![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
288 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Tx Mycobacterium tuberculosis. |
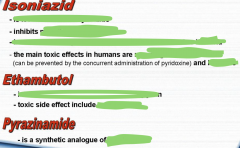
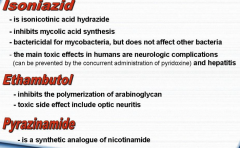
• Rifampicin. • Isoniazid. • Pyrazinamide. • Ethambutol. |
RIPE. |
|
|
Tx Mycobacterium leprae. |
• Dapsone. • Rifampin. • Clofazimine. |
Three agents. |
|
|
Tx Pseudomonas aeruginosa. |
• Pipercillin. • Fluoroquinolones and aminoglycosides. |
|
|
|
Tx Legionella. |
Fluoroquinolone. |
|
|
|
Tx Francisella tularensis. |
Streptomycin (aminoglycoside). |
|
|
|
Tx Bordetella pertussis. |
Macrolides. |
|
|
|
Tx Brucella. |
• Doxycycline. • Rifampin (adjunctive therapy). |
|
|
|
Tx Helicobacter pylori. |
• Clarithromycin (macrolide).
• Amoxicillin. • Proton Pump Inhibitor (PPI). |
|
|
|
Tx Yersinia. |
• Tetracycline. • Streptomycin. • Gentamicin. |
|
|
|
Tx Proteus. |
Sulfonamides. |
|
|
|
Tx Gardnerella vaginalis. |
• Metronidazole. • Clindamycin. |
|
|
|
Tx Pasteurella multocida. |
Penicillin V. |
|
|
|
Tx Bartonella henselae. |
• Azithromycin (macrolide). • Doxycycline for bacillary angiomatosis. |
|
|
|
Tx Neisseria meningitidis. |
• Ceftriaxone. • Rifampin (prophylaxis at close contact). |
|
|
|
Tx Neisseria gonorrhoeae. |
• Ceftriaxone. • Spectinomycin (for beta-lactamase producing gonococci and individuals with penicillin allergies). |
|
|
|
Tx Bacillus anthracis. |
• Fluoroquinolone. • Doxycycline. |
|
|
|
Tx Clostridium difficile. |
• Clindamycin. • Metronidazole. • Oral vancomycin. |
|
|
|
Tx Clostridium perfringens. |
• Penicillin G. • Clindamycin. |
|
|
|
Tx Listeria monocytogenes. |
Ampicillin. |
|
|
|
Tx Actinomyces israelii. |
Penicillin G. |
|
|
|
Tx Nocardia. |
Sulfonamides. |
|
|
|
Tx Chlamydia. |
• Doxycycline. • Ceftriaxone. • Macrolides. |
|
|
|
Tx Mycoplasma pneumoniae. |
Macrolides. |
|
|
|
Tx Rickettsia prowazekii. |
Doxycycline. |
|
|
|
Tx Rickettsia rickettsii. |
Doxycycline. |
|
|
|
Tx Borrelia burgdorferi. |
• Ceftriaxone. • Doxycycline. • Amoxicillin. |
|
|
|
Tx Staphylococcus aureus. |
• Vancomycin. • Nafcillin (MRSA). |
|
|
|
Tx Staphylococcus epidermidis. |
Vancomycin. |
|
|
|
Tx Staphylococcus saprophyticus. |
Vancomycin. |
|
|
|
Tx Streptococcus pyogenes. |
Penicillin. |
|
|
|
Tx Streptococcus agalactiae. |
Intra-partum penicillin. |
|
|
|
Tx Streptococcus pneumoniae. |
• Macrolides. • Ceftriaxone. |
|
|
|
Tx Streptococcus viridans. |
• Macrolides. • Ceftriaxone. |
|
|
|
Tx Enterococcus. |
• Linezolid. • Tigecycline. • Daptomycin. |
|
|
|
Tx Blastomycoses. |
• Amphotericin (disseminated inf.) • Itraconazole (local inf.) |
|
|
|
Tx Candida spp. |
• Amphotericin. • Itraconazole. |
|
|
|
HACEK organisms. |
• Haemophilus. • Aggregatibacter (Actinobacillus). • Cardiobacterium • Eikenella. • Kingella. |
|
|
|
Tx Coccidioides. |
• Amphotericin. • Itraconazole. |
|
|
|
Targeted therapy. |
Selection of a proper antimicrobial agent via demonstration of in vitro activity of several drugs against the infectious agent. Aka a "tailored" selection of drugs. The bacteria is cultured and tested with several antibiotics to see what it is susceptible to or not. |
|
|
|
Empirical therapy. |
• Choosing drugs based on the most likely causative microbe(s) and their sensitivity. • Site of infection. • Nosocomial or community-acquired. • Patient factors (age, weight, immune system condition). |
|
|
|
AST. Break abbreviation and define. |
Antimicrobial Susceptibility Testing, a measure of ability of an antimicrobial agent to inhibit bacterial growth in vitro. |
|
|
|
What is an inoculum? |
The number of bacteria in a suspension, calculated with respect to the final volume. |
|
|
|
Inoculum effect. |
A change in susceptibility related to change in inoculum size. |
|
|
|
MIC. Break abbreviation and define. |
Minimum Inhibitory Concentration. The lowest antibiotic concentration (mg/L) that inhibits the growth of a bacterial strain. |
|
|
|
MBC. Break abbreviation and define. |
Minimum Bactericidal Concentration. The lowest antibiotic concentration (mg/L) that kills a bacterial strain. |
|
|
|
What does MIC50 and MIC90 mean? |
The concentrations of antibiotic that inhibits 50% or 90% of the strains in collection. |
|
|
|
The gold standard for determining the susceptibility of organisms to antimicrobials. |
MIC. |
|
|
|
What are breakpoints? |
Defined concentrations (mg/L) of antibiotic which allow to classify bacterial strain to three categories: • Resistant. • Intermediate. • Susceptible. |
|
|
|
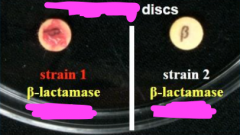
Qualitative AST. |
Diffusion method. Agar disc diffusion test. |
|
|
|
Quantitative AST. |
Dilution method. • Broth dilution. • Agar dilution. • E-test. |
|
|
|
Kirby-Bauer method. |
Standardized disc diffusion test. |
|
|
|
What is an antibiogram? |

