![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
146 Cards in this Set
- Front
- Back
|
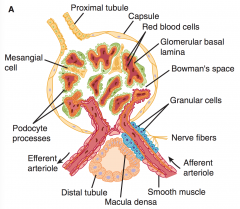
Which of the following are correct/incorrect regarding the Renal System? 1. Each human kidney contains ~1 million nephrons 2. Podocytes interdigitate and form filtration slits along the basement membrane. ~25nm wide 3. The basement membrane (basal lamina) has no gaps 4. Stellate cells (mesangial cells) are located between the basal lamina and endothelium - similar to pericytes 5. Mesangial cells are contractile and regulate glomerular filtration |
all correct |
|
|
Draw the basic glomerulus |
|
|
|
Which of the following are correct/incorrect regarding the Renal System? 1. Neutral substances <4nm usually pass through the BM without issue 2. The cells of the distal convoluted tubule have many microvilli and also had lateral intercellular spaces 3. The juxtaglomerular apparatus consists of the macula densa (top of TAL), lacis cells and renin secreting granular cells in the afferent arteriole 4. Collecting ducts empty into the renal pyramids 5. The collecting duct has Principal cells and Intercalate cells |
2. The cells of the distal convoluted tubule have many microvilli and also had lateral intercellular spaces - incorrect PROXIMAL CT 4. Collecting ducts empty into the renal pyramids - incorrect - into the renal pelvis at the apex of the medullary pyramids |
|
|
Name the components of the nephron in order: |
Glomerulus (cortex) Proximal convoluted tubule Loop of henle (medulla)- thin descending limb - thick ascending limb Distal convoluted tubule Collecting duct (into medulla) |
|
|
Difference between cortical and juxtamedullary nephrons? |
cortical - short loop juxtamedullary - at junction of cortex and medulla - long loop ~15% |
|
|
Function of P and I cells in the collecting duct |
PRINCIPAL CELLS - Theyare involved in Na+ reabsorption and vasopressin-stimulatedwater reabsorption. INTERCALATED cells - smaller numbers - They areconcerned with acid secretion and HCO3– transport |
|
|
PGE2 is secreted by what cells in the kidney? |
Renal medullary interstitial cells - RMICs Macula densa Collecting duct cells |
|
|
Blood supply to the nephron? |
Afferent arteriole from the interlobular arteries (from arcuate artery - from interlobar artery) Capillaries in the glomerulus Efferent arteriole Peritubular capillaries including vasa recta (around loops) drain into interlobular veins |
|
|
Which of the following are correct/incorrect regarding the Renal System? 1. At any one time the volume of blood in the renal capillaries is 30-40ml 2. The descending vasa recta are non fenestrated and have a transporter for urea 3. Lymphatic drainage is via the thoracic duct 4. Innervation of the kidney is via renal nerves along blood vessels containing SNS 5. The renal capsule limits swelling and raises renal interstitial pressure decreasing GFR |
4. Innervation of the kidney is via renal nerves along blood vessels containing SNS incorrect - only because it is incomplete SNS - lower thoracic and upper lumbar; cell bodies in sympathetic chain, superior mesenteric ganglia, along the renal artery PSNS via vagus |
|
|
Nocicepive signals travel via ? ... In the kidney |
Sympathetic nerves in the kidney |
|
|
What is the renorenal reflex? |
Increased ureteral pressure in one kidney leads to a decrease in efferent nerve activity to the contralateral kidney -- permitting increased excretion of Na and water |
|
|
Which of the following are correct/ incorrect? 1. Flow rate to the kidneys = 1.2-1.3L / min 2. % of CO to the kidneys = 25% 3. Glomerular pressure = 45mmHg 4. Noradrenaline constricts renal blood vessels - esp. Interlobar and afferent A. 5. Dopamine causes renal artery constriction and limits natriuresis |
5. Dopamine causes renal artery construction and limits natriuresis - incorrectCauses vasodilation and increases natriuresis |
|
|
