Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
107 Cards in this Set
- Front
- Back
|
Superficial mycoses are limited to these parts of the body
|
non-living tissues such as skin and hair
|
|
|
Cutaneous mycoses are found in these parts of the body
|
skin, scalp, nails
invade and persist in living tissue |
|
|
Subcutaneous mycoses are found in these parts of the body
|
deeper infections that are mostly limited in scope to the skin, muscles, fascia
|
|
|
Factors that limit SCS mycoses:
|
1. innate resistance to fungal infections
-cellular, not humoral 2. fatty acid content 3. pH = fungi like acid 4. cellular turnover 5. normal bacterial flora 6. limited iron content |
|
|
_______ immunity controls fungal infection
|
Cellular
|
|
|
Cellular immunity against Fungi:
-PRR domain proteins like __1__ -__2__ |
1. Card9
2. Toll-like receptors |
|
|
How are Superficial mycoses diagnosed?
|
Direct Observation and culture
|
|
|
Do superficial mycoses elicit an immune response?
|
NO
|
|
|
Superficial mycoses includes things like...(3)
|
Pitryiasis versicolor
White and Black Piedra Tinea Nigra |
|
|
Pityriasis versicolor is caused by this yeast
|

Malassezia furfur
|
|
|
Properties of Malassezia furfur
|
Often asymptomatic
Normal flora Colonizes kids soon after birth |
|
|
Pityriasis Versicolor is in this part of the skin
|
Strateum Corneum
|
|
|
Malassezia furfur is _________
|
lipophilic
-requires special medium |
|
|
Malassezia furfur is often in the __1__ or areas rich in __2__
|
1. Torso
2. Sebaceous glands |
|
|
Pityriasis Versicolor:
-sometimes seen around __1__ -can cause infections around indwelling __2__ -infections can be __3__ -most often in __4__ or in __5__ |
1. puberty
2. catheter 3. widespread 4. tropics 5. summer |
|
|
Pityriasis Versicolor:
-related to fungi that cause __1__ on grain crops |
Bunt or Smut
|
|
|
Diagnosis of Pityriasis Versicolor
|
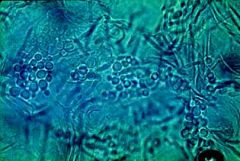
'spaghetti and meatballs' appearance of the organism in KOH cleared specimen
|
|
|
DOC's for Pityriasis Versicolor
*ineffective drug? |
Fluconazole or Itraconazole
*Terbinafine |
|
|
Drug recommended for Pityriasis Versicolor in patients with catheter infections
|
Amphotericin B
|
|
|
Topical treatments that may be considered for Pityriasis Versicolor
|
Selenium or dandruff shampoo
|
|
|
Tinea Nigra etiologic agent
|
Exophiala Werneckii
|
|
|
Tinea Nigra most often occurs on this part of the body
|

Palms or soles
|
|
|
Tinea Nigra can be confused with these things
|

Melanoma
Moles Benign pigmentation |
|
|
Places where Tinea Nigra are usually seen
|
South or Latin America
Africa |
|
|
Tinea Nigra is limited to this part of the skin
|
Strateum Corneum
*no inflammation* |
|
|
Tinea Nigra appearance in KOH cleared tissue
|

abundant dark branched septate hyphae from 1.5-5 micrometers in diameter
|
|
|
Tinea Nigra grow on this agar
|

Sabourauds glucose at 30'C
*they are mucoid colonies *become dark green to black with time |
|
|
Tinea nigra treatment
|
topical antifungal applied for 2-4 weeks
*can be surgically removed or systemic antifungals |
|
|
Black Piedra etiologic agent
|
Piedra Hortae
|
|
|
Describe Black Piedra
|
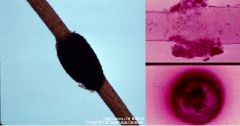
-superficial hair infection
-nodules on hair of head are SEXUAL fruiting bodies and contain Ascospores |
|
|
Most frequently infected area of body with Black Piedra: __1__
Most cases are __2__ and may remain so for __3__ |
1. scalp hair
2. asymptomatic 3. years |
|
|
Diagnosis of Black Piedra
|
Direct Observation
Culture |
|
|
Black Piedra treatment
|
shaving or clipping hair
Topical or Oral Azoles Terbinafine |
|
|
White Piedra etiological agent
|
Trichosporon Beigelii
|
|
|
Describe White Piedra infection
|

