![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
50 Cards in this Set
- Front
- Back
|
Campylobacter |
Most common in Aus nationally. Most common human pathogens: - C. jejuni - C coli They are gram -ve and Zoonotic (acquired from raw meats, milks and untreated water). Also comes from infected pets and farm animals. seen in children and also 20-29 yo (backpacker's diarrhoea). Clin Mani: presents 2-5 days after incubation with rapid onset fever, cramping abdo pain first and then diarrhoea onset lagging behind (24-48 hrs). First secretory diahrrohea and then bloody (inflammatory) diarrhoea which can persist for weeks. Constitutional symptoms are the rule andinclude, malaise, myalgia, headache, backache, andarthralgias. Among rare complications, strong associationwith Guillain - Barre syndrome (persist for weeks afterdiarrhoea) Complications and rare but these 2 are indicative of this species: - reactive arthritis - Guillain-Barre syndrome Diag: - stool sample for culturing on agar (campy selective agar) - stool antigen testing Treatment - self-limiting (so supportive) - if worsening then azithromycin and ciprofloxacin. |
|
|
Vibrio Vibrio cholerae O1 V. cholerae O139 Bengal |
Gram -ve, shaped rods. Causes secretory diarrhoea. The 2 serotypes are: - vibrio cholerae O1(the classic one from history) - Vibrio cholerae 0139 bengal (the strain that came up later in asian countries) - there are some others. It is nationally notifiable. From faecal-contaminated water and seafood harbouring. Vibrio found in syria, refugee camps, tropical. Clin Mani: after 24-48 hrs of ingestions of bacteria: - rice water diarrhoea - abdominal cramps - nausea - vomiting - low grade fever Median duration of disease is 7 days. Vibrio parahaemolyticus - watery diarrhoea Diag: - stool or rectal swab that need to be transported specially. Special agar is "thiosulfate citrate bile salts sucrose agar", lives in salt water converts sucrose to yellow colour which is seen. - serotyping Treat - for classic cholera oral or IV fluds - azithromycin or ciprofloxacin orally if severe - other treatments for the Aus types |
|
|
Clostridium |
G +ve bacillus, found normally in colon. The one that over grows when Abx are given or 3-4 wks after discontinuation. The problem is the pseudomembranous colitis. At risk: - >65 - underlying illness - antiulcer (lowering the acid) - hospital stay. It is a spore forming organism and so can survive all kinds of surfaces. CLin mani - cramping abdo - profuse watery secretory diarrhoea some with blood - smell is distinctinve Complications: pseudomembranous colitis. Diag - culture and toxin detection - stool toxin detection assays: PCR and EIA methods Treatment - resolution usually within 48 to 72 hours after Abx therapy - if not solved or severe: metronidazole, vancomycin, and usually resolves within 36-72 hours. - if no resolve and severe then surgical referral. |
|
|
Listeria monocytogenes |
G +ve facultative anaerobe rods and is a notifiable disease. Associated with the ingestion of soft cheeses and other stuff, problem is that is grows at low degrees. At risk ppl of listeriosis: - elderly - newborns - pregnant - immunocompromised. Clin Mani - listeria-induced gastroenteritis after 1-2 days incubation - secretory diarrhoea Complications: pregnancy associated - BAC travels over placenta -> either neonatal early onset sepsis or neonatal meningitis (late onset meningitis 2-3 wks after birth). meningitis also in elderly, immunocompromised. Diag - blood culture and CSF on selective medium Treatment - Self-limiting in immunocompetent but can be invasivein "at risk populations" (neonates, woman who arepregnant, elderly, immunocompromised) - Consider penicillin/ampicillin/gentimcin. Seek expertadvice |
|
|
Bacillus cereus |
G +ve B. cereus is aerobic, rod, commonly from soil and water. In particular is affects rice. Clin Mani 1. Emetic syndrome - caused from a heat stable enterotoxin which is cannot be killed by heating it up. after 1-5hr incubation: Vomiting, abdo cramps, short lived 2. Diarrhoeal syndrome - from heat-labile enterotoxin. after 6-14 hr incubation: secretory diarhhoea, cramping - duration is 12-36 hours. Treatment illness short lived (usually <10 hrs)Self-limited. Consider antiemetic agents in presentationof violent vomiting Self-limiting. Duration 12-36hrs. Supportive rehydration . |
