![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
170 Cards in this Set
- Front
- Back
|
What is the basic structure of a local anaesthetic? |
Lipophilic group (aromatic ring) connected by an intermediate chain via an ester or amide to an ionizable group (i.e. A tertiary amine) |
|
|
What is the difference between ester links and amide links in local anaesthetics? |
Ester links are more prone to hydrolysis and and thus usually have a shorter duration of action. |
|
|
Are LAs acids or bases? |
Usually weak base Therefore in the body they usually exist as the charged cation - pKa.
The lower the pKa the greater percentage of uncharged species at a give pH. |
|
|
Which form of LAs bind the receptor site? |
Charged cation BUT it is the uncharged form that is able to enter the cell and bind the internal receptor site on the voltage gated sodium channel (alpha subunit) on the inside of the cell membrane (internal binding site) |
|
|
Why are LAs less effective in infected tissues? |
Due to lower extra cellular pH which favors the charged form and hence it cannot reach the internal binding site.
I.e. Adding bicarbonate can help potentiate the effect shortening time to onset. |
|
|
What is the function of pharmacokinetics in the use of LAs? |
Mainly functions to limit effect via metabolism and elimination
No need for activation etc |
|
|
Name common LAs and the duration of action. |
SHORT - procaine
MEDIUM - lidocaine, mepivacaine
LONG - tetracaine, bupivacaine, ropivacaine |
|
|
What factors affect systemic absorption of LAs? |
Dosage Site of injection Drug-tissue binding Local tissue blood flow Use of vasoconstrictor Drug properties - i.e. Lipophilic or protein binding increases duration of action |
|
|
What do the terms hyperbaric, isobaric, hypobaric refer to with regards to LAs? |
Refers to the movement of the LA relative to the CSF during a spinal anaesthetic
Hyperbaric - descend Isobaric - remain static Hypobaric - ascend |
|
|
What is the half life of bupivacaine, ropivacaine, lidocaine? |
Bupivacaine - 3.5 Ropivacaine - 4.2 Lidocaine - 1.6 |
|
|
Describe the distribution of LAs in the systemic blood. |
2 phases Initial alpha phase - rapid distribution in well perfused organs (brain, heart, kidneys, liver) characterized by a steep exponential decline in concentration Secondary beta phase - slower distribution to other organs, slower decline |
|
|
Metabolism and excretion of LAs? |
Amides - liver - P450 groups (hydroxylation and N-dealkylation)
Esters- plasma butyrylcholinesterases
Both are then excreted in the urine |
|
|
How can you increase urinary excretion of LAs? |
Excretion only occurs in the cationic form - not the neutral form.
Acidification of urine promotes ionization of the weak base (tertiary amine) - greater water solubility |
|
|
Mechanism of action of LAs? |
Bind the internal vestibule of voltage gated sodium channel and blocking activity
Binds alpha subunit Prevents depolarization, graded effect |
|
|
Which nerve block results in the highest peak blood level? |
Intercostal due to high surrounding blood flow |
|
|
Which nerve block results in the highest peak blood level? |
Intercostal due to high surrounding blood flow |
|
|
What are the physiological effects of local anaesthetic on the nerve? |
Block Na channel.
Increase threshold for excitation Impulse conduction slows Rate of AP rise declines AP amplitude declines Finally ability to generate an AP is abolished. |
|
|
What are the effects of Ca and K on LA effects? |
Calcium partially antagonises the effect via increasing surface membrane potential
Potassium extracellular - depolarizes the membrane and increases the effect of LAs |
|
|
Other effects of LAs? |
Blunting of the stress response Improvement in perioperative outcome with epidural anaesthesia Antithrombotic effect Modulation of inflammation |
|
|
What are the complications of LA administration? |
Allergy Cardiotoxicity - cardiac arrest , bradycardia, AV block CNS toxicity - metallic taste, tinnitus, nystagmus, perioral tingling, agitation, seizures SNS block- hypotension Respiratory depression and urinary retention with spinals |
|
|
What is the order of type (modality) of nerves blocked by LAs? |
SNS Temp Pain Light touch Motor block |
|
|
What effect do vasoconstrictors with LAs have? |
Neuronal uptake is enhanced due to increased concentration Reduced systemic level Longer duration of effect |
|
|
Treatment for LA toxicity? |
Intralipid If seizures - midazolam and intubation to prevent acidosis which will potentiate LA effects |
|
|
What are the mechanisms by which neurotoxicity occur with LAs? |
Conduction failure Membrane damage Enzyme leakage Cytoskeleton disruption Accumulation of intracellular calcium Disruption of atonal transport Growth cone collapse Apoptosis |
|
|
What is dantrolene used for ? |
Malignant hyperthermia due to anaesthesia
It is a spasmolytic with no central effects |
|
|
What is the origin of non depolarizing muscle relaxants ? |
South America curare poison arrows to kill animals |
|
|
What are the subunits that make up the nicotinic ACh receptor ? |
2 alpha Beta Gamma Delta
Binding receptor on alpha-beta and alpha -delta parts |
|
|
Besides non depolarizing and depolarizing - what drugs/ situations may have similar effects? |
Cholinesterase inhibitor intoxication
ACh high levels |
|
|
