![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
28 Cards in this Set
- Front
- Back
|
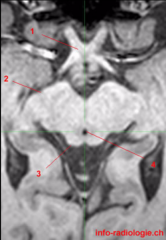
Regarding the anatomy of the midbrain, where does it extend from and to? |
From the level of the trochlear nucleus to the imaginary line drawn between the mammillary bodies and the posterior commissure |
|
|
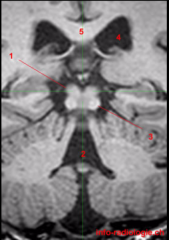
Important structures of the midbrain? (6) |
1. Cerebral peduncles 2. Superior and inferior colliculi 3. The red nucleus 4. Substantia nigra 5. Decussation of the middle cerebellar peduncle 6. CN III and IV |
|
|
Blood supply of the midbrain? |
Depends on the level; lower - perforators from the basilar artery and the superior cerebellar artery; middle and upper - predominantly by the posterior cerebral artery P2 segment |
|
|
Which structures traverse the crus cerebri? |
1. Corticospinal 2. Corticobulbar 3. Corticopontine fibers It is located ventrally |
|
|
Where does the superior colliculus lie? |
In the rostral midbrain dorsal to the cerebral aqueduct (3) |
|
|
What is the role of the superior colliculus? |
It is a visual reflex center, receiving afferent input from the retina, visual cortex and other sensory modalities; also an integral part of the efferent output to burst neurons involved in saccadic eye movements |
|
|
Where is the inferior colliculus located? |
In the caudal midbrain (3) |
|
|
Role of the inferior colliculus? |
Obligatory synapses in the auditory pathway |
|
|
Where is the red nucleus located? |
In the ventral tegmentum ofthemidbrain |
|
|
Main role of rubrospinal fibers? |
Flexion of upper extremity muscles |
|
|
Where is the substantia nigra found? |
Midbrain tegmentum, just dorsal to the corticospinal tracts |
|
|
Which muscles act to widen the palpebral fissure? |
Müller muscle receives sympathetic innervation and the levator of the lid, innervated by cranial nerve III, plays the greater role |
|
|
What is the role of the Edinger-Westphal nucleus? |
Functions in pupillary constriction |
|
|
Compressive lesions of the third nerve complex often result in a pupil-involving third-nerve palsy. Why? And what is the pupil-involvement you see? |
Pupillomotor fibers travel in the outer bundle of the third nerve complex, and that's why you often see pupillary dilation due to impaired parasympathetic component |
|
|
Primary and secondary positions of superior oblique? |
Intorsion and depression |
|
|
Primary and secondary positions of lateral rectus? |
Only primary: abduction |
|
|
Primary and secondary positions of inferior oblique? |
Extorsion and elevation |
|
|
Cranial nerve III has two components. What are they? |
GSE - oculomotor nucleus GVE - Edinger-Westphal nucleus |
|
|
Role of the GSE component of CN III? |
Innervate medial, superior, and inferior recti, and inferior oblique and levator palpebrae |
|
|
Role of the GVE component of CN III? |
Pupillary constriction and accommodation of the lens |
|
|
Where is the trochlear nucleus located? |
At the level of the inferior colliculus |
|
|
The trochlear nerve pathway |
The nerve fascicles course posteroinferiorly around the aqueduct to decussate in the dorsal midbrain in the anterior medullary velum; they den tmerge from the brainstem near the dorsal midline. After traveling on the undersurface of the tentorial edge, the nerve pierces the dura into the cavernous sinus along the lateral aspect. It then enters the orbit through the superior orbital fissure |
|
|
Dysfunction of CN IV may result in? |
1. Hypertropia 2. Excyclotropia 3. Diplopia 4. Head tilt Note that head tilt toward the abnormal side makes symptoms of diplopia worse, recall that a lesion of the nucleus results in contralatreral dysfunction |
|
|
A unilateral oculomotor nerve palsy may result in? |
1. Ptosis 2. Dilated pupil 3. Down (siperior oblique, cranial nerve IV intact) and out (lateral rectus, CN VI intact) eye position |
|
|
A unilateral oculomotor nucleus palsy will result in? |
The same findings as in oculomotor nerve palsy, but will also result in contralateral ptosis and superior rectus dysfunction |
|
|
If there is a lesion at the level above the red nucleus, a patient may have what type of posturing? |
Decorticate due to the influences of the rubrospinal tract (input to flexors of the upperextremity), reticulospinal (predominantly extensor influence of upper and lower extremities), and vestibulospinal tracts (predominantly extensor influence of the upper and lower extremities) |
|
|
If there is a lesion between the red nucleus and the medulla, the patient may have what type of posturing? |
Decerebrate; this results because the input to flexors is removed and the patient mainly has input from the pontine reticulospinal tract and the vestibulospinal tracts |
|
|
Examples of diseases resulting in parkinsonism? |
1. Progressive supranuclear palsy (pallor of substantia nigra and locus ceruleus) 2. Corticobasal-ganglionic-degeneration (intraneuronal inclusions in the substantia nigra) 3. Multiple systems atrophy (neuronal loss in substantia nigra) |