|
|
Staphylococcus aureus |
G +ve Clin mani: it produces an enterotoxin. After 1-6 hr incubation: fever, cramping, violent repeatedretching and vomiting. Secretory diarrhoea (mild) Treatment Short lived illness (6-8 hrs). Antiemetic agents inpresence of dehydration and vomiting, especially forelderly, infants and children, and patients with underlying disease |
|
|
Norovirus |
calciviridae family (non-enveloped, single-stranded RNA virus). Many genotypes but mostly G1 the most common. Most common cause of gastroentoritis. Presents in older children and adults. Transmits via faecal-oral contact. Outbreaks occur: - hospitals - buffets Clin Mani - symptoms are abrupt (~24 hr incubation) - secretory diarrhoea (more in children) - vomiting projectile (more in adults) - illness remains infections some time after feeling better. Diag - from acute clin mani in a community outbreak setting. Treatment - hydration |
|
|
Rotavirus |
From reoviridae family. Seen in infant population (Major cause of diarrhoea in <6m of age)). Double stranded RNA that is non-enveloped. There are outer and inner layer proteins of the cuspid. Outer are involved for attachement of virus. VP6 of inner is used in the diagnostic testing. Faecal-oral route transmission. Can be in fomites alot as can survive. Hospotalised infants. Clin Mani - symptomatic is contagious. - Vomiting - secretory diarrhoea (most in infants and so causes severe dehydration) Diag - electron microscopy - Polyacrylamide gel electrophoresis - PCR approach Treatment - Oral or IV fluids - Vaccine: Rotarix and Rotateq (a reassortment vaccine from bovine-human) |
|
|
Adenovirus |
From adenoviridae family. A double stranded DNA virus. Non-enveloped, single layer cuspid. Serotypes 40, 41 NS 42 mostly cause acute gastroenteritis. Faecal-oral contact trans. causes diarrhoea. Clin Mani - secretoru diarrhoea - can cause with resp conditions - duration is 5-12 days - there are extra intestinal manifestations (conjunctivitis, high fever, foot in mouth disease) Diag - antigent detection kits. Treatment - supportive therapy |
|
|
Salmonella species Salmonella (nontyphoid) |
Clinical features: Salmonellosis: After 8-48hr incubation:fever, abdominal pain, nausea, and vomiting;secretory diarrhoea; symptoms abate 2-5 days Complications: bacteremia; Reiter's syndrome Diag: - nationally notifiable disease - stool or blood cultures - MacConkey agar positive - Salmonella shigella agar Management: Antibiotics NOT indicated for otherwise healthy patientsFor elderly/immunocompromised/children considerazithromycin, ceftriaxone, or ciprofloxacin |
|
|
S. Typhi; S. Paratyphi |
Clinical features: typhoid fever can be preceded by diarrhoea.Usually evolves over 3 weeks: Week 1: fever with temperature-pulse dissociation Week 2: abdominal pain and rose spots on the trunk Week 3: hepatosplenomegaly Other complications: bacteremia; cholangitis;pneumonia; endocarditis; osteomyelitis Management: Always treat cases of typhoid/paratyphoid (Azithromycin, cefetriaxone, ciproflaxacin) Follow up to ensure eradication |
|
|
S. Typhi; S. Paratyphi |
Clinical features: typhoid fever can be preceded by diarrhoea.Usually evolves over 3 weeks: Week 1: fever with temperature-pulse dissociation Week 2: abdominal pain and rose spots on the trunk Week 3: hepatosplenomegaly Other complications: bacteremia; cholangitis;pneumonia; endocarditis; osteomyelitis Management: Always treat cases of typhoid/paratyphoid (see typhoid card)Follow up to ensure eradication |
|
|
Shigella species (serovars) S . sonnei (Group D) S. dysenteriae (Group A) S. flexneri (Group B) S. boydii (Group C) |