Neuromuscular blocking agents have limited CNS penetration. Why? |
Each have one or two quaternary nitrogens making them poorly lipid soluble which limits CNS penetration |
|
|
Reasons to use paralysis in ICU? |
Intubation Improve patient ventilator synchrony Enhance gas exchange Reduce barotrauma Reduce muscle 02 consumption Raised ICP facilitate treatment of tetanus etc |
|
|
What is the rate of homozygous defective pseudoholinesterase? |
1/3200
Paralysis for 3-8 hrs following a single dose |
|
|
Side effects of suxamethonium? |
Hypertension Tachycardia Bradycardia Ventricular arrhythmias Hyperkalaemia Raised ICP Malignant hyperthermia (within 1 hr)
|
|
|
Why do you not use suxamethonium in burns patients? |
Do not use in burns -- causes large K release which may cause cardiac arrest. |
|
|
What is dantrolene ? |
A spasmolytiC-- no central effects - treat malignant hyperthermia ryanodine receptor and prevents Ca2+ release via blocking the ryanodine1 R on the SR --> causes muscle weakness (skeletal muscle) Prevents contraction, lactic acidosis and high temps |
|
|
Describe the volume of distribution of non-depolarizing muscle relaxants. |
Small Vd - only slightly larger than plasma as they are highly ionised and do not readily cross cell membranes and are not strongly bound to peripheral tissues ? Due to quaternary amides |
|
|
Describe the half life of non depolarizing muscle relaxants. |
Depends on the method of elimination/excretion
Kidney - longer half life - pancuronium Liver metabolism - shorter i.e. Roc and vec
ATRACURIUM -- hepatic + HOFFMANN --> laudanosine (may cause seizures in accumulation)
--> liver (all steroid based) - although they may have active metabolites which may accumulate with prolonged administration -ICU) |
|
|
Describe the volume of distribution of non-depolarizing muscle relaxants. |
Small Vd - only slightly larger than plasma as they are highly ionised and do not readily cross cell membranes and are not strongly bound to peripheral tissues |
|
|
MOA, Metabolism and duration of action of sux? |
Short 5-10min Rapid hydrolysis by butyrylcholinesterase and pseudocholinesterase in the liver and plasma respectively
Blockade is terminated by diffusion away from the end plate
MOA - blockade of nAChr
Metabolized to succinylmonocholine is rapidly broken down to succinic acid and choline |
|
|
Test for assessing for variant of plasma cholinesterase? |
Dibucaine number
The abnormality causes prolonged muscle paralysis from sux |
|
|
Which muscle relaxant (non -depolarizing) has the fastest onset and shortest duration? |
Rocuronium |
|
|
MOA of sux? |
PHASE I - Binds nAChR - opens the channel - depolarisation - muscle contraction (fasiculations). Then flaccid paralysis as excitation - contraction coupling requires repriming and repetitive firing to maintain muscle tension - i.e. Non further depolarisations possible.
PHASE II - prolonged exposure - membrane is repolarised but desensitized - the receptors act like that are in a prolonged closed phase ---> possible reversal with cholesterase inhibitors at this stage (not earlier) |
|
|
Metabolism of roc? |
Liver mainly, some renal |
|
|
Metabolism of sux? |
Plasma cholinesterase |
|
|
Metabolism of cis? |
Mostly spontaneous via Hoffmann degradation
Action - 25-45 min |
|
|
How do you assess neurotransmission whilst under a NMJ blocking agent? |
Stimulator and recorder
Single twitch Train of four Tetanic stimulation Double burst and post tetanic count |
|
|
What is train of four ? |
Four muscle twitches in a dose reduced fashion. Ratio of the first and last muscle contractions.
With depolarizing agents there is fade inversely proportional to the blockade.
>0.7 for breathing >0.9 normal (no drug) |
|
|
What does the absence of fade on a double burst mean? |
There is no clinically significant neuromuscular blockade present |
|
|
Which muscle is last to be relaxed with paralysis? |
Diaphragm |
|
|
Side effects from nondepolarising NMJ blockers? |
CVS - atracurium - histamine - hypotension; pancuronium - tachy, increase CO; sux - negative CO/HR HYPERKALAEMIA - sux INCREASE INTRAOCULAR P - sux - not for OPEN globe injuries INCREASED INTRAGASTRIC P - sux - risk of aspiration - bad for delayed gastric emptying (DM), emergency cases, oesophageal dysfunction, morbid obesity MUSCLE PAIN - sux - myalgia |
|
|
What is the effect of anaesthetics on paralytics? |
Potentiate the effects
CNS depression Increased muscle blood flow - increased paralytic to muscle Decreased sensitivity of the post junction all membrane to depolarisation
Also potentiated by LA and aminoglycosides |
|
|
Conditions requiring extra /less paralysis |
Severe burns Upper motor neuron disease
Myasthenia graves and old age require dose reduction |
|
|
Name agents for reversal of neuromuscular blockade. |
Neostigmine Pyridostigmine Edrophonium Sugammadex (roc only) 1mg.kg |
|
|
Describe spasticity. |
Tonic stretch reflexes Flexor muscle spasms (increased basal tone) Muscle weakness Hyper excitability alpha motor neurons
Common with spinal injury, cerebral palsy, multiple sclerosis, stroke |
|
|
MOA benzodiazepines |
GABAa agonist |
|
|
MOA Baclofen |
Orally active GABA mimetic Agonist GABAb receptors --> increased k --> hyperpolarization --> pre synaptic inhibition by reducing Ca influx --> reducing the release of excitatory transmitters in the brain and spinal cord.
