Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
#1
|
Determining the Rhythm
rhythm is either sinus rhythm or not sinus rhythm. (SA node). lead II |
P wave before every QRS complex
upright normal morphology, NSR >100, then “sinus tachycardia” < 60, then “sinus bradycardia” |
|
|
#2
|
no P waves present or the P wave morphology abnormal
-rhythm must be determined -different arrhythmias exist and include |
atrial fibrillation,
atrial flutter, ectopic atrial rhythms, junctional rhythms ventricular rhythms = ventricular tachycardia ventricular fibrillation. |
|
|
what dysfctn occurs when
sinus rhythm is still said to be present. |
Note that when “AV dissociation” is present as previously described (complete heart block or ventricular tachycardia),
there may not be a P wave before every QRS complex, however as long as the P wave is upright in lead II, sinus rhythm is still said to be present. |
|
|
|
LAD
|
left axis deviation
right axis deviation = Can P wave or T wave axis be measured/ |
RAD
Yes |
|
|
To determine the QRS axis, the ____ leads need to be examined
|
limb
(not the precordial leads). |
|
|
|
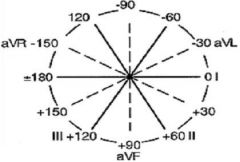
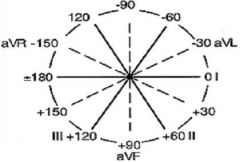
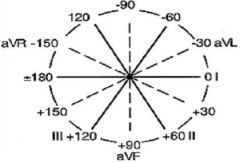
Lead Vectors
I II II AVL AVF AVR |
I = 0
II = +60 III = +120 AVL = -30 AVF = +90 AVR = -150 |
|
|
|
normal QRS axis
Left axis deviation Right axis deviation |
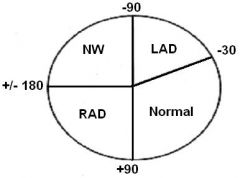
- 30 and +90 degrees.
-30 and -90 +90 and +180 Indeterminate axis is between |
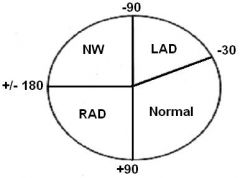
+/- 180 and -90 degrees.
NW = northwest axis or indeterminate axis |
|
|
The fastest, non-specific method to determine the QRS axis is to find the major direction of the QRS complex (positive or negative) in leads
|
I
aVF. |
|
|
|
If the QRS complex is upright (positive) in both lead I and lead aVF, then the axis is
|
normal
|
|
|
|
If the QRS is upright in lead I and downward (negative) in lead aVF, then the axis is between
|
0 and -90 degrees,
likely ____ axis deviation. However, the axis could fall between 0 and -30 which is technically a _____ QRS axis. To further distinguish normal from left axis deviation in this setting, look at ______ If it is downward (negative), then the axis is more towards -90 and left axis deviation is present. |
left
normal lead II. If the QRS complex in lead II is upright (positive), then the axis is more towards 0 degrees and the QRS axis is normal. |
|
|
If the QRS is predominantly _______ in both leads I and aVF, then the axis is indeterminate.
|
downward
If the QRS is downward (negative) in lead I and upward (positive) in lead aVF, then the axis is _________. |
rightward
|
|
|
SA node, the physiological pacemaker. This electrical impulse is propagated throughout the right atrium, and through ____ _____ to the left atrium, stimulating the myocardium of the atria to contract.
|
Bachmann's bundle
As the electrical activity is spreading throughout the atria, it travels via specialized pathways, known as__ ____ from the SA node to the AV node. |
internodal tracts,
|
|
|
Atrial enlargements can =
2ct |
widen the P wave or increase the P wave amplitude.
|
|
|
|
PR interval. This represents the time that it takes for the electrical impulse generated in the
|
sinus node to travel through the atria and across the AV node to the ventricles.
|
|
|
|
normal PR interval is =
or milliseconds (ms). = |
0.12 to 0.20 seconds
120 to 200 Some refer to the PR interval as the PQ interval which can be confusing. |
If no Q wave is present, then the interal is measured from P to R. If no R wave is present, the interval is measured from P to Q.
|
|
|
Multiple abnormalities of the PR interval can occur including =
|
prolongation,
shortening variation from beat to beat. |
|
|
|
A prolonged PR interval indicates delayed conduction of the
|
SA nodal impulse
to the ventricles and is called A short PR interval can be seen then the AV node delay is bypassed such as in = The PR interval will vary in = |
1st degree AV block.