Clinical features: Shigellosis Most commonly isolated species.Typical symptoms aremild secretory diarrhoea after 24-48hrs incubation. Few,if any constitutional symptoms True dysentery (preceded by secretory diarrhoea) Bloody (inflammatory) diarrhoea; fever, nausea, tenesmusabdominal cramping, vomiting, headache, and myalgias. Profound dehydration. Children <2yrs may have associated neurolgic symptomsIn developing countries, S . dysenteriae associated with HUS Management: Treatment centered around rehydration and restoringelectrolyte balance. To prevent dysentery, all patientstreated with antibiotics. Consider, Ampicillin;Cotrimoxazole; Norfloxacin; Ciprofloxacin |
|
|
Diarrhoeagenic E . coli EHEC (E. coli O157:H7) |
Clinical features: Traveller's diarrhoea, developing countries bad water. After 3-4 day incubation, secretory diarrhoeaProgresses to bloody (inflammatory) diarrhoea withsevere abdominal cramping; pain; vomiting; fever usually low grade*(distinguishing feature from otherinvasive intestinal pathogens Complications: HUS and thrombotic thrombocytopenicpurpura; usually appear 5-20 days after onset of infection,and diarrhoea can be resolved by time of diagnosis Management: Uncomplicated, resolves in 7-10days; carrier state lastsanother 1-2 weeks but resolves spontaneously.Supportive (maintain rehydration) Complications: usually common in children, elderly, andimmunocompromised. Antibiotics contraindicatedmight increase expression of toxin and onset of HUS.Usually blood transfusion/dialysis part of HUS treatmentprogram |
|
|
Diarrhoeagenic E . coli ETEC |
Clinical features: common cause of traveller's diarrhoea. After 24-72hrincubation: abrupt secretory diarrhoea; cramping, vomiting,little to no fever. Recovery without long term sequelae Management: Suspect in cases of secretory diarrhoea with few otherclinical symptoms. Supportive rehydrationIf patient was travelling in endemic countries, |
|
|
Diarrheagenic E . coli EPEC |
Clincial features: Major cause of infant (<2 yrs old) diarrhoea in developingcountries; major cause of traveller's diarrhoea inMexico and North Africa. After 6-48hrs incubation:profuse and persistent secretory diarrhoea; cramping,vomiting, severe dehydration. Management: Supportive rehydration; short course Ciprofloxacin |
|
|
Yersinia enterocolitica |
Clinical features: Prevalent throughout Europe and developing nations. Affects all ages, but infants and young children most at riskAfter incubation (~4-6 days), fever, abdominal cramps secretory to bloody diarrhoea (lasting 10-14 days or longer),vomiting, malaise, and anorexia. In adolescents and youngadults pseudo-appendicitis (with no diarrhoea). Post-infection complications: erythema nodosum, Reiter'ssyndrome; numerous extraintestinal complications Management: Diarrhoea is self-limited. Antibiotics can decreasefaecal shedding. Consider doxycycline plusgentamicin/ or single Ciprofloxacin (short course forimmunocompetent patient; 7-10 days forimmunocompromised) |
|
|
Vibrio parahemolyticus and V. vulnificus |
Clinical features: After ~8-12 hrs incubation: explosive secretory diarrhoeavolumes less than cholerae; headache, nausea, vomiting.Wound infections. Septicemia in patients with underlyingdisease Management: Rehydration therapy plus doxycyclineWounds: consider doxycycline and required surgicalmanagement |
|
|
signs and symps of viral hepatitis |
generalized/variable: - malaise, anorexia, nausea, vomiting - joint and muscle pain - Dark urine, diarrhoea/constipation, pruritis - jaundice - hepatomegaly, splenomegaly - systemic symptomes of fever/rash/arthritis - other immune complex mediated disease - hepatic failure: mental status change, coma, death |
|
|
Hepatitis A |
Heparnavirus - RNA virus - survives well (fomites) Trans: faecal/oral life cycle - oral inoculation of faeces contaminated -> trans across GIT epithelium to mesenteric veins of liver -> taken up by hepatocytes where is replicates and is shed off into bile canaliculi -> transported to intestine and excreted in faeces. At risk ppl: - man-man sexual intercourse - IV drug use - children in daycare - travellers and military - sewage workers Cx: No Chronic infection Ix: - First LFTs (raised AST, ALT and normal APT) to determine likely hepatitis - screen for Anti-HA IgM Mx: - vaccines Complications - for elderly, child, immunocompromised rarely fulminant hepatitis can develop (need a liver trans) - if Jaundice lasts for 7 days before encephalopathy then liver trans also.