Effect of noradrenaline, dopamine, angiotensin2, prostaglandins and ACh on renal blood flow?? |
Vasodilators - dopamine, ACh
Vasoconstrictors - noradrenaline, AT2 (aff/eff),
Prostaglandins - increase blood flow in the cortex and reduce it in the medulla |
|
|
Which of the following are incorrect: 1. The glomerulus functions to produce the filtrate ~ 7L/hr 2. Function of the PCT = Resorption of 65% of Na, K, Ca, Mg and H2O; 85% of NaHCO3 and 100% of glucose and AAs 3. Function of Thin descending limb of the loop = passive resorption of water via aquaporins 4. Function of TAL= Active Resorption of 15-25% Na, K, Cl + secondary reabsorption of Mg + Ca 5. Function of CCT = Na /K/H resorption |
Cortical collecting tubule 5. Function of CCT = Na /K/H resorption - incorrect Resorption of Na coupled to secretion of K and H |
|
|
Transporters located in the medullary collecting duct? |
Aquaporins
Drug target via ADH inhibitors |
|
|
Cortical collecting tubule - main targets for drugs ? |
Aldosterone receptor and effect on ENaC (spironolactone) ENaC (Amiloride) Aquaporins (Vartans) |
|
|
Permeability to water in the nephron is highest in the? |
Glomerulus > PCT = Proximal tube straight segments > TDL > TAL = DCT > CCT/MCD |
|
|
Main channel target in the TAL? |
Na/K/2Cl cotransporter |
|
|
Describe the primary active transport of H+ in the nephron. |
Primary active transport occurs in the distal tubule, cortical collecting tubule and ducts. It occurs in INTERCALATED Cells Active ATPase pump at the lumen |
|
|
Describe the secondary active transport of H+ in the nephron. |
PCT (mainly), TAL, early distal tubule Driven by the Na/K ATPase at the basolateral membrane. This creates a Na gradient --> allows transport via the H+/Na+ exchanger. This also allows for Bicarbonate reabsorption |
|
|
What are the 3 different mechanisms for pH buffering? |
1. Chemical buffers (bicarb, phosphate, proteins) - intracellular 2. Respiratory center - discard volatile acids - H2CO3 in the form of CO2 - 2 x as strong 3. Renal - slow but strong - Removal of non-volatile acids produced by protein metabolism |
|
|
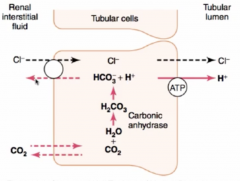
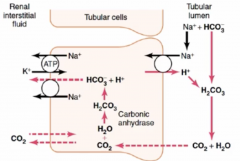
Locations of Bicarbonate reabsorption |
|
|
|
How is bicarbonate reabsorbed in the kidney ? |
Na/ HCO3 is cotransported in the proximal tubules HCO3 is exchanged in the late segments of the proximal tubule - TAL, CCT, CCD |
|
|
How much extra acid is secreted vs bicarb each day ? |
80meq of H+ this is due to the production of non-volatile acids generated by protein metabolism |
|
|
How does the kidney excrete enough H+ to balance the daily production of 80mEq of acid. |
1. Phosphate buffer in the tubules --> secretion of NaH2PO4 (limit 30-40mEq 2. NH3 buffer - 2 sections - more important - PCT - Glutamine breakdown to 2HCO3- (reabsorbed) & 2NH4+ (secreted and binds Cl) - CCT - NH3 ammonia (gas - moves freely) binds H+ = NH4+ (ammonium) in the lumen due to active H+ secretion from intercalated cells (and binds Cl) |
|
|
Describe the Ammonia buffer |

|
|
|
What is the importance of the ammonia buffer system in the nephron? |
Most important renal buffer 2 different processes Constitutes 50% of acid excreted (~40mEq) and 50% of bicarbonate generation in normal situations but can +++++ (500mEq/L) increase with chronic acidosis |
|
|
How do you calculate the net urinary acid excretion? |
NH4+ + titratable acid - HCO3- NH4+ is not a titratable acid due to the high pKa 9.2 and therefore H+ does NOT dissociate at pH of 7.4 Titratable acids are calculated by titrating urine pH to 7.4 by NaOH |
|
|
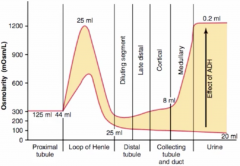
Describe the process of producing concentrated urine |