|
|
|
|
Magic bullets. |
Selective toxicity. |
|
|
|
Antimicrobial drug. Define and give examples. |
A chemical that inhibits the growth or kills bacteria, regardless of its origin. • Antibiotics. • Semisynthetic and synthetic drugs. |
|
|
|
Chemotherapeutic drug. |
Any chemical used in the treatment, relief, prophylaxis or disease. |
|
|
|
Antimicrobial chemotherapy. |
The use of chemotherapeutic drugs to control infection. |
|
|
|
Intermediately susceptible bacteria may be killed by antibiotics under what conditions? |
• If the antibiotic is physiologically concentrated at the site of infection. • Higher than normal doses with low toxicity are given. |
|
|
|
Bacteriostatic action. |
Inhibitory. |
|
|
|
Bactericidal action. |
Killing. |
|
|
|
No antibiotic is effective against all bacteria (T/F). |
True. |
|
|
|

|
|
|
|
What does therapeutic index (TI) express, and how may it be expressed? |
Selective toxicity. Therapeutic dose / Toxic dose. |
|
|
|
The larger the therapeutic index, the better the antimicrobial (T/F). |
True. |
|
|
|
Examples of bactericidal antibiotics. |
• Penicillin. • Aminoglycosides. |
|
|
|
Examples of bacteriostatic antibiotics. |
• Tetracyclines. • Macrolides. |
|
|
|
What kind of antibiotics are preferred in immunocompromised pts. and in tx against serious systemic infections? |
Bactericidal antibiotics. |
|
|
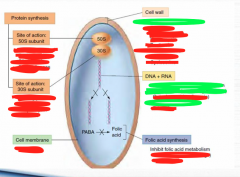
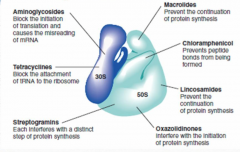
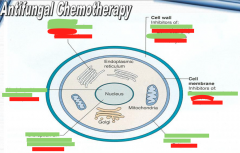
Greens are modes of action, and reds are antibiotics. |