|
|
|
hepatitis C |
AKA HCV or Flavivirus Trans: blood-to-blood Cx: Incubation period - ~6-7 wks average - jaundice more common 30-40% - Persistant infection >85% - Chronic hepatitis 70% (cirrhosis 10-20%, HCC 1-5%) Prevention: - No vaccine - screening of blood, organ, tissue donors - reduction in high risk behaviours Ix: - First LFTs (raised AST, ALT and normal APT) to determine likely hepatitis - serology for Anti-HCV indicates exposure - followed by PCR for HCV RNA Monitoring - HCV RNA |
|
|
hepatitis E |
AKA Hepevirus - RNA virus Epi: most common cause of acute Hep in Asia Trans: Faecal/oral trans Ix: - First LFTs (raised AST, ALT and normal APT) to determine likely hepatitis Clin features: - incubation period 40 days - severity of illness increases with age - fatality increased dramatically with pregnant. Chronic sequence - No Chronic Infection can develop - In developed countries, Hep E can progress to Chronic Hepatitis and chronic liver disease only in immunocompromised Pts. Prevention and control: - dont drink water that is not bottled. |
|
|
Hepatitis B |
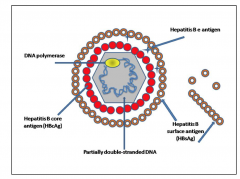
Hepadnaviridae - partially double stranded DNA virus Trans (blood/body fluid): - percutaneous (needles, biting,) - permucosal (sex, perinatal,)
Cx: - incubation of 45-180 days (long) Yes Chronic infection - <5 yrs old at infection : 30-90% of dev chron - >5 yrs old: 2-10% Jaundice acute case -fatality rate: ~1% Premature mortality from Chronic Liver Dis: 15-25% Ix: - First LFTs (raised AST, ALT and normal APT) to deterine likely hepatitis - Anti-HBsAg Hep B antigens: - HBsAg = surface antigen (Abs against = indicate immunity, but if persistant it indicates infectivity) - HBcAg = Core antigen - HBeAg = Infectivity related (this + Abs against this = serological markers of infection) Complications: - Fulminant (1% of cases) - Relapses (15%) - Chronic infection (5-10%) can lead to hepatocellular carcinoma, chronic persistant hep, Chronic active hep Risk groups - ppl who have had sex with infected person - IV drug users - STDs (so ppl with multiple sex partners) - infants of HBV infected mothers - occupations with blood exposure - recipients of unscreened blood products - hospital stays Prevention and Prophylaxis - blood donor screening - destruction of sharps and sterilisation of instruments - education - Pre/post immunizations through primary vaccine (HBsAg) and passive vaccine (HBIG) Chronic infection treatment: - IFN-alpha (>4 months) - if > 1 yr then lamidivudine or entecavir |
|
|
Helicobacter Pylori |
gram -ve, catalase +ve, oxidase +ve, grows on special media (choc agar), non-sporulating curved or spiral shaped bacillus. Epi: developing countries infection ratees as high as 70-90%. Major risk factors; - crowded living - poor hygiene - poor sanitation Trans: gastric-oral (vomiting), oral-oral (H. pyloris survives after reflux), faecal-oral. Pathophysiology: virulence factors allow H. pylori to survive in the stomach: - Motility (by polar flagella) & mucolyticenzymes - Urease* (converts Urea -> ammonia + CO2, the ammonia damages host) - Adherence factors* - Superoxide dismutase* - Catalase* - VacA* vacuolating-toxin (enduces vacuol formation in eukaryotic cells. Only 50% of H. pylori are able to produce toxin) - pathogenicity island (PAI) and CagA* (the H. pylori genome has large PAI inherited via horizontal gene transfer. These PAI contain genese that: encode type-IV secretion systems. Phosphrylation of the CagA results in pedestal formation) H. pylori is generally not invasive, but it doesinduce a strong immune response. Clinical manifestations Signs and symptoms of acute infection: After an incubation period of ~ 7 days or so, patient’s can