Superficial hair infection
|
|
|
Trichosporon is a normal member of the flora of these body sites
|
Mouth
skin nails |
|
|
A ______ bacterial infection can be present along with Trichosporon (White Piedra)
|
Coryneform
|
|
|
White piedra affects these animals in addition to humans
|
Horses and monkeys
|
|
|
Taxonomy of White Piedra
|
Basidiomycete, related to Cryptococcus
|
|
|
Clinical significance of White Piedra
|
IC'ed hosts at risk to develop invasive infection
-lungs -kidneys -spleen |
|
|
White Piedra are more often seen on these hairs
|
Pubic or Axillary hairs
|
|
|
Treatment of White Piedra
|
Shaving or Clipping hair
Oral Itraconazole |
|
|
One case of disseminated White Piedra infection was reported as having been treated with _________
|
Capsofungin
|
|
|
Cutaneous Mycoses infect ______ tissue and elicit ______
|
Living tissue
immune response |
|
|
Cutaneous mycoses are often called__________
|
Dermatophytes
|
|
|
3 prominent genera of Cutaneous Mycoses
|
Epidermophyton
Trichophyton Microsporum |
|
|
All cutaneous mycoses are ________
|
Mitosporic Ascomycetes
*mitosporic = reproduce by mitosis, asexual |
|
|
Cutaneous Mycoses includes these clinical infections
Severity of infection is related to ________ |

Athletes Foot
Onychomycosis Ringworm (=Tinea) Immune status of the host |
|
|
Tinea corporis = 1
Tinea Capitis = 2 Tinea Cruris = 3 Tinea Barbae = 4 Tinea Pedis = 5 Tinea unguium = 6 |
1. body ringworm
2. scalp 3. jock itch 4. beard 5. athletes foot 6. onychomycosis/nails |
|
|
Term for Dermatophyte fungi associated with humans
|
Anthrophilic
|
|
|
How is Tinea diagnosed?
|
Visualization of fungi in specimen
Lesion characteristics |
|
|
List the 3 Zoophilic Tinea
|
-Microsporum canis
-Trichophyton mentagrophytes var Metnagrophytes -Trichophyton verrucosum |
|
|
Explain the significance of the Woods lamp
|
Fluorescence does indicate the presence of Fungi, but lack of fluorescence does not indicate absence of fungi
|
|
|
Most common fungal complaint?
|

Tinea Pedis (athletes foot)
|
|
|
DOC's for Tinea Pedis
1. Simple cases 2. More effective approach 3. Moccasin infections |
1. topical Allylamines, Azoles
2. Terbinafine applied 2X daily 3. Oral Terbinifine or Itraconazole for widespread or prolonged infection |
|
|
Tinea corporis occurs on this part of the skin
|

relatively HAIR-LESS
|
|
|
What distinguishes Tinea Corporis from a Superficial infection
|
Tinea corporis causes an immune response
|
|
|
Transmittance of Tinea Corporis
|
by pets or from infected people (sharing shoulder pads)
|
|
|
DOC's for Tinea Corporis
1. for few lesions 2. Widespread infection |
1. Topical
2. Oral -Terbinifine -Itraconazole -Fluconazole -Griseofulvin |
|
|
Tinea cruris = ?
|

Jock itch
|
|
|
Dermatophytes that cause Tinea Cruris (4)
|
1. Epidermophyton floccosum
2. Microsporum canis 3. Trichophyton mentagrophytes 4. Trichophyton rubrum |
|
|
If the scrotum is involved in Tinea Cruris, this fungus is involved
|
Candida
|
|
|
Tinea Capitis involves these parts of the body
|

scalp
hair |
|
|
Tinea capitis is most common in these people
|
pre-pubescent blacks
|
|
|
Tinea capitis DOC's
|
Oral
-Griseofulvin -Terbinafine -Itraconazole -Fluconazole *topical not effective b/c drug cannot penetrate into the follicle |
|
|
This is not useful in diagnosing Tinea Capitis
|
Wood lamp
|
|
|
Tinea Barbae are caused by ___________
How do you tell the difference between fungal and bacterial infection? |
Zoophilic Dermatophytes = most common in Farm-workers
Plucking hairs is painless in Tinea Barbae, but painful in bacterial infection |
|
|
Tinea Barbae treatment
|
ORAL
-Itraconazole -Terbinafine *oral b/c infection is deep in follicle |
|
|
Onychomycosis is sometimes called _______
|
Tinea Unguium (a subset)
*T. Unguium is caused by Dermatophyte fungi *Onychomycosis can also be caused by yeast or other molds |
|
|
Onychomycosis is more common in these people
|
Men
Elderly Diabetics *seen in 2-3% of the pop. |
|
|
Most common form of Onychomycosis and its agent
|