|
|
|

In what mechanism of action order do the antibiotics follow?
|

|
|
|
|
Cell wall synthesis inhibitors only work on old, inactive cells (T/F). |
False. They are only active in young and growing cells, because old ones do not synthesize peptidoglycan. |
|
|
|
PRSP. |
Penicillin-Resistant Staphylococcus pneumoniae. |
|
|
|
MRS. |
Methicillin-Resistant Staphylococci = resistance to all beta-lactams. |
|
|
|
Beta-lactamases inactivate beta-lactams by hydrolyzing the beta-lactam ring out of the antibiotics (T/F). |
True. |
|
|
|
Aminopenicillins. |
• Amoxicillin. • Ampicillin. |
|
|
|
Carboxypenicillins. |
• Carbanecillin. • Ticarcillin. |
|
|
|
Ureidopenicillins. |
• Azlocillin. • Mezlocillin. • Piperacillin. |
|
|
|
Suicide inhibitors. |
Beta-lactamase inhibitors that become active when hydrolyzed by beta-lactamase. |
|
|
|
MRCNS. |
Methicillin-Resistant Coagulase Negative Staphylococci. |
|
|
|
VRE. How does this happen? |
Vancomycin Resistant Enterococci. Acquisition of vanA, vanB, D, E or G genes. |
|
|
|
VISA, VRSA. |
Vancomycin-Intermediate Staphylococcus Aureus Vancomycin Resistant Staphylococcus Aureus. |
|
|
|
ESBL. Break abbreviation and name the bacterias that produce this. |
Extended Spectrum Beta-Lactamases. • E. coli. • Klebsiella. • Proteus. |
|
|
|
Name some non-fermentative rods. |
• Pseudomonas.
• Stenotrophomonas. • Burkholderia. • Acinetobacter. |
|
|
|
Name some AmpC and carbapenemases. |
• P. aeruginosa. • Klebsiella. |
|
|
|
Among Enterobacteriaceae, what bacteria has natural resistance against aminopenicillins and carboxypenicillins? |
Klebsiella pneumoniae. |
|
|
|
Cephalosporins of higher generations have a higher ... spectrum. |
Gram-negative. |
|
|
|
Higher Gram-negative spectrum in cephalosporins means lowered potency (higher MIC) against Gram-positive bacteria (T/F). |
True. |
|
|
|
What bacteria are naturally resistant against cephalosporins? |
• Enterococci. • Listeria monocytogenes. |
|
|
|
What antimicrobial technique did Ignaz Semmelweis introduce? |
Handwashing. He discovered that childbed fever was carried on the hands of physicians who came directly from an autopsy to the delivery ward, without washing. |
|
|
|
What antimicrobial technique did Joseph Lister introduce? |
Phenol use as a surgical germicide. He was the first person to perform surgery under antiseptic conditions. |
|
|
|
What is a phenol coefficient? |
Quantitative comparison of a chemical's antimicrobic properties to those of phenol. |
|
|

|

|
|
|
|
What does aseptic mean? |
That an object or area is free of pathogens. |
|
|
|
What does aseptic technique mean? |
Use of specific methods to exclude contaminating microbes. |
|
|
|
What does antisepsis mean? |
Destruction of vegetative pathogens on living tissue. |
|
|
|
Define contaminants. |
Microbes present at a given place or time that are undesirable or unwanted. |
|
|
|
Name some examples of physical agents in decontamination methods. |
Heat or radiation.
|
|
|
|
Name some examples of chemical agents in decontamination methods. |
Disinfectants and antiseptics. |
|
|
|
Name one example of mechanical methods in decontamination methods. |
Filtration. |
|
|
|
What is the degree of antimicrobial control in sterilization? |
Removal of all microbial life. |
|
|
|
What is the degree of antimicrobial control in disinfection or antisepsis? |
Removal of pathogens (vegetative forms). Does not necessarily destroy all bacterial spores on inanimate objects. |
|
|
|
What is the degree of antimicrobial control in sanitization? |
Lower microbial counts to safe public health levels. |
|
|
|
What is the degree of antimicrobial control in preservation? |
Prevention of microbial growth in food or pharmaceuticals. |
|
|
|
What is sterilization? |
A process that results in the destruction or elimination of all forms of life, including bacterial spores and viruses on inanimate objects. |
|
|
|
What is disinfection? |
A process that results in the destruction or elimination of microbes but does not necessarily destroy all bacterial endospores on inanimate objects. |
|
|
|
What is antisepsis? |
A process that results in the destruction or elimination of vegetative microbes on exposed body surfaces, wounds and surgical incisions. |
|
|
|
What is degerming? |
Removal of microbes from a limited area, such as the skin around an injection site. |
|
|
|
What does the suffix -cide or -cidal indicate? |
A killing action.
|
|
|
|
What does the suffix -static or -stasis indicate? |
Inhibition of the microbial growth. |
|
|
|
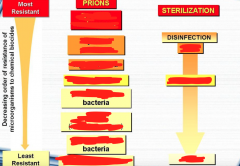
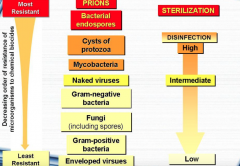
What is the most resistant microbial entity? |
Bacterial endospores. |
|
|
|
What kind of destruction is the goal of sterilization? |
Endospore destruction. Because any process that kills endospores will invariably kill all less resistant microbial forms. |
|
|
|
Any object that was undergone sterilization is considered to be what? |
Sterile. |
|
|
|
What entity that is not destroyed included in the term "sterile"? |
Prions, because they are not destroyed by standard sterilization procedures. |
|
|
|
What does SAL stand for, and what does it mean? |
Sterility Assurance Level; probability of a viable organism being present on a product unit after sterilization. |
|
|
|
In the EU, what is the SAL value, and does it mean? |
< 10^-6. Out of 10^6 items, a maximum of 1 item is it accepted as "sterile". |
|
|
|
What does PNSU stand for, and what does it mean? |
Probability of a Non-Sterile Unit; the probability of a unit being non-sterile after the sterilization process. |
|
|
|
What does the high level of disinfection include? |
Killing of all microorganisms, except for high levels of bacterial spores. |
|
|
|
What does the intermediate level of disinfection include? |
Killing of mycobacteria, most viruses and bacteria. |
|
|
|
What does the low level of disinfection include? |
Killing of vegetative bacteria and some viruses (lipid viruses), but not mycobacteria and nonlipid viruses. |
|
|
|
|
|
|
|
What gives Mycobacterium its' higher resistance to many chemicals? |
They have lipid mycolic acids in their cell wall. |
|
|
|
What is the least level of disinfection needed to get rid of Mycobacterium? |
Intermediate level. |
|
|
|
The bigger microbial population, the more... |
Time we need to kill it. |
|
|
|
During the death phase of a cell population, cells die at a constant rate (T/F). |
True. |
|
|
|
Define D value.
|
Decimal reduction time; the time required for killing 90 % of a population of bacteria under specific conditions. |
|
|
|
A bacterium is defined as dead if ...? |
It does not grow and reproduce when inoculated into culture medium that would normally support its' growth. |
|
|
|
What is the microbiological definition of death?
|
The permanent loss of reproductive capability even under optimum growth conditions. |
|
|
|
What does VBNC stand for, and what does it mean? |
Viable But Non-Culturable; bacteria that are still viable and show metabolic activity and respiration, but cannot be shown as CFU. |
|
|
|
VBNC are able to return to the infectious state after passaging animal hosts (T/F). |
True. |
|
|
|
Why is it important to clean items before disinfection or sterilization?
|
Because environmental factors such as • pH • Temperature • Presence of fats and other • Organic material such as blood and other body fluids can strongly influence microbial death rates. |
|
|
|
What is a critical item that may pose for infection? |
Items that come in direct contact with body tissues (e.g., needles, scalpels, forceps etc.). |
|
|
|
What is a semicritical item that may pose for infection? |
Items that come in contact with mucous membranes, but do not penetrate body tissue (e.g., GI endoscopes and endotracheal tubes). |
|
|
|
What is a non-critical item that may pose for infection? |
Items that only come in contact with unbroken skin (e.g., stethoscope). |
|
|
|

