![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
|
What is subcortical dementia? |
Dmentia primarily due to damage to the frontal subcortical connections |
|
|
Typical clinical features of subcortical dementia? (6) |
1. Inattention 2. Bradyphrenia 3. Executive dysfunction (difficulties planning and sequencing tasks) 4. Apathy 5. Psychomotor slowing and mood disorders |
|
|
Cognitive disorders related to cerebrovascular disease consist of 3 major subtypes, what are they? |
1. Vascular cognitive impairment but not dementia (not yet interfering with day-to-day activities) 2. Vascular dementia 3. Mixed vascular dementia and primary neurodegenerative dementia (usually Alzheimer disease) |
|
|
What is the risk of poststroke dementia after a clinical stroke? |
20% |
|
|
How many % of dementia cases are vascular dementia? |
Up to 20% |
|
|
Which is the most common criteria for the diagnosis of vascular diagnosis? |
National Institute of Neurological Disorders and Stroke-ASsociation Internationale Pour la Recherch e et l'Enseignment en Neuroscience |
|
|
Clinical features of Binswanger disease (8) |
1. Early gait apraxia and parkinsonian gait 2. Frequent falls 3. Focal motor deficits and pyramidal signs on examination (extensor plantar responses and exaggerated deep tendon reflexes) 4. Urinary urgency and incontinence 5. Apathy and psychomotor slowing 6. Attention and concentration difficulties 7. Frontal release signs and milder memory deficits than those that occur with other dementias 8. Executive dysfunction |
|
|
What is Binswanger disease? |
The classic syndrome of subcortical dementia from vascular disease |
|
|
Causes of vascular dementia (6) |
1. Hypoperfusion 2. .Hypoxic-ischemic injury 3. Large-vessel injury 4. Small-vessel injury 5. Coagulation disorders 6. Others (superficial siderosis, A beta-related vasculitis) |
|
|
Large-vessel disease that may be a cause of vascular dementia? |
Vasculitis, either granulomatous or systemic |
|
|
Small-vessel disease that may be a cause of vascular dementia? (4) |
1. Binswanger disease 2. Multiple lacunar infarctions 3. CADASIL 4. Spatz-Lindenberg disease |
|
|
Typical location of a stroke that results in apathy and psychomotor slowing? |
Dorsolateral caudate nucleus; recurrent artery of Huebner infarct |
|
|
Typical location of a stroke causing psychomotor hyperactivity, disinhibition, and impulsiveness? |
Ventromedial caudate nucleus; recurrent artery of Huebner |
|
|
Typical location of a stroke causing anterograde and retrograde amnesia? |
Hippocampi; often from hypoperfusion injury, typically bilateral |
|
|
Typical location of a stroke causing altered level of consciousness, lack of spontaneous behaviour, and vertical gaze palsy? |
Paramedian thalamus, Artery of Percheron; artery arisses at basilar bifurcation and supplies paramedian thalamus and rostral midbrain |
|
|
Typical location of a stroke resulting in acute delirium? |
Right parietal lobe |
|
|
Typical location of a stroke causing acalculia, agraphia, left-right dissociation and finger agnosisa? |
Dominant angular and supramarginal gyrus, Gerstmann syndrome; located in parietal lobe |
|
|
Typical location of a stroke causing optic ataxia, oculomotor apraxia, and simultanagnosia? |
Bilateral parieto-occipital lesions, Balint syndrome; often caused by bilateral watershed hypoperfusion infarcts |
|
|
Typical location of a stroke causing left-hand apraxia? |
Anterior corpus callosum |
|
|
Typical location of a stroke causing pseudobulbar palsy? |
Bilateral internal capsule infarcts |
|
|
Typical location in a stroke causing depression? |
Left frontal lobe |
|
|
Typical location in a stroke causing OCD? |
Posterior right frontal lobe |
|
|
MRI findings in vascular dementia? |
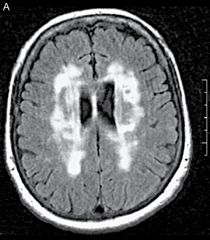