Mulitple steps 1. Development of concentration gradient in medullary interstitium via the loop of henle - counter current multiplier - active NaCl reabsorption 2. Water reabsorption in the cortex due to ADH - Aquaporins - cortical collecting tubules 3. Maintenance of the concentration gradient by the count current exchanger - the vasa recta - same shape as loop to prevent dissolution of gradient into the plasma 4. Role of passive Urea reabsorption ?? helps in maintaining the medullary concentration gradient |
|
|
What is the average concentration of urine Maximal concentration? |
Average - 600mOsm Max - 1200mOsm/L |
|
|
What factors are required for high urine concentration |
ADH High osmolarity of medullary interstitial fluid |
|
|
Describe the development of the medullary concentration gradient by the counter current multiplier. |

ESTABLISHING THE GRADIENT - complex process - best demonstrated with pictures but essentially urine 300mOsm is filtered - this reaches the TDL where H20 moves freely. Initially the interstitium is 300mOsm also to no movement. The urine then gets to the TAL where solutes are actively reabsorbed but not H2O movement. This increases the Concentration in the interstitium. More urine is pushed through which now at the TDL equibilates with the interstitium --> generating more concentrated urine (H2O leaves the lumen) --> this more concentrated urine reaches the TAL and more solute is excreted (diluting the urine) but also increasing the concentration in the interstitium. The end result is DILUTE urine but CONCENTRATED INTERSTITIUM |
|
|
Graphically demonstrate the difference in urine production with ADH vs no ADH at different stages throughout the nephron |
|
|
|
The hydrogen bonding between H2O moelcules allows for 3 key properties relevant to physiology - what are these? |
1. High surface tension 2. High heat of vapourisation 3. High dielectric constant (ie good conduction) |
|
|
Plasma as a % of total body weight? |
5% |
|
|
Interstitial fluid as a % of total body weight ? |
15% |
|
|
Extracellular fluid as a % of total body weight? |
20% |
|
|
Total body water as a % of total body weight ? |
60% |
|
|
Intracellular fluids as a % of total body weight ? |
40% |
|
|
Normal breakup of body fluids ? |
60% body weight = fluid of this -60 = 40% intracellular + 20% ECF ECF 20% = 15% interstitial + 5% plasma |
|
|
Normal physiological pH? Gastric fluid? Pancreatic secretions? |
7.35-7.45 -- slightly alkaline Gastric - 3.0 Pancreatic 8.0 |
|
|
The best buffers have a pKa of?? |
The same as the target pH ie 7.35-7.45 - physiological --> ie 50% ionised + 50% unionised therefore can buffer acidic or basic changes |
|
|
Describe Ficks law of diffusion. |
Fick law describes the movement of one molecule from a region of high concentration to low concentration. Net rate of diffuse - J Dependent on Concentration gradient/ chemical gradient = Concentration difference/thickness of boundary -- fraction; diffusion coefficient - D; area - A |
|
|
Define osmosis. |
Movement of a solvent into a region where there is a high concentration of solute to which the membrane is impermeable to. ie in the thin descending limb of the loop of henle |
|
|
What is the mOsm of 1 mmol of glucose, NaCl |
Glucose = 1mOsm NaCl = 2mOsm (dissociates into Na+ and Cl-) This is in an ideal/theoretical situation - although there is some interaction between the ions/incomplete disassociation -- therefore 154mmol of NaCl ie in a L bag of Normal saline does not produce 308mOsmol --> it is actually closer to 285 |
|
|
Define osmolality and osmolarity Differences? |
Theosmolarity is the number of osmoles per liter of solution (eg,plasma), whereas the osmolality is the number of osmoles perkilogram of solvent. Therefore, osmolarity is affected by thevolume of the various solutes in the solution and the temperature, while the osmolality is not. |
|
|
Units of osmolality in the human? |
mOsm/L of H2O |
|
|
What is the net effect of an infusion of 5% glucose? |
infusion of a hypotonic solution because the glucose is metabolised |
|
|
what proportion of the serum osmolality is made up by Na, Cl, HCO3? |