|
|
|
|
What is the practical technique in using moist heat as antimicrobial growth control? |
Boiling water or steam. |
|
|
|
What is the practical technique in using dry heat as antimicrobial growth control? |
Flame or electric heating coil. |
|
|
|
What does moist heat cause in pathogens? |
Coagulation and denaturation of proteins. This quickly and permanently halts cellular metabolism. It also degrades nucleic and disrupts cell membranes. |
|
|
|
Moist heat operates at lower temperatures and shorter exposure times to achieve the same effectiveness as dry heat (T/F). |
True. |
|
|
|
What is needed to inactivate prions? |
A combination of chemical and heat. Commonly 70% ethanol and formaldehyde vapor. |
|
|
|
In the presence of moisture, microorganisms are destroyed at a lower temperature than in dry heat (T/F). |
True. |
|
|
|
What cells are least resistant to both moist and dry heat? |
Vegetative cells of bacteria and fungi. |
|
|
|
For practical purposes, all non-heat-resistant forms of bacteria, fungi, protozoa, worms and viruses are destroyed by exposure to 80 Centrigrade for 5 minutes. |
False. It's for 20 minutes. |
|
|
|

|
|
|
|
What is pasteurization? |
Technique in which heat is applied to liquids to kill potential agents of infection and spoilage, while at the same time retaining the liquid's flavor and food value. |
|
|
|
What is the main goal of pasteurization? |
Prevent the transmission of milk-borne diseases from infected cows or milk handlers. |
|
|
|
What are the primary targets of pasteurization? |
Non-spore forming pathogens. • Salmonella. • Listeria. • Campylobacter. • Brucella. • Coxiella. • Mycobacterium bovis + tuberculosis. • and several enteric viruses. |
|
|
|
Pasteurization inactivate most viruses and destroy vegetative stages of 97-99% of bacteria and fungi, but do not kill endospores or thermoduric microbes (T/F). |
True. |
|
|
|
What is the batch method of pasteurization?
|
63-66 Centrigade for 30 minutes. |
|
|
|
What is the flash method/high-temperature short-term HTST pasteurization? |
71.6 Centigrade for 15 seconds followed by rapid cooling. |
|
|
|
Milk is sterile after pasteurization (T/F). |
False. It is not. That explains why opened milk will eventually spoil. |
|
|
|
What is the ultrahigh temperature UHT pasteurization? |
134 Centrigrade for 1-2 seconds. |
|
|
|
What is tyndallization? |
Fractional sterilization; triple pasteurization performed by 3 following days. |
|
|
|
What is an autoclave? |
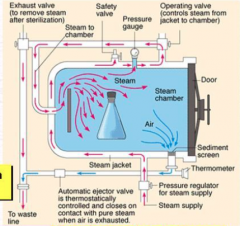
Steam-pressure sterilizer. |
|
|
|
Autoclaving is the preferred method of sterilization, unless the material to be sterilized can be damaged by heat or moisture (T/F). |
True. |
|
|
|
What bacteria is used to monitor sterilization?
|
Geobacillus stearothermophilus. |
|
|
|
Person-to-person transmission of prions causes what disease? |
Creutzfeldt-Jakob Disease. |
|
|
|