Can have withdrawal symptoms - seizures - needs slow cessation
|
|
|
Tizanidine MOA |
Alpha 2 agonist
Used for spasticity
Less cardio effects than clonidine |
|
|
What are the 5 characteristics of general anaesthesia? |
Unconsciousness Amnesia Inhibition of autonomic reflexes Skeletal muscle relaxation Analgesia |
|
|
Define local anaesthetic. |
Drugs which provide a loss of sensation in a region of a body
Is REVERSIBLE (vs etoh and tetrodotoxin) |
|
|
Nerve sensitivity to LAs |

Back (Definition)
|
|
|
Basic structure of LAs |

Intermediate = ester or amide |
|
|
Draw the buffer curve for a weak base. |
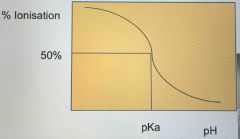
Weak acid is inverse of this Steep portion due to logarithmic scale of pH |
|
|
Factors that prolong the effects of LAs? |
Increased lipid solubility Increased protein binding
Injected into less vascular tissue Vasoconstrictor added |
|
|
Describe the pKa, protein binding and oil:gas partition coefficient.
What effect does this have? |
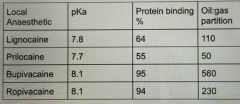
Lower pKa = faster onset
Increased protein binding and oil:gas coefficient = longer duration of action |
|
|
Effect of liver disease on LAs? |
Significant accumulation!! Toxicity
I.e. Lignocaine can increase t1/2 from 1.5 hrs to 6 hrs
I.e. Less frequent dosing |
|
|
Problems with LAs
Toxicity - local and systemic |
Local - intraneural injection (neuropraxia), direct pressure (due to large volume)
Spinal - TNS (transient neurological symptoms) - lignocaine, cauda equine syndrome, cardiac arrest (behold-jarisch reflex)
Systemic - CNS (perioral, tinnitus, muscle twitching, seizures, unconsciousness, apnoea, coma), cardiovascular collapse |
|
|
Problem with prilocaine? |
Significant metHb in adults with doses > 600mg
Beware - blue baby (cyanosis) with excess EMLA - contains prilocaine |
|
|
Recommended doses for common LAs |
Lignocaine 3mg/kg (7mg/kg with adrenalin)
Bupivacaine - 2mg/kg (Addition of adrenalin for alpha 2 effects)
Ropivacaine - 3mg/kg |
|
|
Which is less cardio toxic - ropivacaine or bupivacaine? |
Ropivacaine - provided as s isomer and less lipid soluble vs bupivacaine BUPIVACAINE IS Bad for the heart |
|
|
What is the classic arrhythmia with LA toxicity? |
Torsades de pointes |
|
|
Indication of muscle relaxants? |
Paralyse skeletal muscle with no effect on cardiac or smooth muscle Intubation (relax vocal cords, no gaging/coughing) Facilitate mechanical ventilation + major surgery |
|
|
Muscle relaxant adverse effects? |
Very dangerous, takes away the ability to breathe without an effect on consciousness (i.e. they are aware) Apnoea --> Death May also cause Anaphylaxis |
|
|
When do most cases of awareness occur when under a muscle relaxant without sufficient anaesthesia ? |
During prolonged induction, prolonged intubation attempts, Emergence/recovery (residual paralysis) |
|
|
Describe the physiology of the NMJ. |
ACh is synthesised in the nerve terminal by choline acetyl transferase from acetyl CoA and choline --> Depolarisation of the nerve --> Ca influx --> Fusion of vesicles with terminal via docking proteins --> ACh release --> ACh binds nAChR --> depolarisation of muscular endplate /muscle --> activation of voltage gated Na channels --> propagation of depolarisation --> Contraction (Can also have spontaneous vesicle release - MEPP) |
|
|
What do vesicles with ACh contain besides ACh? |
ATP Ca, Mg, H |
|
|
What is MEPP ? Function? |
Mini End Plate Potential - depolarisation due to ACh binding --> summate to cause depolarisation of the muscle and contraction Individual MEPP unable to cause depolarisation individually Possible function to main population of nAChR (lost with denervation) |
|
|
What can happen to ACh following release from the Nerve terminal? |
1. Hydrolysed by acetylcholinesterase 2. Bind post synaptic nAChR 3. Bind pre synaptic AChR (mobilise further ACh) 4. Diffuse away from NMJ to ECF/plasma |
|
|
Describe the nAChR. |
Pentamer Transmembrane Ligand -Gated Ion Channel (Cation pore - Na, Ca) 2x alpha, beta, delta, epsilon --> adult form ACh binds alpha units - requires 2 ACh molecules for activation Presynaptic and foetal forms have different subunit makeup |
|
|
Which answer is correct regarding the release of ACh at the motor endplate: A. Hemicholinium directly interfers with release B. Only in response to action potential C. Decreased by aminoglycosides D. Is a Ca dependent process E. Always causes an action potential |
A. Hemicholinium directly interfers with release (interfers with choline uptake) B. Only in response to action potential (spontaneous release) C. Decreased by aminoglycosides - CORRECT D. Is a Ca dependent process (spontaneous release) E. Always causes an action potential (MEPP) |
|
|
Why do you measure muscle relaxant effects? |
