Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
47 Cards in this Set
- Front
- Back
|
hallucinegens/psychotomimetics- produce what effects (4)
|
produce delirium, true hallucinations (neurons being excited)), loss of contact with reality, death
|
|
|
psychotomimetics/hallucinegens- hollister's definition (4)
|
upon a single effective dose:
cause changes in thought, mood and perception with little memory impairment produce little stupor/narcosis or excessive stimulation (amphetamines) produce minimal autonomic side fx are non addicting |
|
|
why study these agents? (4)
|
hallucinegens as as tools for studying psych diseases (LSD for schizo)
basic neurochemical mechanisms in the brain NT functoin GPCR research |
|
|
classes of psychotomimetic agents (6)
|
LSD
phenylethylamine indole alkylamines (serotonergic) phenylcyclohexyl (PCP) N-methyl 3 piperidyl benzilate (Anticholinergic) canniboids |
|

|
LSD
|
|
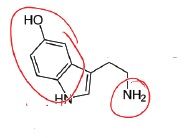
name the type of activity it has as well
|
indole alkylamine (serotonergic)
|
|
|
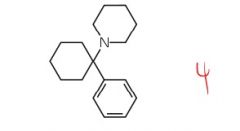
PCP (phenylcyclohexyl)
|
|

mimics what structure
|
phenylethylamine
(mimics DA/NE structure) |
|
|
classical hallucinogen properties (3)
|
meet hollister definition
bind to 5HT2 receptor recognized by DOM trained animals (behavioral) |
|
|
dissociative agent properties (3)
|
blocks or reduces signals to cortico/conscious mind
detachment from environment inhibits sensations from physical senses |
|
|
animal vs human studies for psycho agents (4)
|
human subjects should be best suited to provide most reliable assessment of actoins/potency of psychotomimetic agents- but...
case studies not that well controlled (limited pops, few drug doses, anecdotal) very few approved clinical studies in humans for psycho agents therefore we rely heavily on animal studies |
|
|
drug discrimination paradigm (testing method?) properties (3)
|
1) used for a variety of psychoactive agents
2) does not represent a model of psychomimetic activity 3) general applicability and is used to study stimulants, barbs, CNS agents, etc. |
|
|
describe drug discrimination paradigm general concept (2)
|
animals trained to discriminate the stimulus of a training drug (known MoA agent) vs vehicle (saline, DMSO, water)
then animals are taught to associate the effect of training drug with one specific lever, and one lever for vehicle |
|
|
DDP - describe how animals are trained (4)
|
2 levers in training boxes
lever A if saline will give animal food lever B will give food if animal is injected with LSD now you can test an unknown substance to see if it produces pharmacologically similar effects to training drug |
|
|
DDP- accuracy rate
dose dependency? |
trained animals respond 80% of the time or better to the appropriate drug
dose dependent- lower drugs = more mistakes, so can correlate # of mistakes to potency of drug via dose response curve |
|
|
DDP challenge drug
|
drug with unknown MoA- want to see if it gives similar stimulus effect
|
|
|
what is stimulus generalization?
|
important note: if similar stimulus effect to training drug is instigated we call it stimulus generalization. this does NOT mean they have the same MoA.
|
|
|
non-classical hallucinogens
|
canniboids
PCP |
|
|
3 common species of marijuana
|
cannabis sativa
cannabis indica cannabis ruderalis |
|
|
3 major presentations of pot- order in level of potency from highest to low
|
hashish- pure resin- most potent
ganja- flowering tops of plants- second most potent bhang- leaves and stems- least potent |
|
|
major active constituent of canniboid/pot
|
delta 9 THC
|
|
|
delta 8 THC
|
less potent version of delta 9 THC
|
|
|
major metabolite of THC
activity |
11 hydroxy delta 9 THC
retains some activity |
|
|
THC absorption (3)
|
most rapid through inhalation
absorbed through gut absorbed by body tissue then released slowly back into recirculation (hence why it lasts so long in your body) |
|
|
how long dose THC stay in body
|
D2O (deterium) labeled delta 9 THC has been detected even after 2 weeks in body after a single dose
|
|
|
THC tolerance and addiction
|
delta 9 THC dose develop but does not lead to physical dependence (addiction- as in you get withdrawals)
|
|
|
negative effects of MJ (4)
|
marijuana can impair memory, performance and learning- produces an amotivational sequence
|
|
|
CP55940
|
cannabinoid mimic made by pfizer- induces appetite but never marketed
|
|
|
win 55,212-2 - category of compound
activity |
not really cannabinoid. it is an aminoalkylindole that produces similar fx to THC
|
|
|
SR14617A - what's it do? (3)
|
inverse agonist at cannbinoid receptor (produces opposite effect)
attenuates TCH effect used for weight loss (appetite suppressed)- but if you stop taking it you gain all the weight back |
|
|
indole structure
|
know
|
|
|
AE of SR14617A (3)
|
depression
suicide if used in clinically silent MS pt resulted in sx manifestation that resulted from disruption of normal neuroprotective mechanisms |
|
|
MoA of cannibinoids (receptors affected) (2)
|
affects CB1 and 2 receptors
|
|
|
CB1 vs CB2
|
CB1 is found in brain
CB2 is found in periphery and believed to have immunomodulation effects |
|
|
endogenous cannibinoid (CB1) ligands (3) and potency relative to THC
|
anandamide- less potent
docosatetraenoylethanolamide- more potent homo-gamma-linolenylethanolamide (least potent) |
|
|
stability of endogenous CB1 ligands vs THC
|
not as stable? listen again
|
|
|
how is delta 9 THC metabolized?
potency |
OH on C11- more potent
|
|
|
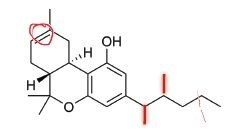
most potent THC derivatives (SAR)
|
delta 8 THC with 2 methyl groups on alklyl chain
|
|
|
delta 8 THC DMH (dimethyl) metabolism
|
hydroxyl group on C11 to 11 hydroxy delta 8 DMH
|
|
|
adding hydroxy group to THC- effect on potency
|
makes it more potent
|
|

what compound is this
potency? |
delta 8 thc metabolite
more potent (due to OH) |
|

compound? potency?
|
hydroxy dimethyl version of delta 8 THC
MOST potent |
|

compound?
potency? |
more potent
metabolite of delta 9 THC |
|

compound/potency
|
delta 9 THC
least potent |
|
potency
compound |
2nd most potent
delta 8 THC DMH |
|
|
non cns related disorders treated with weed (5)
|
alleviate IOP in glaucoma
spasticity in MS tourette's immune disorders (CB2 related) weight loss...maybe |
|
|
CNS related disorders that can be treated with weed (5)
|
neuropathic pain
parkinson's disease epilepsy drug abuse psych disorders |