|
|
|
|
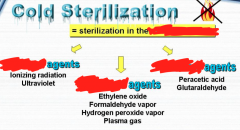
What happens during ionizing radiation (e.g., gamma rays, X rays) for sterilization? |
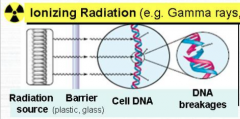
It breaks the chemical bonds in DNA. That may: • Inactivate enzymes. • Damage cell membrane. • Generate highly reactive free radicals. |
|
|
|
What happens during nonionizing radiation (e.g., UV) for sterilization?
|
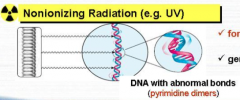
Formation of abnormal bonds within DNA (pyrimidine dimers). That may: • Generate highly reactive free radicals. |
|
|
|
What is the major target site for radiation sterilization? |
DNA. |
|
|
|
What is the most lethal type of UV radiation? What is its' action? |
UVC; 240-280 nm. May lead to cell mutations and/or cell death. |
|
|
|
What does UVA cause? |
315-400 nm; Changes in the skin that causes skin tanning. |
|
|
|
What does UVB cause? |
280-315 nm; Sun burning. |
|
|
|
UV radiation is usually directed at sterilization rather than disinfection (T/F). |
False. It is usually directed at disinfection rather than sterilization. |
|
|
|
The dosage of radiation is measured in ... |
Grays. 1 Gy is defined as absorption of the energy quantum 1 J/kg. |
|
|
|
Ionizing radiation is a highly effective alternative for sterilizing materials that are sensitive to ... |
Heat or chemicals.
|
|
|
|
How large of a dose is sufficient to disinfect with radiation? |
25 kGy. |
|
|
|
Name alkylating agents that are used in gaseous sterilization. |
• Ethylene oxide. • Formaldehyde. • β-propiolactone. • Methylbromide. • Propylene oxide. |
|
|
|
Name oxidizing agents that are used in gaseous sterilization. |
• Hydrogen peroxide. • Paracetic acid. • Chlorine dioxide. • Ozone. |
|
|
|
What does ethylene oxide sterilize? |
• Plastic materials and delicate instruments in hospitals and industries. • Prepackaged medical devices, surgical supplies, syringes and disposable petri plates. • Dressings and matrasses. |
|
|
|
What does ethylene oxide disinfect? |
Sugars, spices, dried foods and drugs. |
|
|
|
What is the difference between ethylene oxide and formaldehyde? |
Formaldehyde is used mainly as a surface sterilizing, because unlike EtO, it does not penetrate deeply. |
|
|
|
What is the mechanism of action of hydrogen peroxide vapor?
|
Local formation of hydroxyl radicals (-OH) that react with membrane lipids, DNA, and double bonds of essential cell components. |
|
|
|
Sterilization process of hydrogen peroxide vapor occurs at a temperature of ... in the concentration of ... |
• 35-49 Centigrade. • 10 mg/L. |
|
|
|
Gases, e.g, hydrogen peroxide, can be converted into the plasma form using a radiofrequency electromagnetic field (T/F). |
True. |
|
|
|
What are the two aldehydes used most often in microbial control? |
Glutaraldehyde and formaldehyde. |
|
|
|
Glutaraldehyde is employed in dental instruments to inactivate hepatitis B and other blood-borne viruses (T/F). |
True. |
|
|
|
Formalin tincture (8%) has a limited use as a ...
|
Disinfectant for surgical instruments. |
|
|
|
Filtration is an effective method to remove microbes from ... and ... |
Air and liquids. |
|
|
|
Air sterilization by filtration is made possible with what? |
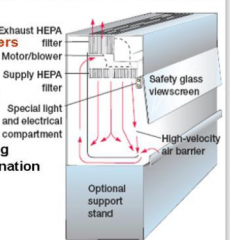
High-Efficiency Particulate Air (HEPA) filters. |
|
|
|
Disinfectants are ... applied only to ... |
• Antimicrobials. • Inanimate objects. |
|
|
|
Antiseptics are ... applied to ... and ... |
• Germicides. • Living tissue and skin. |
|
|
|
What are aqueous disinfectants/antiseptics? |
Disinfectant/antiseptic agents that are dissolved in pure water. |
|
|
|
What are tinctures? |
Disinfectants/antiseptics dissolved in pure alcohol or water/alcohol mixtures. |
|
|
|
In the properties of an ideal disinfectant, what agents currently in use come closest to fulfilling them? |
Glutaraldehyde and hydrogen peroxide. |
|
|
|
What are phenolics?
|
Phenol with one or more of its aromatic carbon rings attached to functional groups (Cl and CH3). |
|
|
|
Name the 4 most important phenolics. |
• Alkylated phenols (cresols). • Chlorinated phenols. • Bisphenols. • Triclosan. |
|
|
|
What bacteria have a natural resistance to triclosan, which strains have a decreased sensitivity to it? |
• M. tuberculosis and Pseudomonas are naturally resistant. • Desensitized strains include E. coli and S. aureus. |
|
|
|
During the production of triclosan, a highly carcinogenic and toxic compound is manufactured named ... |
Dioxin. |
|
|
|
Phenolics in high concentrations are ... |