~270 of 290 plasma proteins make up very little of the plasma osmolality despite high g/L - due to high weight |
|
|
Location of Osmoreceptors |
anterior hypothalamus |
|
|
Location of synthesis of vasopressin? |
magnocellular neurons in the supraoptic and paraventricular nuclei of the hypothalamus and then transported via the neuronal axons to their nerve endings in the posterior lobe of the hypothalamus. |
|
|
Composition of Lymph? |
Normal Lymph flow is 2-4L/24hrs |
|
|
Function of lymph? |
1. Remove the excess fluid that is lost from capillaries and promote turnover of tissue fluid. 2. Movement of protein and other macromolecules from the ECF (esp protein from the liver and intestine) ~ 50% of circulating protein is returned to the blood by this method in one day 3. Movement of long chain fatty acids and cholesterol from the intestine via the lymphatics |
|
|
Types of Lymphatics ? |
1. Initial lymphatics --> drain into --> 2. Collecting lymphatics - contain valves and SM (contracts to propel the lymph) |
|
|
Causes for increased interstitial fluid and oedema? |
Increased filtration pressure/hydrostatic pressure - Post capillary venule constriction - Increased venous pressure - heart failure, incompetent valves, venous obstruction, increased total ECF, gravity Decreased osmotic gradient - Decreased plasma protein - cirrhosis, nephrotic syndrome - Accumulation of osmotically active substances in the interstitial space - inflammation Increased capillary permeability - inflammation, Substance P, histmine, kinins, cytokines Inadequate lymph flow |
|
|
Normal plasma osmolality range? Main mechanism for maintaining this? |
280-295 Vasopressin release or inhibition |
|
|
What type of receptors are Vasopressin receptors? Mechanism of signalling? |
G coupled receptors V1a + V1b = Phosphatidylinositol hydrolysis - IP3 to increase intracellular calcium V2 = Gs - Increase cAMP |
|
|
What is the physiological response to increased ECF osmolality? |
Increased thirst and Vasopressin release |
|
|
Effects of vasopressin? |
Vasopressin = ADH 1. V2 receptors - Increases permeability of the collecting duct to water via insertion of aquaporin 2 - concentrates the urine - water retention 2. Va1 - Vasoconstrictor effect - potent stimulator of vascular smooth muscle 3. Centrally reduces cardiac output 4. Va1 - glucogenolysis in the liver 5. Acts as a neuotransmitter 6. V1b - anterior pituitary to increase ACTH |
|
|
Factors that increase vasopressin secretion. |
Increased effective osmotic pressure of plasma (high osmolality) Decreased ECF volume Pain, emotion, stress N&V AT2 |
|
|
Factors that decrease vasopressin secretion. |
Vasopressin - increases H20 reabsorption - solute free 1. Decreases effective osmotic pressure of plasma (low osmolality) - osmoreceptors in the anterior hypothalamus 2. Increased ECF volume - stretch receptors - venous, arteries, atrial 3. Alcohol |
|
|
Vasopressin secretion occurs at what levels of osmolality>? |
285mOsm/L and upwards |
|
|
Pathway of signals from low pressure volume receptors to result in vasopressin release? |
Veins --> vagus nerve --> NTS nucleus tractus solitarius --> caudal ventrolateral medulla CVLM --> Hypothalamus (supraoptic and paraventricular nuclei) --> hypothalamohypophysial tract --> posterior pituitary |
|
|
Causes of vasopressin deficiency? |
30% neoplasms 30% post traumatic 30% idiopathic Remainder due to vascular lesions, infections, systemic diseases such as sarcoid |
|
|
Clinical syndrome produced by vasopressin insufficiency? |
Central diabetes insipidus polyuria polydipsia |
|
|
How come desmopressin can be used for central DI but not as a pressor like vasopressin? |
Desmopressin - dDAVP Has very high anti-diuretic activity with little pressor activity. Good for Rx of central DI |
|
|
What is the most important determinant of extracellular fluid volume? |