1. Onset - ? ideal for intubation? 2. Measure depth of paralysis - Adequate for surgery 3. Measure offset - ? require reversal |
|
|
How do you monitor Muscle relaxants? Modes? |
Peripheral nerve stimulator - 2 electrodes - Delivers electrical current - Monitor - visual, tactile, force transducer MODES - Single twitch, TOF, double burst (better for tactile monitoring), post tetanic count |
|
|
Difference between depolarising and non-depolarising muscle relaxants to TOF? |

Depolarising - no fade, TOF always 1 because no fade Non depolarising - fade |
|
|
When can reversal of non depolarising muscle relaxants able to be reversed? |
TOF count of 2 or more TOF Ratio > 0.9 = adequate reversal |
|
|
What is fade with muscle relaxants? |
ACh binds both post and presynaptic nAChR Presynaptic function - Mobilisation of vesicles via Ca influx and acts as a positive feedback loop to provide more ACh. Reduction in contraction due to >? reduced ACh - due to blockade of BOTH pre and post synaptic receptors |
|
|
What does Alpha-bungarotoxin do? |
It is a snake venom and blocks POST-synaptic nAChR Acts like non-depolarising muscle relaxant without FADE |
|
|
Post tetanic count Physiology? Clinical Relevance |
Tetanic stimulation mobilises/primes vesicles ready for release for subsequent APs. Greater quantities of ACh are released with APs/single twitches after a period of tetany --> then gradually declines to baseline levels. The extra ACh overcomes non depolarising competitive antagonists --> contraction (i.e. not with SUX) Count of 8-10 = TOF 1 |
|
|
Describe when different methods of measuring paralysis are useful. |
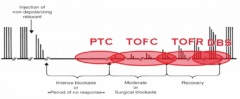
PTC and BD are better for tactile/visual monitoring |
|
|
Describe the receptor occupancy number for 1. a TOFC of 4 2. TOFR >0.9 3. ED95 |
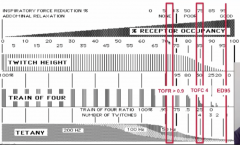
1. a TOFC of 4 - 75% 2. TOFR >0.9 - 85% 3. ED95 - >95% (twitch height reduction of 95%) |
|
|
Paralysis agent for RSI? |
Sux - short onset (<60sec) and offset (5-8 minutes) Can be given IMI - i.e. if a patient develops laryngospasm without IV access |
|
|
Dose of Sux? |
1-1.5mg/kg |
|
|
Onset of SUX? |
<60sec with fasciculations |
|
|
Duration of action of SUX? |
6-8 minutes No reversal (spontaneous) |
|
|
SUX MOA? |
Homologous to ACh (2 molecules) Binds nAChR - Opening of channel - MEPP - Summation --> Activation of resting Voltage gated Na channels --> opening of M + H gate (activated state) --> time dependent closing of H gate (inactivated state) --> change to resting state is dependent on re-polarisation which does not happen with suxamethonium present (remains depolarised) --> End plate block Sux - not metabolised by acetylcholinesterase |
|
|
What are the possible causes of a prolonged block by suxamethonium ? |
1. Abnormal SUX metabolism - plasma/pseudo/ butyryl cholinesterase (plasma protein, produced in the liver, high activity) - Genetics - Absence or reduction in enzyme - dibucaine test - Low in premies - Lower in pregnancy - Liver failure, malnutrition, disseminated malignancy, renal failure - Iatrogenic - plasma pheresis, Cardiopulmonary bypass - Drugs - anti cholinesterases - neostigmine, edrophonium; metoclopramide, cyclophosphamide, OCP 2. Phase II block with infusions or repeat dosing (2-4mg/kg) - similar to non-depolarising block |
|
|
Complications of prolonged paralysis i.e. due to pseudocholinesterase deficiency ? |
Reassurance for the patient who is paralysed and conscious Re-establish unconsciousness Maintain airway and ventilatory support until resolution --> ICU if prolonged Later --> Plasma cholinesterase activity assay, family testing, alert bracelet, avoid mivacurium |
|
|
Why check that sux has worn off before giving a non depolarising muscle relaxant? |
To ensure no prolonged paralysis by six to avoid confusion at the end of the case as to which has caused prolonged paralysis if it occurs |
|
|
What is the Dibucaine number of a normal person? a. 20 b. 40 c. 60 d. 80 e. 10 |
a. 20 b. 40 c. 60 d. 80 - Correct e. 10 |
|
|
Plasma Cholinesterase: A. Metabolises Dibucaine B. Metabolises Esmolol C. Hydrolyses Mirvacurium at 80% the rate of suxamethonium D. Is unaffected by neostigmine |
A. Metabolises Dibucaine (inhibited by dibucaine) B. Metabolises Esmolol C. Hydrolyses Mirvacurium at 80% the rate of suxamethonium - Correct D. Is unaffected by neostigmine |
|
|
Adverse effects of Sux ? |
Uncommon but serious: Anaphylaxis Malignant hyperthermia Bradycardia/Asystole Severe Hyperkalaemia/Cardiac arrest Prolonged paralysis Masseter muscle rigidity / spasm - difficult airway management Common but less serious: Myalgias (50%) Transient rises in IOP + ICP + intra-abdominal pressure Transient rise in K ~0.5mmol/L |
|
|
Conditions associated with severe/ life threatening hyperkalaemia with suxamethonium ? Cause> |