Cellular poisons (rapidly disrupts cell walls and membranes and precipitates proteins). |
|
|
|
Phenolics are highly disinfectant, destroying most vegetative bacteria, fungi and viruses (except hepatitis B), but is not a reliable sporicide (T/F). |
True. |
|
|
|
What are the main characteristics of phenolics? |
• Stays on organic matter for a long time. • Detergent properties. • Disagreeable odor and can cause skin irritation. |
|
|
|
... is often used as an active ingredient in mouthwash. |
Chlorhexidine. |
|
|
|
What are the halogens? |
• Fluorine. • Bromine. • Chlorine. • Iodine. • Astatine. |
|
|
|
What's so special about the halogens? |
They are microbicidal and are sporicidal with longer exposure. |
|
|
|
What halogens are routinely used in germicidal preparations? |
Chlorine and iodine. Because fluorine and bromine are difficult and dangerous to handle. |
|
|
|
Chlorine combined with water releases what? |
Hypochlorous acid (HOCl). |
|
|
|
Phagocytes kill bacteria using what kind of halogen?
|
HOCl. |
|
|
|
What are the two primary preparations of iodine? |
• Free iodine (I2). • Iodophors. |
|
|
|
What are iodophors? |
Complexes of iodine and an organic carrier (a neutral polymer such as a polyvinylalcohol). |
|
|
|
What alcohols are suitable for microbial control? |
Ethyl and isopropyl alcohol. |
|
|
|
How is 70% alcohol better than 100% alcohol in terms of microbicidal activity? |
Water is needed for protein to coagulate. 100% alcohol would just dehydrate the cells and inhibit growth. |
|
|
|
Isopropyl alcohol (rubbing alcohol) must be used with caution in disinfection or skin cleansing, because ... |
Inhalation of its vapors can adversely affect the nervous system. |
|
|
|
Hydrogen peroxide is especially useful in treating infections by ... bacteria. Why? |
Anaerobic.
|
|
|
|
What are detergents? |
Polar molecules that act as surfactants. |
|
|
|
Cationic detergents are more effective than anionic ones (T/F). |
True. |
|
|
|
What are quats, and what are they used for? |
Quarternary ammonium disinfectant aka catonic detergents, used for low-level disinfection in the clinical setting. |
|
|
|
Only preparations containing ... and ... still have any significance as germicides. |
Mercury and silver. |
|
|
|
Ophthalmia neonatorum may be treated with what? |
Silver nitrate (AgNO3). |
|
|
|
Where does the acquirement of methicillin resistance come from? |
Acquisition of the mecA gene, encoding PBP2a.
|
|
|
|
Beta-lactamase inhibitors have no effect against MRSA (T/F). |
True. |
|
|
|
HA-MRSA. |
Hospital/Healthcare-Associated MRSA. |
|
|
|
CA-MRSA. |
Community-Acquired MRSA. |
|
|
|
Define homogenous MRSA. |
All cells in the population have the mecA gene, and they do show methicillin/oxacillin resistance. |
|
|
|
Define heterogenous resistance. |
All MRSA in a population have the mecA gene, but not all express methicillin/oxacillin resistance under in vitro conditions. |
|
|
|
What are the best methods for detecting MRSA? And what are the other, less costly ones? |
• PCR or DNA hybridization to detect the mecA gene. • Detect production of PBP2a by serologic tests. The routine clinical methods are as follows: • Disc diffusion. • Dilution tests (MIC). • Oxacillin agar screen test. |
|
|
|
PCR. |
Polymerase Chain Reaction. It is used to detect the mecA gene in MRSA cases. |
|
|
|
BORSA. |
Borderline Oxacillin Resistant Staphylococcus Aureus. They do not contain mecA, and may be treatable with beta-lactam/beta-lactamase combinations. |
|
|
|
BORSA may be due to what mechanisms? |
• Modifications in PBP 1,2 or 4 that do not bind to oxacillin efficiently. • Some strains are hyperproducers or beta-lactamase that partially inactivates oxacillin and other beta-lactams. |
|
|
|
MDR. |
Multidrug resistance. |
|
|
|
The drug of choice for pneumococcal infections. |
Penicillin. |
|
|
|
What are many PRSP also often resistant to? |
MDR strains.
• Macrolides. • Tetracyclines. •Trimethoprim/sulfamethoxazole. • Chloramphenicol. |
|
|
|
PNSP. |
Penicillin-Nonsusceptible Streptococcus pneumoniae. |
|
|
|
In a patient with S. pneumoniae induced meningitis, how should the susceptibility testing be done? |
MIC tests for penicillin and cefotaxime/ceftriaxone should be done. NOT oxacillin! |
|
|
|
In a patient with S. pneumoniae induced nonmeningeal infections, how should the susceptibility testing be done? |
Oxacillin disc screen test. |
|
|
|
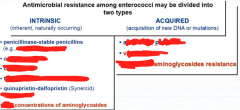
Define intrinsic resistance. |
Naturally occurring, chromosomally encoded resistance. |
|
|
|