Na -- this to a great extent determines Cl (the other major solute) |
|
|
What are the physiological mechanisms to maintain ECF volume? |
1. Renin-Angiotensin II --> aldosterone and vasopressin release + Thirst + vasoconstrictor 4. Aldosterone - Na retention 3. High osmolality + Low volume = Vasopressin = H2O retention |
|
|
Which of the following are incorrect regarding the renin-angiotensin pathway? 1. ATII works at AT1, AT2 and AT3 receptors 2. Prorenin is converted to renin (active) in the kidneys only and is released from the granular cells in the juxtaglomerular apparatus 3.Renin half life 80minutes 4. ACE converts ATI --> ATII in the lungs; and also inactivates bradykinin 5. Renin is a protease that cleaves Angiotensinogen to angiotensin I |
1. ATII works at AT1, AT2 and AT3 receptors - incorrect - only 1 + 2 currently exist |
|
|
Location of synthesis of angioteninsogen? |
Liver |
|
|
Function of ACE? Main location of function? |
1. ATI --> ATII 2. Inactivation of bradykinin Mainly LUNGS - in endothelial cells |
|
|
Receptor causing the cough with ACEI? Frequency of cough side effect? |
B2 receptor - bradykinin Cough occurs in 20% |
|
|
Drugs that inhibit renin secretion? |
Indomethacin - inhibitors of prostaglandin synthesis propanolol pepstatin Renin inhibitors - enalkiren prevent ATI generation directly |
|
|
Half life of ATII |
1-2minutes |
|
|
Function of angiotensin II |
1. Arteriolar vasoconstriction --> increase BP - strong (except in Na deplete states due to high ATII and down regulation of receptors) 2. Aldosterone release - adrenal cortex 3. Facilitation of NA release 4. Contraction of mesangial cells and reduced GFR 5. Increased Na reabsorption 6. Vasopressin release + ACTH release |
|
|
Areas of the brain that ATII causes increase in polydipsia ? |
Subfornical organ - SFO OVLT part of the circumventricular organs |
|
|
Which of the following is incorrect? 1. ATIII has 40% of the pressor effect of ATII and 100% of the aldosterone effect 2. Micro renin-ATII systems help regulate local processes 3. AT1 receptors (chromosome 3) are associated with cavolae 4. AT2 receptors (chromosome X) are associated with phosphatases, activte K channel, increase NO and therefore cGMP 5. The Juxtaglomerular apparatus is made up of the macular densa and juxtaglomerular (granular) cells of the distal tubule |
5. The Juxtaglomerular apparatus is made up of the macular densa and juxtaglomerular (granular) cells of the distal tubule - incorrect Also has the non-granular cells - Lacis cells at the junction between the afferent and efferent arterioles |
|
|
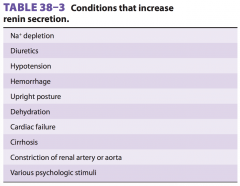
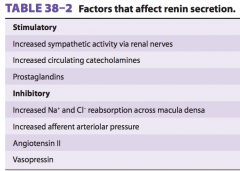
Factors that affect Renin secretion? |
1. Intra-renal baroreceptor mechanism - high pressure --> reduces renin secretion 2. Macula densa - Na load to distal tubule; High load = reduced renin 3. Stimulation from SNS, catecholamines, prostaglandins 4. Inhibition from ATII, Vasopressin |
|
|
Conditions associate with high renin levels |
|
|
|
Function of ANP? Atrial natriuretic peptide? |
Increase secretion due to NaCl intake or expanded ECF Cause natriuresis + vaso dilate Essentially reduce BP Released by atrial stretch |
|
|
BNP - brain natriuretic peptide / B-type NP is found in ? |
Brain and human ventricles |
|
|
Function of ANP and BNP? |
ANP and BNP in the circulation act on the kidneys to increaseNa+ excretion - dilating afferent arterioles andrelaxing mesangial cells = increased GFR - Inhibit Na reabsorption from the renal tubules - Vasodilators to reduce BP - ANP is found in neurons - opposite effect to ATII - reduce BP and cause natriuresis |
|
|
Effect of water immersion of ANP, ATII, Renin ? |
ANP - increase due to loss of gravity on blood and increased venous return ATII, aldosterone and renin - decreased |
|
|
How does EPO increase RBC production ? |
G protein linked