Extensive white matter T2-signal hyperintensities known as leukoaraiosis, which is particularly prominent in Binswanger disease |
|
|
MRI findings in HIV-associated neurocognitive disorder |
Global atrophy and T2-signal hyperintensities in the periventricular and deep white matter |
|
|
Time from infection to onset of neurosyphilis? |
3 to 40 years after infection with T.pallidum |
|
|
How does neurosyphilis present? |
With a frontal dysexecutive syndrome with inattention and executive dysfunction |
|
|
Autoimmune or paraneoplastic cognitive disorders can be broadly divided into two categories. What are they? |
1. Infrequently associated with cancer, which are termed autoimmune encephalopathies or dementias 2. Those associated with cancer, which are often termed paraneoplastic encephalopathies |
|
|
What is probably the most common cause of autoimmune encephalopathy? |
The voltage-gated potassium-channel complex autoantibody |
|
|
How does the voltage-gated potassium-channel complex antibody work? |
They bind to 2 proteins that assocciate with the channel |
|
|
How does autoimmune encephalitis usually present? (4) |
1. Subacute cognitive decline characterized by fluctuations 2. Frequently accompanied by tremor or myoclonus 3. Seizures may also coexist 4. Acute presentations occur as a classic limbic encephalitis |
|
|
When a paraneoplastic encephalopathy is under consideration, what else could be considered? |
Body CT or PET; neuron-specific autoantibodies may rule out paraneoplastic encephalopathy |
|
|
Treatment of autoimmune encephalopathy? |
High-dose i.v. methylprednisolone once daily for 5 days is recommended, and most patients improve within a few weeks |
|
|
NMDA encephalitis is related to which cancer? |
TEratoma, usually ovvarian |
|
|
Cognitive impairment is an underrecognized feature of MS. It affects approximately how many % of the patients? |
60%, although frank dementia occurs in less than 5% |
|
|
Thymomas are associated with which neural autoantibodies? (5) |
1. CRMP-5IgG 2. GAD65 3. Ganglionic acetylcholine receptor autoantibody 4. Glycine receptor antibodies 5. Caspr-2 (VGKC-complex) |
|
|
AMPA neural autoatibody is seen in which cancers? (3) |
1. Thymic tumors 2. Ling carcinomas 3. Breast carcinomas |
|
|
Thyroid peroxidase autoantibodies have been associated with what? |
Something that is termed Hashimoto encephalopathy or steroid-responsive encephalopathy associated with thyroid autoimmunity |
|
|
Supporting features of autoimmune encephalopathies |
1. Evidence of an inflammatory response on CSF examination 2. MRI evidence of T2-signal abnormalities in the mesial temporal lobe |
|
|
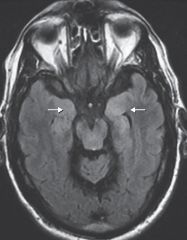
MRI findings in autoimmune voltage-gated potassium channel complex-associated encephalopathy. T2-signal hyperintensity is greater in the left than the right mesial temporal lobes (white arrows) |
|
|
How long must an alcoholic patient be sober before assessment of dementia? |
At least 2 months, and treatment with alcohol cessation may result in some improvement |
|
|
Presentation of alcohol-related dementia (4) |
1. Frontal-dysexeccutive disorder with poor working memory 2. Inattention 3. Impaired judgement 4. Poor verbal fluency |
|
|
Triad of Wernicke-Korsakoff syndrome |
1. Global confusion 2. Truncal ataxia 3. Ophthalmoplegia or nystagmus |
|
|
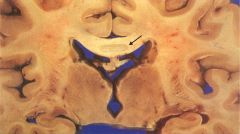
Brain with Marchiafava-Bignami disease. Note discoloration of the central portion of corpus callosum (arrow). Microscopic examination would show demyelination and necrosis |
|
|
Korsakoff syndrom consists of |
1. Anterograde amnesia and retrograde amnesia; recent memory is usually affected more than remote memory 2. Often confabulate early in the course |
|
|