Upper or lower motor near defect, prolonged chemical denervation (paralysis, magnesium, botulism), direct trauma, burns (delayed - not with acute burn), disuse atrophy, severe infection Caused by the up regulation of metal nAChR which stay open for longer allowing greater K EFFLUX and are also able to be activated by Choline (six breakdown product) |
|
|
Is it safe to use SUX for intubation in patients with a head injury? |
YES Transient rise in ICP but still safe |
|
|
Other routes of administration for SUXAMETHONIUM? |
3-4mg/kg peripheral muscle --> 3-4minutes onset - Long 1mg/kg INTRALINGUALLY will cause apnoea and vocal cord relaxation in 75sec - Quick IE - use in a child without IV access who develops laryngospasm |
|
|
MOA of Rocuronium? |
Competitive antagonism nAChR Same as all non-depolarising paralytics |
|
|
How are Non-depolarising agents usually used? |
Post induction Given IV Dose is usually 2-3x ED95 Maintenance - smaller intermittent boluses or constant infusion |
|
|
What is ED50 and LD50? What is therapeutic index? |
ED50 - Effective dose 50 - dose at which 50% of subjects have the desired effect LD50 - Lethal dose 50 - dose to kill 50% of subjects Therapeutic index = LD50/ED50 |
|
|
What is EC95%? |
Dose required to produce 95% of the maximal response Graded measure |
|
|
How is potency of non-depolarising muscle relaxants measured? |
ED95 Median dose required to produced 95% twitch height reduction in 50% of subjects - Should actually be EC95 This is actually a graded response - i.e. EC95 ED95 is the ED50 for an EC95 response |
|
|
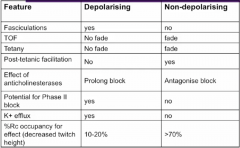
Describe the features for both depolarising and non-depolarising paralytic agents. fasiculations TOF tetany post tetanic facilitation effect of anti-cholinesterases potential for Phase II block K+ efflux % receptor occupancy for decreased twitch height |
|
|
|
Which non-depolarising paralytic has the shorted onset? |
Mivacurium - not really used in AUS ROC is the one we use Roc < atra |
|
|
Which Non-depolarising muscle relaxant is the least potent? |
roc i.e. need bigger doses for the same effect |
|
|
Metabolism of ROC? |
Biliary and renal prolonged duration with biliary obstruction |
|
|
Metabolism of Atracurium? |
Hoffmann degradation - spontaneous degradation also some hydrolysis by non-specific plasma esterase's Ie not end organ --> not dependent on liver or kidneys |
|
|
Which Non-depolarising muscle relaxant has 10 isomers? |
atracurium also associated with histamine release and may cause hypotension |
|
|
Difference between atracurium and cisatracurium? |
Cis - one isomer of atracurium Cis - less histamine, more potent, smaller doses, slower onset Metabolism - both - Hoffmann |
|
|
Breakdown product of Cisatracurium? Complications ? |
Laudanosine in accumulation associated with CNS excitation and seizures with prolonged administration |
|
|
Vecuronium - Elimination? - Reversal? |
Mainly biliary 40-60%; 20-30% renal Can be reversed with sugammadex |
|
|
Drugs that potentiate Non-depolarising muscle relaxant effects? |
Volatile anaesthetic Gentamicin, clindamycin Local anaesthetics Magnesium, CCBs |
|
|
Drugs that inhibit the effect of Non-depolarising muscle relaxants? |
Carbamazepine Calcium |
|
|
Complications of inadequate Non-depolarising muscle relaxant reversal? |
Distress / PTSD Respiratory - airway obstruction, hypoventilation, atelectasis |
|
|
What are the indicators of adequate reversal from Non-depolarising muscle relaxants? |
TOFR >0.9 Clinical (Unreliable) - sustained head lift >5sec, negative inspiratory pressure 40cmH2O, Vital capacity 20ml/kg |
|
|
Reversal of Sux? |
No reversal - short acting If prolonged action due cholinesterase deficiency --> FFP or whole blood as a source of plasma cholinesterase If in Phase II (no longer occurs) - normal reversal agents |
|
|
Agents for Reversal of Non-depolarising muscle relaxants? |
1. Increase endogenous agonist with ANTICHOLINESTERASES i.e. neostigmine 2. Bind and inactivate drug - SUGAMMADEX |
|
|
Problems with reversal of Non-depolarising muscle relaxants? |
Cant reverse deep block Need TOFC >2 Residual block not uncommon Anticholinesterases - block at both NMJ and PSNS nerve endings --> +++PSNS outflow at mAChR - therefore it is given with an anti-muscarinic agent - atropine or glycopyrrolate Anticholinesterases can cause paralysis - organophosphates and sarin gas |
|
|
Benefits of glycopyrrolate over atropine in combination with Non-depolarising muscle relaxant reversal with an anti cholinesterase? |
1. Onset similar to Neostigmine 2-3 minutes (atropine is faster and therefore SNS effects prominent) 2. Quanternary nitrogen group - polar - does not cross the BBB into the CNS (Atropine does cross) - central anticholinergic syndrome (elderly) - |
|
|
What is central anticholinergic syndrome? |