The receptor has tyrosine kinase activity, andit activates a cascade of serine and threonine kinases, resultingin inhibited apoptosis of red cells and their increased growthand development. takes 2-3 days to occur |
|
|
Source of EPO? |
85% - kidneys - interstitial cells 15% - liver |
|
|
Causes of EPO secretion? |
Hypoxia Cobalt salts, andogrens Alkalosis that occurs at high altitudes Catecholamines |
|
|
Erythropoietin is secreted by 1. cells in the macula densa. 2. cells in the proximal tubules. 3. cells in the distal tubules. 4 granular cells in the juxtaglomerular apparatus. 5. cells in the peritubular capillary bed. |
5. cells in the peritubular capillary bed. |
|
|
Dehydration increases the plasma concentration of all thefollowing hormones except A. vasopressin. B. angiotensinII. C. aldosterone. D. norepinephrine. E. atrial natriuretic peptide. |
E. atrialnatriureticpeptide. |
|
|
Renin is secreted by cells in the macula densa. cells in the proximal tubules. cells in the distal tubules. granular cells in the juxtaglomerular apparatus. cells in the peritubular capillary bed. |
granular cells in the juxtaglomerular apparatus. |
|
|
When a woman who has been on a low-sodium diet for 8days is given an intravenous injection of captopril, a drug thatinhibits angiotensin-converting enzyme, one would expect her blood pressure to rise because her cardiac output would fall. her blood pressure to rise because her peripheral resistance would fall. her blood pressure to fall because her cardiac output would fall. her blood pressure to fall because her peripheral resistance would fall. her plasma renin activity to fall because her circulating angiotensin I level would rise. |
her blood pressure to fall because her cardiac output would fall. |
|
|
Which of the following would not be expected to increase reninsecretion? Administration of a drug that blocks angiotensin-convertingenzyme Administration of a drug that blocks AT1 receptors Administration of a drug that blocks β-adrenergic receptors Constriction of the aorta between the celiac artery and the renal arteries Administration of a drug that reduces ECF volume |
Administration of a drug that blocks β-adrenergic receptors |
|
|
Which of the following is least likely to contribute to thebeneficial effects of angiotensin-converting enzyme inhibitorsin the treatment of congestive heart failure? A. Vasodilation B. Decreasedcardiacgrowth C. Decreased cardiac afterload D. Increased plasma renin activity E. Decreased plasma aldosterone |
D. Increased plasma renin activity |
|
|
% of nephrons with long loops of henle? |
15% |
|
|
Location of prostaglandin synthesis in the kidney? |
Mainly Renal medullary interstitial cells - RMICs Major site of COX2 and prostaglandin synthase Also EPO production here |
|
|
Swelling of a kidney is limited by? |
Renal capsule |
|
|
% of cardiac output to the kidneys? |
25% |
|
|
Substance used to measure renal plasma flow? |
PAH p-aminohippuric acid |
|
|
Glomerular capillary pressure ? Pressure in the peritubular capillaries? |
Glomerular - 45mmHg (40% of systemic) The drop between these occur in the efferent arterioles Peritubular - 8mmHg Renal vein 1-3 mmHg |
|
|
Effect of ATII on glomerular arterioles? |
Constrictor of afferent and efferent arterioles = reduce GFR = conservation of fluid |
|
|
What is the range for renal autoregulation of blood flow? |
90-220mmHg |
|
|
Region of the nephron most vunerable to ischemia? |
Medulla |
|
|
Define renal plasma clearance |
Renal plasma clearance is the volume of plasma fromwhich a substance is completely removed by the kidney ina given amount of time (usually minutes). |
|
|
The ideal substance to calculate GFR is Inulin. We use Creatinine as a non-invasive and fairly reliable parameter to calculate GFR. Why is the value calculated with Cr slightly higher than inulin? |
Cr also has a component of secretion in the tubules |
|
|
What is normal GFR? Normal volume filtered by the glomerulus each day? |