present with: - “Burning” pain or discomfort (tenderness) in the upper abdomen (ie., dyspepsia) - Bloating (feeling of being “full”) after a small meal - Persistent episodes of nausea and vomiting - Diarrhoea - Fatigue - Fever (?) - Weight loss - Dark stools - Manifestations last ~3-14 days Chronic infection: - (Pan)-gastritis - Dysregulation of the inflammatory immune response (invasion of gastric mucosa by neutrophils,eosinophils and basophils) lymphocytes (T and Bcells), macrophages and plasma cells - Not every acute infection leads to chronicinfection; and not all chronically infected peopleare symptomatic - Chronic infection can have varyinggastrointestinal disease outcomes Clinical outcomes - duodenal ulceration - gastric ulceration - Chronic inflam leads to parietal cell loss -> chronic atrophic gastritis which is one step away from gastric cancer (gastric adenocarcinoma). - MALT lymphoma Diag - Urea breath test - Faecal antigen test - serology (but cannot distinguish between the current or previous cases)\ - endoscopy Treatment indicated for peptic ulcers, MALTomas. - Proton pump inhibitor triple therapy {PPI (twice daily) + amoxicillin (twice daily) +clarithromycin (twice daily; for 7 to 10 days)} - Quadruple therapy: PPI (twice daily) + metronidazole (3 timesdaily) + tetracycline (3 times daily) +bismuth salts for 7 or 14days- Sequential therapy: PPI (twice daily) + amoxicillin (twice daily)for 5 days followed by PPI (twice daily) + clarithromycin (twicedaily) + tinidazole (twice daily) for 5 days |
|
|
Hepatitis D |
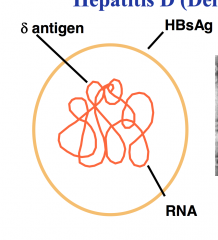
AKA RNA "viroid" Trans: percutaneous and permucosal exposures Two types of infection: - Co infection - Superinfection Prevention: - ForHBV-HDV co Infection prophylaxis to HBV infection - For HBV-HDV superinfection education and reduction in risky behaviours. Cx: - yes chronic infection |
|
|
What is diarrhoea? what are the3 most common bacterial causes of infectious diarrhoea and how they are contracted? |
3 or more loose or watery stools per day or a decrease in consistency + increase in frequency compared to normal individual.Campylobacter (poultry, milk)> salmonella (eggs, poultry, milk, meat) > shigella ( > E. Coli Transmission from contact with an individual who has it, or you may get it after eating contaminated food or drinking contaminated water. |
|
|
Which tests are used for differentiating viral and bacterial causes of diarrhoea. |
Majority of acute infectious diarrhoea is viral. Severe diarrhoea is usually bacterial.Processobtain history (including hypovolaemia, travel, day care hx, diet, sexual Hx, MEDx) and physical examination -> evaluate severity and duration of diarrhoea -> treat dehydrationTests include:- stool sample for culturing- colonoscopy (for pseudomembranous colitis)- readiology (dilated LI, thickening of the wall, sometime unexplained ascietes)- test for C. difficile Toxin A +/- B |
|
|
How does clostridium difficile cause diarrhoea and how is this diagnosed. |
There are hypercirulent C. Difficile strains (that produce 20x more toxin).pathogenesis:upregulatino of transciption factors for toxins A and B occurs in BAC. Then toxin is release from BAC and binds to cell-surfcae receptor -> internalisation of toxin and intracellular actions occur.Clinical features:Severe CDI- fever >38.5 C˚- acute abdomen- ileus and toxic megacoloninvestigations- colonoscopy (presence of pseudomembranes is assoc with severe disease)- Radiology (dilation of LI, thickening of wall, unexplained ascites, perforation)Diag- detect organism (culture)- detect toxin (cytotoxic assay)- detect toxin coding genes |
|
|
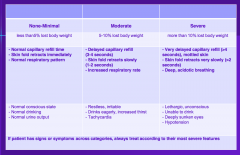
staging of dehydration in diarrhoea |