Syndrome produced by atropine crossing the BBB --> Causing confusion, drowsiness, delayed waking + other muscarinic side effects Rx - physostigmine (anti cholinesterase which crosses the BBB) |
|
|
Sugammadex function + uses? |
Irreversibly binds and inactivates rocuronium or vecuronium in the plasma Uses 1. Difficult airway - use large dose of roc for rapid onset and then if - can't intubate, cant ventilate - give sugammadex and rapid reversal in 90seconds 2. Reversal from deep paralysis for quick surgeries i.e. open/shut laparotomy or microlaryngoscopy 3. Therapy for Roc anaphylaxis |
|
|
Factors affecting the onset of paralysis ? |
Blood flow - i.e. cardiac output, IVC vs CVC, Highly perfused muscles From blood to NMJ --> Diffusion --> Ficks law of diffusion - Concentration/dose Receptor interaction - Sux only requires 15% of receptors bound to have effect, vs non-depolarising which require >70% for onset |
|
|
Describe the physical properties of the ideal anaesthetic. |
Physical Properties Stable in aqueous solution (don't need be mixed) Stable in light and at room temperature (can sit on the shelf) Stable in plastics No environmental impact Cheap, easy to produce Easy to administer Non-irritant to veins, arteries or tissues No pain on injection |
|
|
Describe the Chemical properties of the ideal anaesthetic. |
CHEMICAL PROPERTIES Rapid and smooth onset and offset Predictable onset No allergic reactions Rapid metabolism to inactive substances (Not dependent on end organ metabolism) No accumulation with repeated doses or infusion No drug interactions Minimal effects on body systems |
|
|
Name the common Intravenous agents for sedation or induction? |
Barbituates - Thiopentone Alkylphenols - Propofol Imidazoles - Etomidate (USA) Benzodiazepines - Midazolam Opioids - Fentanyl Other - Ketamine, droperidol, althesin |
|
|
Physiochemical properties of Thiopentone? |
THIOPENTONE Barbituate pKa7.5, pH 10.8 Produced as a salt - needs to be diluted Irritant to veins, arteries, tissues Some bacteriostatic properties |
|
|
Physiochemical properties of Propofol? |
PROPOFOL Alkylphenol pKa11, pH 6.0-8.5 Very lipid soluble 1% solution in soybean oil, glycerol, lecithin Solution promotes bacterial growth Pain on injection Non-irritant |
|
|
Physiochemical properties of Midazolam? |
pH 3.3 Water soluble 2 concentrations available - be careful! Non-painful, Non-irritant |
|
|
Physiochemical properties of Ketamine>? |
Phencyclidine derivative pKa 7.5, pH 3.5-5.5 Water soluble |
|
|
Describe the structure activity Relationships for BARBITURATES. |
Increase solubility- Sodium substitution at N3 › Increase hypnosis - At C5 substitute with an aryl or alkyl group, increase the number ofC atoms at R1/ R2 (at > 5-6 carbon atoms will decrease potency,increase convulsant activity) › Increase anticonvulsant effect- Phenyl substitution at C5, N1, N3 › Faster onset/ recovery – sulphonate C2, methyl substitution at N1 › Excitatory phenomena – methyl or ethyl substitution at N1 |
|
|
Describe the structure activity Relationships for benzodiazepines. (Ie chemical substitutions for clinical effect) |
Benzodiazepines Electronegative group at R7 essential for activity Increase activity – methyl group at R1, halogen group at R11 Decrease activity – larger group at R1, substitutions at R31 |
|
|
For Sedatives what does high lipid solubility allow for? |
High lipid solubility along with the large proportion of cardiac delivering blood to the brain allows for a rapid onset of action |
|
|
What is the effect of high protein binding on ONSET of sedatives? |
Bound drug cannot cross the blood-brain barrier, so whenprotein concentration is decreased, more drug is available Ie in hypoalbuminaemia --> increased drug available (requires dose reduction) |
|
|
What is redistribution half-life? |
Redistribution half-life – t1/2α – the time required for thecentral compartment concentration to decrease by 50%
|
|
|
Describe the pharmacokinetic properties of PROPOFOL. Onset, Lipid solubility, Vd, protein binding, metabolism |
Onset - 1-2min Highly lipid soluble, oil:water partition coefficient is 4700 Vd 200-400l (High) 98% protein-bound High hepatic extraction ratio (hepatic blood flow is moreimportant than the liver’s ability to extract propofol indetermining clearance) › Total clearance is greater than hepatic blood flow(significant extra-hepatic metabolism); 1400 – 2800 ml/min Hepatic Metabolism - Glucuronide and sulpha congugation + Renal metabolism |
|
|
Describe the Metabolism of Propofol. |
Hepatic metabolism - Glucuronide and sulpha congugation Renal metabolism (Up to 40%) >? pulmonary - low No active metabolites |
|
|
What is the half life of propofol? |
3 Compartment model T1/2 - alpha --> 2-8 minutes (removal from CNS - reflects clinical effects) T1/2 - beta --> 40 minutes (Secondary redistribution) T1/2 - terminal --> 300-700 minutes (Complete elimination - very long but no clinical effect on the pt) |