This disease was initially described in drinkers of Italian red wine, but it has since been described in others with chronic alcoholism associated with other alcoholic beverages |
Marchiafavia-Bignami disease |
|
|
Hallmark finding in Marchiafava-Bignami disease is |
demyelination in the corpus callosum, usually involving the central regions |
|
|
MRI findings in Marchiafava-Bignami disease? |
Callosal enhancement early on and T2-signal changes and atrophy in the later stages |
|
|
Patients with a B12-deficiency may, in addition to dementia, present with which features? (4) |
1. Neuropsychiatric symptoms 2. Coexisting optic atrophy 3. Peripheral neuropathy 4. Subacute combined degeneration of the spinal cord |
|
|
The three ds of Pellagra? |
Diarrhea, dermatitis, and dementia, which at times may be rapidly progressive, mimicking CJD |
|
|
Inherited metabolic diseases that are associated with dementia? (4) |
1. Mitochondrial disorders 2. Inherited leukodystrophies 3. CADASIL 4. Lysosomal storage disorders (e.g., Neimann-Pick disease) |
|
|
One inherited disorder that deserves mention |
Adult polyglucosan body disease, beccause its presentation is often late in adulthood with an onset between the firth and seventh decades of life |
|
|
Presenting features of adult polyglucosan body disease (4) |
1. Dementia 2. Peripheral neuropathy 3. Neurogenic bladder 4. UMN signs |
|
|
Repetitive head trauma increases the risk of (3) |
1. Alzheimer disease 2. Chronic traumatic encephalopathy 3. Perhaps other neurodegenerative diseases |
|
|
Clinical features of postconcussive syndrome |
1. Inattention 2. Impaired working memory 3. Psychomotor slowing 4. Dizziness 5. Posttraumatic headache and psychiatric symptoms |
|
|
Which brain regions are most commonly affted by cerebral contusions? |
The frontotemporal regions |
|
|
Chronic traumatic encephalopathy is also called |
Dementia puilistica |
|
|
Unilateral temporal lobe injury may cause |
Learning and memory troubles |
|
|
Bilateral anterior temporal lobe lesions may cause |
Klüver-Bucy syndrome (hyperorality, hypersexuality, hypermetamorphosis, and docility) |
|
|
Underlying mechanism of chronic traumatic encephalopathy? |
Newer studies have shown that chronic traumatic encephalopathy is often associated with underlying tau abnormality and have suggested it be considered a progressive tauopathy |
|
|
Which MRI sequences may be helpful in the diagnosis of chronic traumatic encephalopathy? |
MRI using gradient echo sequences or susceptibility-weighted imaging, which is sensitive to hemosiderin deposition and may be helpful |
|
|
What are Lundberg waves? |
Intracranial pressure waveform |
|
|
Clinical presentation of normal pressure hydrocephalus? |
Gait disturbance (magnetic gait), urinary incontinence, and dementia |
|
|
The dementia in NPH is thought to be due to? |
Hydrocephalus impinging on periventricular frontostriatal projections |
|
|
MRI findings in NPH |
1. Ventriculomegaly out of proportion to cortical atrophy 2. Loss of sulci superiorly 3. Periventricular white matter changes from transependymal flow and a T2-signal hypointense flow void in the cerebral aqueduct |
|
|
Is OSA an independent risk factor for cognitive impairment? |
Yes; suggested pathomechanism have included hypoxemia resulting in subsequent reperfusion brain injury, endothelial dysfunction causing a vascular-type dementia, and excessive daytime somnolence affecting daily functioning |
|
|
What is Ganser syndrome? |
A form of dementia where the answers are always nearly correct but still incorrect, may occur in pseudodementia but is also present with malingering |
|
|
What is a fugue |
A psychiatric disorder characterized by reversible amnesia for personal identity that may last hours to months |