Distal and Lateral Subungual Onychomycosis (DLSO)
Dermatophyte fungi -Trychophyton -Epidermophyton -Microsporum |
|
|
DOC's for Onychomycosis
|
Lamisil - oral 6-12 wks
Sporanox - oral, pulse dosing -1 week on, 3 off for 5 months Griseofulvin Loprox (tea tree oil) |
|
|
Downfall of Lamisil (Terbinifine)
|
some Hepatocytoxicity
|
|
|
Downfall of Sporanox (Itraconazole)
|
Hepatotoxicity
Congestive heart failure |
|
|
Cutaneous mycoses can also include ___________
|

mucocutaneous candidiasis
|
|
|
Mucocutaneous Candidiasis is a _______ infection of men and women
-it is in the _____ of all mammals |
yeast
GI tract |
|
|
Way to diagnose Mucutaneous Candidiasis of the vagina
|
Candida in WET MOUNT of vaginal smear
|
|
|
DOC's vaginal candidiasis
|
Clotrimazole cream/tablets
Oral Fluconazole |
|
|
Orophayngeal Candidiasis is more common in these people
|
Nursing babies
AIDS |
|
|
DOC's for AIDS Oropharyngeal Candidiasis
|
Lozenges of Clotrimazole or Nystatin
|
|
|
How are Subcutaneous Mycoses infections usually obtained?
|
following trauma
|
|
|
Subcutaneous Mycoses infections characteristics
|
-can be life threatening (difficult to treat)
-grow thru tissue and cause surface lesions -usually follow trauma -course of infection often many years -considered rare and exotic in USA -infect otherwise healthy people |
|
|
How are Sporotrichosis infections often acquired?
|
puncture wound (rose thorn)
|
|
|
Sporotrichosis is associated with __1__, and outbreaks among __2__ workers
|
1. sphagnum moss
2. nursery |
|
|
Sporotrichosis follows the _____ that drain the site of inoculation
|

Lymphatic glands
-lymph nodes are usually not involved |
|
|
Sporotrichnosis:
-lesions sometimes mimic __1__ -sometimes called "__2__" |
1. Blastomycosis
2. rose gardener's thumb |
|
|
How is Sporotrichosis diagnosed?
|
-pattern of infection
-culture from tissue at 30'C, dimorphism is demonstrated by switching culture to 37'C |
|
|
Treatment of Sporotrichosis (3)
|
-ORAL SATURATED POTASSIUM IODIDE
-Itraconazole for subcutaneous disease -AmphotericinB for disseminated |
|
|
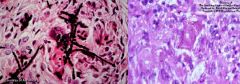
Describe Chromoblastomycosis lesions
|

chronic warty/verrucous nodules of epithelial tissue overgrowth caused by abnormal # and arrangement of cells
|
|
|
What initiates Chromoblastomycosis lesions?
How much do they grow per year? |
trauma
~2 mm/year = very slow growing |
|
|
How is diagnosis of Chromoblastomycosis made?
|

Examination of Clnical Material
-Sclerotic cells or "Medlar bodies" are characteristic |
|
|
Chromoblastomycosis are caused by a variety of __1__ fungi that are found in these places: __2__
|
1. dematiaceous = dark hyphae
2. soil, decaying vegetation, rotting wood, forest carpets |
|
|
Common fungi causing Chromoblastomycosis
|
Cladosporium carrionii
Fonsecaea Phialophora verrucosa Exophiala |
|
|
Chromoblastomycosis is common in this general area of the world
|
tropics
|
|
|
Chromoblastomycosis treatment
|
Surgery
Cautery with topical antifungals |
|
|
Phaeohyphomycosis lesion
-initiated most commonly by __1__ -can infect these parts of the body:__2__ |

Nodule or cyst
1. wound 2. sinus, brain, bone |
|
|
Diagnostic feature of Phaeohyphomycosis
|
Melanized cell walls
|
|
|
Phaeohyphomycosis commonly causing fungi
|
Exophiala jeanselmei Phialophora richardsiae
Bipolaris spicifera Wangiella dermatitidis |
|
|
Treatment of Phaeohyphomcosis
|
Surgical excision and chemotherapy
-Amphotericin B and 5-Fluorocytosine or Itraconazole |
|
|
2/3's of Mycetoma lesions are on this part of the body
|
feet
|
|
|
Mycetomas are characterized by this lesion
|

Indolent, deforming swollen lesions that contain numerous draining sinus tracts
*may take years to develop |
|
|
How are Mycetomas diagnosed?
|
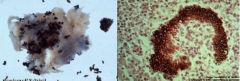
observation of 'grains' of fungal tissue in specimen
|
|
|
Mycetomas are caused by these fungi
|
Pseudallescheria boydii
Madurella mycetomatis Madurella grisea Exophiala jeanselmei Acremonium falciforme Fusarium Scedosporium *Pseudo Madur Exo Acre Fus Sced |
|
|
Organisms that cause Mycetomas are all common ______ fungi
|
soil
|
|
|
Treatment for Mycetomas
|
Surgical debridement
Long-term chemotherapy AMPUTATION |
|
|
3 most common fungi causing Onychomycosis
|
Trichophyton rubrum
Trichophyton Mentagrophytes Epidermophyton Floccosum |
|
|
Causative agent of Superficial White Onychomycosis
|

Trichophyton Mentagrophytes
|