|
|
|
What are findings that suggest development of peritonitis from C. Difficile diarrhoea infection? |
Severe CDI- fever >38.5 C˚- acute abdomen- ileus and toxic megacolon- peritonitis/bowel perforationLab- WCC > 15x 109- Elevated lactate level- rise in creatine level- albumin <25 mg/l |
|
|
factors that complicate UTIs |
Functional or anatomic abnormality of urinary tract Male gender Pregnancy Elderly patient Diabetes Immunosuppression Childhood UTI Recent antimicrobial agent use Indwelling urinary catheter Urinary tract instrumentation Hospital-acquired infection Symptoms for more than 7 days at presentation |
|
|
Cystitis |
superfifiacl infection of the bladder mucosa, F>M (due to short urethra) Symptoms » Dysuria » Frequency and/or urgency » Suprapubic tenderness* » Haematuria* » Nocturia » Cloudy,foul-smellingurine » Fever and chills are not usually present* Lab Diag - urinalysis (mid stream) DDx: Vulvovaginitis - vaginal discharge shows presence of inflam cells. Urethritis - Urethral discharge with inflam cells. Treatment: Non-pregnantadultwoman: » Trimethoprim » Cephalexin » Augmentin » Nitrofurantoin » If resistance to all of above drugs proven;norfloxacin |
|
|
Pyelonephritis |
Symptoms – Abrupt onset of chills* – Accompanied by dysuria, frequency, and urgency – Fever (can be ≥ 38oC) – Nausea and vomiting* – Unilateral/bilateral flank(costovertebral angle) pain Lab Diag - Urinalysis - reveals bacteriuria, and WBC casts - blood cultures for hospitalised patients withe systemic toxicity (e.g SIRS) Treatment - Mild to moderate infection (10-14days): » Cephalexin » Augmentin » Trimethoprim » If resistance to above; ciprofloxacin or norfloxacin Severe infection: » IV gentamicin plus amoxycillin/ampicillin » Gentamicin contraindicated: IV ceftriaxone or cefotaxime |
|
|
Prostatitis |
Acute prostatitis symptoms - Perineal pain - Dysuria, frequency, urgency - Fever - Prostatic tenderness (on rectalexamination) Lab Diag - Urine culture - Urine analysis reveals pyuria and bacteriuria |
|
|
specimen collection urinalysis |
midstream urine. Quick transport or refrigeration, |
|
|
Escherichia coli and Proteus mirabilis |
E. coli (most common) - normal gut flora P. Mirabilis - normal gut flora both Gram -ve |
|
|
Pseudomonas aeruginosa, Staphylococcus saprophyticus, staphylococcus aureus. For UTIs |
P. aeruginosa - can be normal or acquired. S. saprophyticus - 5-10% community acquired UTIs. Coag -ve, honeymoon cystitis. S. aureus - coag +ve, UTI occurs via haematogenous spread. |
|
|
Enterococcus and Streptococcus in UTI |
Enterococcus species - More common in hospital than community - E.faecalis, E.faecium - Normal flora in the gut Streptococcus agalactiae - <2% of community and nosocomial UTIs - “Group B Streptococcus” - Normal flora of gut (+/-vagina) - Important neonatal pathogen - Always treat in pregnant women(even if reported as part of mixed growth) |
|
|
Candida |
5% of nosocomial (hospital originating) |
|
|
Lab diag in UTIs |
Microscopic examination of urine - Urine might show presence of: – Pyuria: defined as ≥ 10 x 106 leukocytes / L – Haematuria: erythrocytes ≥ 12 x 106 / L NOTE: Presence of RBC might also be indicative of other disorders like tumours, vasculitis, and glomerulonephritis – Bacteriuria : bacteria present at ≥ 108 / L* Contamination of sample: squamous epithelial cells present at ≥ 10 x106 / L Rapid indirect (Dipstick) methods - Presence of urine nitrite: – Bacteria convert nitrate present in the medium to nitrite - Presence of pyuria detected by: – Leukocyte esterase test NOTE: A negative leukocyte test plus negativenitrite test are strongly predictive of the absenceof UTI |
|
|
Syphilis (treponema pallidum) |