Wolff-Parkinson-White syndrome or Lown-Ganong-Levine syndrome. second degree type I AV block (Wenckebach). |
|
|
PR segement is the area beteween the P wave and the onset of the QRS complex. This is supposed to be isoelectric similar to all segments.
PR segment elevation can be seen in lead ___ due to . |
aVR
pericarditis The PR segment is not commonly referred to since the above mentioned conditions are relatively rare. |
Abnormalities of the Q waves are mostly indicative of myocardial infarctions and are discussed in the ECG criteria review sections. The terms Q wave myocardial infarction and non-Q wave myocardial infarction are old designations of different types of myocardial infarctions where the end result is Q wave development or the absence of Q wave development respectively.
|
|
|
R wave morphology itself is not of great clinical importance, however at times it can vary.
|
In lead V1 the R wave is usually quite small, however if the R wave is large in V1 (greater in amplitude than the S wave), then significant pathology may be present
|
Causes of an R wave to S wave ratio of greater than 1 in lead V1 include a right bundle branch block, Wolff-Parkinson-White syndrome, an acute posterior myocardial infarction, right ventricular hypertrophy and isolated posterior wall hypertrophy (which can occur in Duchenne's muscular dystrophy).
|
|
|
In the setting of a right bundle branch block there may be two ____ -____ present giving the classic _________ ____ appearance of the QRS complex. In this setting, the second R wave is termed =
|
R waves
“bunny ear” R1 R’ “R prime” |
|
|
|
A large slurred S wave is seen in lead I and V6 in the setting of a =
|
right bundle branch block.
|
|
|
|
In the normal ECG, there is a large S wave in ____ which progressively becomes _____ to the point where almost no S wave is present in ___
|
V1
smaller V6. |
|
|
|
The normal duration (interval) of the QRS complex is=
When the duration is between _______ ______ seconds it is intermediate or slightly prolonged. |
0.08 and .10 seconds
(80 and 100 ms). 0.10 and 0.12 A QRS duration of greater than ____ seconds is considered abnormal |
0.12
|
|
|
A widened QRS duration occurs in the setting of a
|
right BBB
left BBB non-specific intraventricular conduction delay ventricular arrhythmias ie: ventricular tachycardia |
|
|
|
T waves should be upright in most leads (except =
|
aVR
V1 T waves should be asymmetric in nature. The second portion of the T wave should have a steeper decline when compared to the incline of the first part of the T wave. If the T wave appears symmetric, cardiac pathology may be present such as _____ . Many abnormal T wave patterns exist . |
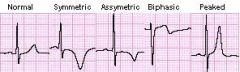
ischemia
|
|
|
normal QT interval
QT interval is less than ______ Females have a ____ QT interval than males. |
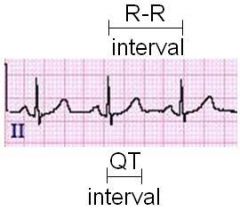
400-440 ms
(0.4 to 0.44 seconds). longer Also, lower heart rates result in a _______ QT interval. |
longer
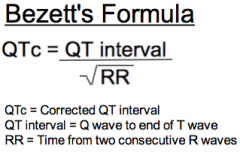
info Due to the heart rates effects, the corrected QT interval (QTc) is frequently used. Slower heart rates normally have longer QT intervals and the opposite is true as well. The QTc corrects for this normal variation of the QT interval with heart rate by incorperating the RR interval (which depends on the ventricular rate). The QTc is considered prolonged if greater than 450 ms in males and 470 in females and is calculated using the Bazett’s formula as below: |
|
|
The ST segment is the portion of the ECG from the =
|
end of the QRS complex to the beginning of the T wave
The ST segment normally remains isoelectric and thus ST segment depression or ST segment elevation can indicate cardiac pathology. |
|
|
|
TP Segment
The portion of the ECG from the end of the |
T wave to the beginning of the P wave.
info |
This segment should always be at baseline and is used as a reference to see if the ST segment is elevated or depressed since there are no specific disease conditions which elevate or depress the TP segment.
During states of tachycardia the TP segment is shortened and may be difficult to visualize altogether. It is good to examine the TP segment closely for the presence of U waves or atrial activity that could indicate pathology. |