GFR 125ml/min Total filtrate produce - 180L/D --> >99% of this is reabsorbed |
|
|
Normal clearance of glucose, sodium, Creatinine, K>? |
Glucose - 0 - but with hyperglycaemia the GLUT2 is overwhelmed leading to glycosuria Sodium - 0.9ml/min K - 12 ml/min Creatinine 140ml/min |
|
|
What are the factors that govern GFR? |
Basic ultrafiltrate -- ie dependent on hydrostatic and osmotic pressures acting on the fluid. Also depends on the permeability of the membrane which may change with disease Surface area |
|
|
Charge of the sialoproteins in the glomerular capillary? |
Negative - hence negatively charged particles are repelled and need to be very small to pas through the membrane <4nm Vs 7nm for neutral particles |
|
|
Which is more easily filtered at the glomerulus? Positively charged molecules Neutral molecules Negatively charged molecules |
Positively charged molecules |
|
|
Normal amount of protein in the urine? |
100mg/d this is usually shed from the tubular cells rather than filtered |
|
|
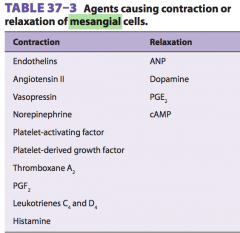
Name some factors that affect mesangial cells and what is the effect of this on GFR? |
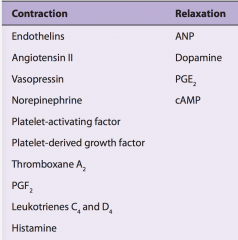
Contraction of mesangial cells reduces capillary lumen and reduces blood flow and hence GFR |
|
|
GLUT transport in muscle? |
GLUT 4 |
|
|
GLUT in neurons |
GLUT3 |
|
|
GLUT in liver and kidney? |
GLUT2 |
|
|
GLUT in Endothelium, BBB, RBC? |
GLUT 1 |
|
|
True/false. The pressure in the glomerular capillaries is higher than than in other capillary beds because the afferent arterioles are short,straight branches of the interlobular arteries and the efferent arterioles are relatively low resistance. |
FALSE All true except efferent capillaries are high resistance |
|
|
Is exchange in the glomerular capillaries flow or diffusion limited? |
FLOW ie - excess areas that are not forming filtrate -- increase flow will increase GFR |
|
|
What are the factors affecting GFR? |
SA Blood flow - systemic BP, afferent/efferent constriction/dilation Hydrostatic pressure - kidney swelling tamponaded by the capsule, blood flow/pressure, ureter obstruction Osmotic pressure - plasma proteins concentration Permeability |
|
|
T/f Clearance = GFR? |
It can be true IF there is no reabsorption or secretion of the substance in question but is usually FALSE |
|
|
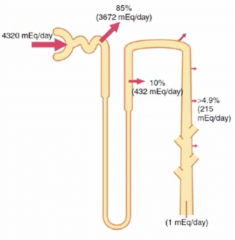
Which of the following are incorrect regarding renal physiology: 1. Na+ is actively reabsorbed in all parts of the tubules via Na/K ATPase pump 2. 60% of Na is reabsorbed in the proxmial tubule mainly via the Na/H exchanger 3. 30% of Na is reabsorbed in the TAL via the Na/K/2Cl cotransporter 4. 7% of Na is reabsorbed in the distal convoluted tubule via the Na/K cotransporter 5. 3% of Na is absorbed in the collecting ducts via ENaC |
1. Na+ is actively reabsorbed in all parts of the tubules. - Incorrect - not in the THIN part of the loop of henle 4. 7% of Na is reabsorbed in the distal convoluted tubule via the Na/K cotransporter -- Incorrect - Na/Cl cotransporter |
|
|
ENaC expression is regulated by ? |
Aldosterone |
|
|
The proximal tubule is involved in the reabsorption of? |
Na, K, Cl, Mg, Ca Glucose Bicarbonate Amino acids Water |
|
|
How is glucose reabsorbed from urine filtrate? |
PCT Apical - SGLT2 - sodium dependent glucose transporter (Na and glucose into the cell using the Na electrical and chemical gradient) - secondary active transport dependent on the Na/K ATPase Basal - Facilitated diffusion via GLUT2 |
|
|
What is tubuloglomerular feedback? |
As rates of flow increase through the TAL and DCT --> Glomerular filtration decreases (the reverse is also true) Sensor - Macula densa - senses the amount of fluid via the amount of Na/Cl present when taken up into the cells --> Increased Na ---> increased Na/K ATPase activity --> more ATP hydrolysis --> increased adenosine --> secreted --> A1 receptors --> macula densa --> increase release of Ca --> afferent arteriole vasoconstriction --> reduction in GFR and reduced RENIN |