General - needs tissue culture to grow, but still only lasts a few generations. - lack ability to make growth factors. trans - skin abrasions - cross placenta into foetus 1˚ phase - 1 lesion develops 10-90 days after infection at point of entry of BAC. -> papule soon erodes epithelium into an ulcer -> untreated will generall heal spntaneously, but pt still infectious. 2˚ phase (disseminated stage) - pts show flue like symptoms (including mucocutaneous rash of entire body) -> if untreated symps generally resolve and pt enters latern phase. 3˚ phase (latent phase) - if <2 years since infection pt can go back to stage 2˚. - If >2 yrs since infection , can progress to stage 3˚ - 3˚ shows neurosyphilis (with argyll robertson pupils) - granulomatous syphilis. Congenital syphilis. - death or multi-organ malformations. - If survive inital stage of disease will present with: Hutchinson's teeth, saddle nose, sabre shins. Lab Diag - Dark field microscopy - TPA test (treponema-pallidum particle agglutination) - Non-treponema test is then used to monitor management. |
|
|
Bacterial Vaginosis |
Epi - most noted in women who have sex with women. - Microscopy shows coccobacilli of various names. - have this increases women's risk of getting other STIs Clin Mani - fishy vaginal odour (amine volatile at increased pH) Diag Criteria 1. homegenous vaginal discharge 2. Vaginal pH > 4.6 3. +ve whiff test (amines) 4. presence of clue cells. Treatment - metroidazole oraly |
|
|
Trichomona vaginalis |
Epi - 50% of all curable diseases worldwide. - it may cause urethritis in men but often asymptomatic. Pathophysiology 1. trophozoite in vaginal and prostatic secretions and urine (diagnostic stage) -> 2. multiply by longitudinal binary fission -> 3 trophozoite in vagina or orifice of urethra (infectious stage). Clin Mani - in women micro-ulcerations via direct contact with BAC. - colpitis macularis (strawberry cervix) - in men recognised as a cause of NGU. Lab Diag - microscopic exam of vaginal fluid - pH>4.5 - +ve whiff test (amines) - PCR Treatment - metronidazole (same as B. vaginosis) |
|
|
Klebsiella granulomatis |
Epi - encapsulated, G -ve bacillus, causes genital ulcers in certain populations (India, PNG, etc) Cli mani - painless smalle papules - red 'beefy' ulcer - rolled edges that bleed on contact - in men -> prepuce, corona, shaft - in women -> labia, rarely other place.s Diag - on clin mani - confirmed by "donovan" bodies on histological exam. treatment - azithromycin (orally) 1/52 |
|
|
Candida Albicans |
Epi - is the cause of 85% of volvovaginal candidiasis. - About 75% of women will have at least 1 episode of V candidiasis. Clin mani - abnormal discharge is usually thick and adherent (cottage cheese) Diag - Vag pH normal - -ve whiff test - microscope shows yeast cell and hypheal forms - culture vaginal material. Treatment - uncompliated infection - vaginal topical agent - Complicated Infection - vaginal agents for long periods. |
|
|
Chlamydia trachomatis |
general - obligate intracellular bacteria (ie feeds on hosts cells for energy ATP). - Tropism for epithelial cells (preference for BAC to grow on these cell types) - Biphasic life cycle: elementary body is the infectious form of BAC and is extracellular -> Reticulate body are the replicative form of the BAC that is intracellular in phagosomes. Epi - Biovars (trachoma and LGV) - Trachoma has 15 serovars; Types A to C causes trachoma and other cause Urogenital tract disease - LGV has 4 serovars; all cause LGV (lymphogranuloma venereum). Trachoma - causes chronic keratoconjunctivitis, mostly children. Its trans via eye to eye contact (eg. hands as fomite). In adults a genital infection precedes eye infection. Urogenital tract