|
|
|
|
Name three cell-wall active antibiotics. |
• Ampicillin. • Penicillin. • Vancomycin. |
|
|
|
What is the action of cell-wall active antibiotics? |
Bacteriostatic; inhibit, but do not kill. |
|
|
|
Treatment of Enterococci infections require a combination therapy of what? |
Cell-wall active antibiotics + aminoglycoside. |
|
|
|
Which Enterococcus strain is typically susceptible to ampillin/penicillin, and which one is resistant?
|
• E. faecalis is typically susceptible. • E. faecium are more often resistant. |
|
|
|
HLAR. |
High-Level Aminoglycoside Resistance. It is caused by the acquisition of aminoglycoside-modifying enzymes. |
|
|
|
AAD. |
Aminoglycoside adenyltransferase. It is a form of aminoglycoside-modifying enzyme. |
|
|
|
APH. |
Aminoglycoside phosphotransferase. It is a form of aminoglycoside-modifying enzyme. |
|
|
|
AAC. |
Aminoglycoside acetyltransferase.
It is a form of aminoglycoside-modifying enzyme. |
|
|
|
What is the usual aminoglycoside choice? |
Gentamicin. |
|
|
|
Intrinsic low-level resistance in enterococci is usually due to the presence of ... genes. |
vanC. Occurs exclusively in E. gallinarum and E. casseliflavus. |
|
|
|
Vancomycin has no activity against Gram-negative bacteria (T/F). |
True. |
|
|
|
Vancomycin is very gentle and easy to administer, and is usually used on the most common infections (T/F).
|
False. It is very toxic and hard to administer, and is restricted to only the most serious, life-threatening infections. |
|
|
|
VRE becomes a clinical disaster if that includes the bacteria being a MRSA as well (T/F). |
True. |
|
|
|
MRSE. |
Methicillin-Resistant Staphylococcus epidermidis. |
|
|
|
The most common type of VRE. What kind of bacteria does it include, and what is its' characteristics. |
VanA. • E. faecium. • Strains are highly resistant to vancomycin and teicoplanin. |
|
|
|
The second most common type of VRE. |
VanB. • E. faecalis. • Strains are highly resistant to vancomycin, but susceptible to teicoplanin. |
|
|
|
VDE. Characteristic? |
Vancomycin-Dependent Enterococci. It only grows in the presence of vancomycin in agar. |
|
|
|
VSSA. |
Vancomycin Susceptible Staphylococcus Aureus. |
|
|
|
GISA. |
Glycopeptide-Intermediate Staphylococcus Aureus. |
|
|
|
GRSA. |
Glycopeptide Resistant Staphylococcus Aureus. |
|
|
|
What may be the cause of VISA? |
Thickened cell wall (increased production in PBP2a). |
|
|
|
How many VRSA strains have been detected so far (2002-2009)? What kind of strains are they? What kind of gene cluster do they have? |
• 11 VRSA. • MRSA strains. • VanA gene cluster. |
|
|
|
What may be a successful treatment against patients infected with VRSA/MRSA? |
• Combinations of vancomycin and beta-lactams.
e.g., vancomycin + oxacillin. |
|
|
|
Define MLS(B) and its' mode of action. |
Multiple mechanism of resistance to 3 different groups of antibiotics. • Macrolides. • Lincosamides. • Streptgramins B. Inhibits protein synthesis by binding to the 50S ribosomal subunit (23S rRNA). |
|
|
|
What is MLSB resistance mediated by? |
Erythromycin resistance methylase (erm genes). |
|
|