|
|
Pharmacodynamics of propofol on the CNS? |
Rapid acting hypnotic 1-3mg/kg for induction Decrease cerebral metabolism, decreases cerebral blood flow, decreases ICP due to vasocontriction Anticonvulsant effect Causes myoclonic movements Shortens therapeutic seizure in ECT Significant amnesia at sedative doses |
|
|
Pharmacodynamics of propofol on the Respiratory System? |
Decreases ventilatory drive, tidal volume and minute ventilation (dose dependent) Apnoea common Decreases airway responsiveness Decreases protective airway reflexes (risk of aspiration) Decreases airway resistance |
|
|
Pharmacodynamics of propofol on the CVS System? |
Decreases blood pressure by decreasing systemic vascular resistance and myocardial contractility Blunts the barostatic reflex May cause arrhythmias, sinus arrest |
|
|
Regarding Propofol which of the following is correct? 1. Causes PONV 2. Causes irritation with arterial injection or tissue extravasation 3. Causes hypertension on administration 4. Is metabolised by the liver only 5. Has intrinsic anti-emetic activity |
1. Causes PONV (No - helps prevent PONV) 2. Causes irritation with arterial injection or tissue extravasation (No) 3. Causes hypertension on administration (Hypotension) 4. Is metabolised by the liver only (Renal also) 5. Has intrinsic anti-emetic activity |
|
|
Which is correct regarding PROPOFOL? A. Pain free injection B. Triggers Histamine Release on injection C. Is a trigger for malignant hyperthemia D. Rarely causes anaphylaxis E. Can cause puritis F. Associated with Lactic acidosis following brief administration |
A. Pain free injection (Painful) B. Triggers Histamine Release on injection (No) C. Is a trigger for malignant hyperthemia (No) D. Rarely causes anaphylaxis E. Can cause puritis (Anti-puritic) F. Associated with Lactic acidosis following brief administration (Prolonged administration with high doses) |
|
|
Regarding Fospropofol vs propofol which of the following are incorrect (more than 1)? 1. Prodrug of propofol 2. Metabolised by the liver to propofol + phosphate +formaldehyde 3. Effects are due to metabolite - propofol 4. Faster onset than propofol 5. Also has painful administration 6. Sedation dose - 6.5mg/kg 7. Currently used in NSW |
1. Prodrug of propofol 2. Metabolised by the liver to propofol + phosphate + formaldehyde 3. Effects are due to metabolite - propofol 4. Faster onset than propofol - incorrect (3-4 minutes) 5. Also has painful administration - incorrect (Painless) 6. Sedation dose - 6.5mg/kg 7. Currently used in NSW - incorrect |
|
|
Regarding the pharmacokinetics of Thiopentone which of the following is INCORRECT (Multiple). 1. Highly lipid soluble 2. Oil:water coefficient = 5000 3. 20% protein bound 4. T1/2 alpha - 2-4minutes ; T1/2 beta 6-12hrs 5. Hepatic metabolism with inactive metabolites 6. Clearance 120-180ml/min 7. Vd - low ~ 10-20L |
THIOPENTONE 1. Highly lipid soluble - true 2. Oil:water coefficient = 5000 - incorrect (propofol ~5000, thiopentone 500) 3. 20% protein bound - incorrect (85% protein bound) 4. T1/2 alpha - 2-4minutes ; T1/2 beta 6-12hrs - true 5. Hepatic metabolism with inactive metabolites - incorrect (Pentobarbitone longer acting metabolite) - hangover effect 6. Clearance 120-180ml/min - true 7. Vd - low - incorrect (High - 100-200L) |
|
|
Regarding the pharmacodynamic effects of THIOPENTONE which of the following are correct/incorrect: 1. Rapid onset hypnotic - dose 4-7mg/kg 2. Decreases CMRO2/CBF/ICP 3. Neuroprotective - can have flat EEG 4. Anticonvulsant effect 5. Inhibitory effects on the respiratory system (reduced drive, Vt, MV + apnoea + reduced protective reflexes) 6. Decreases airway responsiveness |
THIOPENTONE 1. Rapid onset hypnotic - dose 4-7mg/kg 2. Decreases CMRO2/CBF/ICP 3. Neuroprotective - can have flat EEG 4. Anticonvulsant effect 5. Inhibitory effects on the respiratory system (reduced drive, Vt, MV + apnoea + reduced protective reflexes) 6. Decreases airway responsiveness - incorrect - increases - i.e. laryngospasm (propofol decreases) |
|
|
Regarding the pharmacodynamic effects of THIOPENTONE which of the following are correct/incorrect: 1. Causes Bradycardia 2. Causes hypotension 3. Causes PONV 4. Stimulate histamine 5. Anaphylaxis is common 6. Non-irritating to vessels/tissues 7. Decreased renal blood flow and increases ADH |
THIOPENTONE 1. Causes Bradycardia - incorrect (Tachycardia) 2. Causes hypotension 3. Causes PONV 4. Stimulate histamine 5. Anaphylaxis is common - incorrect (uncommon) 6. Non-irritating to vessels/tissues - incorrect (very irritating - may cause thrombophlebitis or thrombosis in arteries or tissue necrosis) 7. Decreased renal blood flow and increases ADH |
|
|