disease in women is mostly asymptomatic, but symptomatic in urethritis. Neonatal conjuntivitis can occur during passage of baby in birth. Ater 5-12 days incubation baby's symptoms occur. Infant pneumonia can also occur, onse 2 - 3 weeks after birth. Urogenital infections in men - see purulent discharge in urethritis. LGV has 2 stages. stage 1 - painless lesion 1-4 weeks after incubation stage 2 - systemic symptoms, pts can also present with anorectal involvement. tertiary stage - if untreated and fibrosis occurs. Lab diag for C. trachomatis - specimen from site of infection -> PCR Treatment - LGV - doxycycline - genital infection disease - azithromycin - Neonate conjuctivitis - azythromycin - Trachoma - azithromycin |
|
|
Other causes of non-gonococcal urethritis (NGU) - M. Hominis - M. Genitalium |
M. Hominis - Bacterial vaginosis - pelvic inflammatory disease - post partum fever M. Genitalium - Pelvis inflamatory disease - but also endometritis and cervicitis. Lab Diag - collect specimen from site of infection -> PCR Treat - doxycycline |
|
|
Neisseria Gonorrhoea |
General - G -ve - fastidious (requires chocolate agar) Epi - 15-29 y/o - asymptomatic carres as reservoir - the symptoms depend on site of infection (rectal and pharyngeal more likely asymptomatic) Cx in males - urethritis, dysuria or asymp Complications - asending infection -> other structures related to urethra (e.g prostate) Cx in females - cervicitis, urethritis, gland infection, Complications - asending infection Other Cx for both genders - disseminated infections: septicaemia symps - other syndromes: purulent conjunctivitis in newborns, anorectal gonorrhoea. Lab diag - culture, use special swabs (dacron and rayon) - don't refridgerate - first pass urine for PCR treat - ceftriaxone + azithromycin - for disseminated disease IV Abx then do culture and susceptibility tests to then decide to switch to normal regime. |
|
|
HPV |
General - DNA viruses - Non-Enveloped - Grouped on predominant anatomic locaiton Cx: - causes Skin warts and anogenital warts - most asymptomatic, but if they are then itching, burning and painful. - anaogenital warts in males Cx as hirsutoid papillomatosis appears as a pearly penile papule. - anogenitaa warts in females is more likely perineum>vagina>anus>cervix>urethra. Also aceto-whitening of cervix when acetic acid washed over. - Cervical intraepithelial neopplasia (CIN) assoc with infections of HPV types 16,18,31 and 45. Px: infect squamous epithelium -> proliferate forming warts. Epi: - 15-44 y/o Complications: - penile intraepithelial neoplasia - Vulvar intraepithelial neoplasia - vaginal intraepithelial neoplasia - anal cancer Lab Diag - Pap smear - PCR of cervical swabs looking for DNA - screen for other STI's to rule out. Prevention - gardasil vaccine |
|
|
HSV |
general - causes primary and recurrent disease - 2 types that are not distinguishable clinically. Trans - HSV-1 mainly spread via oral contact - HSV-1 mainly spread via sexual contact Epi - most common cause of genital ulcers in Aus pathogenesis - infect trigeminal and sacral ganglia. Cx: - genital infection - inguinal LN enlargement, Dysuria, - In men -> clear vesicles on glans and shaft of penis - In Females -> itching and vag discharge - Recurrent gentil herpes through reactivation of latent HSV in sacra ganglion. HSV-2 more likely to produce recurrent infection. Complications - Encephalitis (RBC in CSF -> assoc w seizures, other neuro abnormalities) - meningitis (from HSV-2) - Keratitis (HSV-1 usually) - neonatal infections by HSV-2, prevention might involve caesarian birth Lab Diag - Tzanck or PAP test - cell culture - PCR Serology treat - antivirals - seek advice on pts with pregnancy |