|

|
|
|
|
What kind of beta-lactams can beta-lactamases inactivate? |
• Penicillinases. • Cephalosporinases. • Carbapenemases. |
|
|

|

|
|
|

|

|
|
|
|
Define inducible beta-lactamases. |
Bacteria that only produce beta-lactamases in the presence of a beta-lactam antibiotic. Poses a diagnostic problem. |
|
|
|
Define constitutive beta-lactamases. |
Bacteria that continually produce beta-lactamases. |
|
|
|
MRCNS. |
Methicillin Resistant Coagulase Negative Staphylococci. |
|
|
|
PPNG. |
Penicillinase Producing Neisseria Gonorrhoeae. Plasmid-mediated beta-lactamase production. |
|
|
|
CMRNG. |
Chromosomally Mediated Resistant Neisseria Gonorrhoeae. Altered PBPs. |
|
|
|
H. influenzae with TEM-1 and ROB-1 has resistance to what? |
Amoxicillin and ampicillin. |
|
|
|
BLNAR. |
Beta-lactamase negative, ampicillin resistant. |
|
|
|
M. catarrhalis with beta-lactamases BRO-1 or BRO-2 has resistance to what? |
• Ampicillin. • Amoxicillin. • Penicillin. |
|
|
|
Tx M. catarrhalis. |
Amoxicillin-clavulanic acid (Augmentin). Others: • Trimethoprim-sulfamethoxazole. • Oral cephalosporins. • Macrolides. • Tetracyclines. • Fluoroquinolones. |
|
|
|

|
|
|
|
ESBL-mediated resistance is not always obvious to all cephalosporins in vitro, thus the disc diffusion test is unreliable in detecting ESBL (T/F). |
True. |
|
|
|
Define AmpC beta-lactamases. What bacteria produces it?
|
• Chromosomal inducible cephalosporinases. • Enterobactericeae. • P. aeruginosa. |
|
|
|
AmpC beta-lactamases are inhibited by beta-lactamase inhibitors (T/F).
|
False. They are not inhibited. |
|
|

|

|
|
|

|

|
|
|
|
Beta-lactams mode of action. |
Irreversibly block the biosynthesis of peptidoglycan. |
|
|

|
|
|
|
|
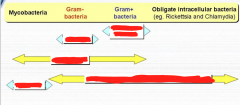
Aminoglycosides are ineffective against obligate intracellular bacteria (Rickettsia and Chlamydia), because they are not actively transported into cells (T/F). |
True. |
|
|
|
What aminoglycoside can be adminstered to help control P. aeruginosa infections that occur in patients with cystic fibrosis? |
Tobramycin. |
|
|
|
... is a bactericidal cyclic polypeptide which inhibits cell wall synthesis, and is mainly active against Gram-positive bacteria. |
Bacitracin. |
|
|
|
... is a bacteriostatic agent that inhibits protein synthesis by forming a stable complex with elongation factor EF-G. It is active against Gram-positive cocci. |
Fusidic acid. |
|
|
|
... are commonly used as alternatives to beta-lactam antibiotics for treating a variety of infections. |
Fluoroquinolones. |
|
|

|

|
|
|
|
TMP/SMX. |
Trimethoprim-Sulfamethoxazole. |
|
|
|
Name a sulfonamide. |
Sulfamethoxazole. |
|
|

|

|
|
|
|
Name a nitroimidazole. |
Metronidazole. |
|
|

|

|
|
|
|
|
|
|
|
XDR-TB. |
Extensively Drug Resistant Tuberculosis. MDR-TB strains that are also resistant to three or more of the six classes of second line drugs. |
|
|
|
MDR-TB. |
Multidrug Resistant Tuberculosis. Strains that are resistant to at least the two main first-line TB drugs (rifampin and isoniazid). |
|
|
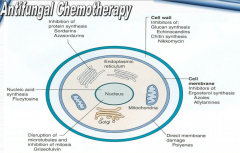
Greens are modes of action, and reds are the antimicrobics. |
|
|
|
|
Polyenes mode of action.
|
Cell membrane disruption by binding with ergosterol. |
|
|

|

|
|