and interpretation modulation-suppression or facilitation of pain |
|
|
14.Pain transduction begins .... |
when tissue is damaged by exposure to chemical, mechanical, or thermal noxious stimuli and is converted to electrophysiological activity. This causes activation of nociceptors. |
|
|
14. Processing of pain 1st order neurons-nociceptors- |
bare nerve endings in the skin, joints, arteries and visera that respond to chemical, thermal, or mechanical stimulation. |
|
|
14. Processing of pain- 2nd order neurons |
Interneurons in the dorsal horn of the spinal column. They cross over and ascend. Excitatory or inhibitory-pain gate to regulate pain transmission |
|
|
14. Processing of pain- 3rd order neurons |
Afferent neurons in the spinothalamic tract. Carry info to the sensory cortex and reticular/limbic systems to process and interpret pain. |
|
|
14. Endogenous Opiate Peptides |
Decrease the perception of pain-like opioids-bind with opioid receptors. Enkephalins Endorphins Dynorphins Endorphins |
|
|
14. Dynorphins |
Most potent |
|
|
14. Beta Endorphins |
Reside in the hypothalamus and pituitary and are released during stress, pain, emotion, eating chocolate, laughter, massage or acupuncture. Reduce pain and produce sedation and euphoria. Strong mu receptors agonists that provide natural pain relief. |
|
|
14. Endorphins |
Potent analgesics GI and anti-inflammatory agents. |
|
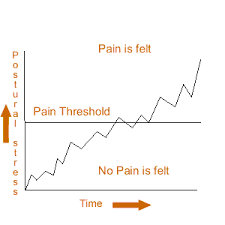
15. Pain Threshold |
The point at which a stimulus is viewed as painful. This point does not tend to vary over the lifetime or between people. |
|
|
15. What causes perceptual dominance? |
Perceptual dominance is caused when pain is so intense in one location, that it tends to mask pain in another location. |
|
|
15. What factors can influence an individual's pain tolerance? |
Pain tolerance is the amount of pain, or length of time a person will endure pain before engaging in overt pain responses. Influenced by: Culture, expectations, mental and physical health, roles, gender, fatigue, anger, boredom, apprehension, and sleep deprivation. |
|

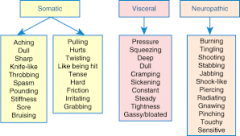
16. Somatic Pain |
|
|

16. Visceral Pain |
|
|
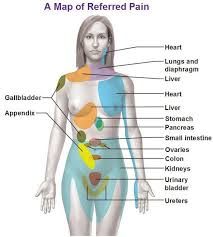
16. Referred Pain |
|
|

16. Neuropathic Pain |
|
|
|
16. Peripheral Neuropathic Pain |
|
|
|
16. Central neuropathic pain |
|
|
|
. |
|
|
2. paroxysmal nocturnal dyspnea |
pt wakes up gasping for air need to sit or stand Associate with CHF or undx obstructive sleep apnea. |
|
|
2. orthopnea |
lying down SOB |
|
|
2. dyspnea |
flaring of nostrils accessory use of muscles retractions |
|
|
2. cough |
acute 2-3 weeks chronic- > 3 weeks |
|
|
2. Kussmauls |
slightly increased ventilatory rate Very large tidal volumes No expiratory pause |
|
|
2. stridor |
high pitched sounds made during inspiration |
|
|
2. hyperventilation |
alveolar ventilation exceeds metabolic demands--->resp alkalosis from hypocapnia Blowing off CO2 Caused by anxiety, head injuries and increased RR. |
|
|
2. hypoventilation |
alveolar ventilation inadequate to meet metabolic demands--->resp acidosis from hypercapnia Caused by airway obstruction, chest wall restrictions, altered neurologic control of breathing |
|
|
2.central cyanosis |
Decreased arterial blood Caused by Pulmonary disease or pulmonary/cardiac right to left shunts Seen in lips of mucous membrane Poor indication of respiratory failure. Lack of cyanosis does not indicate normal 02 |
|
|
2.Peripheral cyanosis |
Vasoconstriction of periphery Seen in nails beds |
|
|
2.Clubbing |
Bulbous enlargement of the end of a digit -nailbed hypertrophy Associated with cystic fibrosis, *pulmonary fibrosis, congenital heart disease, *bronchiectasis Nonreversable Painless |
|
|
4. ARDs S/S (progressive) |
Dyspnea/hypoxemia-poor response to 02 supplementation----> Hyperventilation/Resp alkalosis---> Decreased tissue perfusion, metabolic acidosis and organ dysfxn-----> Hypercapnia, resp acidosis and worsening hypoxemia----> Decreased cardiac output, hypotension and death |
|
|
17.PediatricPain |
*PediatricPain Pathways-functional preterm and newborn infants *20-24 weeks gestations-nociceptors functional *Infants, crying, facial expression, body language, lack of consolability *5-18 years- lower pain threshold than adults |
|
|
17. S/S-infant Pain |
Brows-lowered, drawn together Forehead-bulge between brows, vertical furrowsEyes-closed tightly Cheeks-raised Nose-broadened, bulging Mouth-open, squarish |
|
|
17. Pain in Older Adults |
*Influenced by chronic disease *Pain threshold increases d/t peripheral neuropathies, skin thickens, cognitive changes *Pain tolerance decreases-women are more sensitive than men. *Alterations in the metabolism of drugs and metabolites occur d/t decreased renal/liver function |