Which anaesthetic is contraindicated in PORPHYRIA ? |
Thiopentone / barbituates The barbiturates induce ALA synthase which catalyses theinitial step in haeme biosynthesis - ALA can accumulate because of the reduced enzyme activityand is neurotoxic |
|
|
What is the benefit of etomidate? |
Minimal CVS effects - i.e. no hypotension, cardiac depressive effects like propofol and thiopentone |
|
|
Which of the following are incorrect/correct regarding MIDAZOLAM pharmacokinetics: 1. T1/2 alpha - 7-15min 2. Cl 300-400ml/min 3. Vd 70-130L 4. High protein binding 94% 5. Highly lipid soluble due to unprotonated state 6. Metabolised via hydroxylation 7. High first pass metabolism - 15% oral bioavailability |
ALL CORRECT 1. T1/2 alpha - 7-15min 2. Cl 300-400ml/min 3. Vd 70-130L 4. High protein binding 94% 5. Highly lipid soluble due to unprotonated state6. Metabolised via hydroxylation 7. High first pass metabolism - 15% oral bioavailability |
|
|
Effects of midazolam - True/false: 1. Strong anxiolytic 2. Respiratory depression equally in all patients 3. Rapid onset hypnosis with large doses 4. Anticonvulsant effect 5. No drug synergy |
MIDAZOLAM 1. Strong anxiolytic 2. Respiratory depression equally in all patients - Incorrect (COPD greater depression) 3. Rapid onset hypnosis with large doses 4. Anticonvulsant effect 5. No drug synergy - incorrect (significant synergy with EtOH and opioids) |
|
|
Regarding the pharmacokinetics of KETAMINE which of the following are correct/incorrect: 1. Long T1/2 alpha - 11-17minutes 2. Cl 1250-1400ml/min 3. Vd 200-250L 4. High protein binding 90% 5. Metabolism - hepatic via N-demethylation to an inactive compound norketamine |
KETAMINE 1. Long T1/2 alpha - 11-17minutes 2. Cl 1250-1400ml/min 3. Vd 200-250L 4. High protein binding 90% - incorrect (low 12%) 5. Metabolism - hepatic via N-demethylation to an inactive compound norketamine - incorrect (true except norketamine is an ACTIVE compound) |
|
|
Effects of Ketamine on the CNS? |
Block NMDA - receptor Dissociated anaesthetic Profound analgesia Hallucinations Dysphoria Increases CMRO2/CBF/ICP |
|
|
IV dose of Ketamine? |
1-2mg/kg IMI 6-8mg/kg |
|
|
Benefits and negatives of Ketamine on CVS, resp, GIT... |
BENEFITS Bronchodilator Little respiratory depression Limited effects on airway reflexes Increases BP, HR, CO, SVR, contractility (may decrease if at maximal catecholaemine state) NEGATIVES Copious salivation (give with glycopyrrolate) Increase myocardial demand (AMI) PONV |
|
|
Effects of propofol, thiopentone, etomidate, benzos, ketamine on CMRO2, CBF, ICP, CPP? |
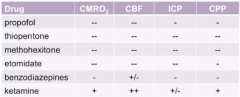
Mainly Ketamine increase |
|
|
Effects of propofol, thiopentone, etomidate, benzos, ketamine on the Cardiovascular System? |
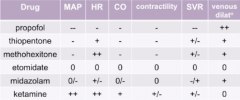
Ketamine only ++ |
|
|
Effects of propofol, thiopentone, etomidate, benzos, ketamine on the Respiratory System? |
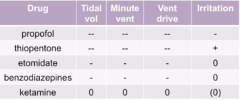
Ie if coughing after propofol ? aspiration because so depressant |
|
|
DOSE OF LIGNOCAINE, BUPIVACAINE, ROPIVACAINE |
Lignocaine 3mg - 7mg/kg with adrenalin Bupivacaine - 2mg/kg (cardiotoxic) Ropivacaine - 3mg/kg |
|
|
Which LA has the highest protein binding? |
Bupivacaine 95% ropivacaine 94% |
|
|
Potency order for paralytics for vec, cis, roc, pan, atracurium |
Vecuronium = pancuronium > cisatracurium = Atracurium > rocuronium |
|
|
Dose of sugammadex? |
1mg/kg |
|
|
What is the mechanism for the reduced incidence of hypotension with a single bolus dose of thiopentone compared with propofol? It is a direct positive inotrope Inhibition of the baroreceptor reflex is less pronounced It does not cause peripheral vasodilation Direct vasoconstrictor activity Less histamine release |
Inhibition of the baroreceptor reflex is less pronounced |
|
|
What are the respiratory side effects of propofol? Apnoea and reduced minute ventilation Bronchodilation and reduced bronchial secretions Reduction in upper airway reflexes with preservation of minute ventilation Respiratory stimulation and increased minute ventilation Bronchospasm and increased bronchial secretions |
Apnoea and reduced minute ventilation |
|
|
Apart from anxiolysis what is the other desired effect that makes midazolam useful in premedication for general anaesthesia? |
Anterograde Amnesia |
|
|
Ketamine is highly desirable as an anaesthetic drug. As well as its “dissociative anaesthetic” effect what other property is useful in the intraoperative management of patients? |
Analgesic properties |
|
|
What causes FADE? |
Non-depolarizing NMBDs block prejunctional receptors, resulting in failure of mobilization of ACh to keep pace with the demands of the stimulation frequency. Clinically, this is manifest as tetanic fade and TOF fade, in which there is a reduction in twitch height with successive stimuli. |