|
|
How much urine would be produced with complete central diabetes insipidus? |
20.9L/day |
|
|
What is glomerulotubular feedback? |
Increased GFR = increased solutes to tubule = increased reabsorption of solutes and water so that solute reabsorption is generally held constant |
|
|
What occurs with water in the proximal tubule? |
Reabsorption so that the filtrate remains iso-osmotic. Reabsorption via aquaporin1 in both the apical and basal membranes |
|
|
Which part of the nephron is the diluting segment? |
TAL - solute reabsorption but impermeable to water (also the first part of the DCT - same functionality) thus -- dilution |
|
|
Where abouts in the nephron is ROMK located ? |
TAL |
|
|
Location of Aquaporin 2 |
Collecting duct insertion into the membrane is due to the presence of ADH/vasopressin via V2 receptors --> cAMP and PKA |
|
|
Protein involved in autosomal dominant polycystic kidney disease? |
PKD1+ PKD2 Ca receptor associated with a non specific ion channel - unclear function |
|
|
Channels associated with Batter syndrome? |
Any of the following -- TAL Na/K/2Cl cotransport, ROMK, ClC-Kb channel or barttin integral protein associated with deafness (except Cl-Kb mutation) Chronic Na loss - hypovolaemia without hypertension, hyperkalaemia, alkalosis |
|
|
channel effected in liddles syndrome? |
ENac - constitutively active HTN due Na retention Collecting duct |
|
|
ANP effect on Na reabsorption? |
increases cAMP which inhibits ENaC ---> natriuresis |
|
|
PGE2, IL1, endothelin effects on Na reabsorption? |
prevents reabsorption leading to natriuresis |
|
|
What rate of free water ingestion is required for water intoxication? |
>16ml/min for an extended period of time results in swelling of cells to hypo-osmolar changes in the plasma ---> swelling of neurons --> cell death --> convulsions - coma and death or at lower rates if exogenous vasopressin or oxytocin? is given |
|
|
General handling of K in the kidneys? |
Large reabsorption in the proximal tubules Secretion in the later tubule |
|
|
Symptoms of uraemia? |
lethargy, anorexia, nauseaand vomiting, mental deterioration and confusion, muscletwitching, convulsions, and coma. |
|
|
Pudendal nerves contain fibers from? |
S2/3/4 - control the external sphincter |
|
|
SNS + PSNS supply to the bladder? |
SNS - Hypogastric nerves - L1/2/3 - via inferior mesenteric ganglion PSNS - Pelvic nerves - S2/3/4 |
|
|
Function of the Detrusor? |
emptying the bladder during micturition |
|
|
In the presence of vasopressin, the greatest fraction of filteredwater is absorbed in the: proximal tubule. loop of Henle. distal tubule. cortical collecting duct. medullarycollectingduct. |
proximal tubule. |
|
|
In the absence of vasopressin, the greatest fraction of filteredwater is absorbed in the : proximal tubule. loop of Henle. distal tubule. cortical collecting duct. medullary collecting duct. |
proximal tubule |
|
|
If the clearance of a substance which is freely filtered is lessthan that of inulin, there is net reabsorption of the substance in the tubules. there is net secretion of the substance in the tubules. the substance is neither secreted nor reabsorbed in thetubules. the substance becomes bound to protein in the tubules. the substance is secreted in the proximal tubule to a greater degree than in the distal tubule. |
there is net reabsorption of the substance in the tubules. |
|
|
What is the clearance of a substance when its concentrationin the plasma is 10 mg/dL, its concentration in the urine is100 mg/ dL, and urine flow is 2 mL/min? 2 mL/min 10 mL/min 20 mL/min 200 mL/min Clearance cannot be determined from the information given. |
20 mL/min |
|
|
Agents that cause contraction and relaxation of mesangial cells? |
|
|
|
Factors that affect renin secretion - stimulation/inhibition? |
|