![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Deviation of the chin may suggest X mandible fracture. |
Deviation of the chin may suggest condyle fracture. |
|
|
|
What is meant by tension band & stabilization plate in mandible fx? Where are these placed? |
Tension band and stabilization plate: A small plate is placed at the alveolar border to neutralize tensile forces; a larger plate is placed at the inferior border to neutralize compression and torsional stresses. |
|
|
|
Functional stability, provided solely by the fixation system, is accomplished only by reconstruction plates is called... |
Load-bearing stability |
|
|
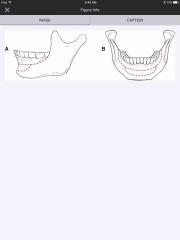
What do these lines depict? |
Champy lines of ideal osteosynthesis. |
|
|
|
Condyle fracture without malocclusion treatment? |
Soft diet & close observation. Treat with arch bars/elastics if malocclusion develops. |
|
|
|
General type of blood vessels that supply the flat bones of the facial skeleton? |
Flat bones of the facial skeleton, as well as the scapulae, sternum, and ribs, do not contain a diaphysis, metaphyses, or epiphyses. They contain a dual blood supply with nutrient arteries (generally based off of the maxillary artery or middle meningeal artery for the calvaria) and the periosteal vessels and vascular plexus. |
Blood supply is dual. |
|
|
Are lag screws in the mandible load bearing or load sharing? |
Examples of load-sharing osteosynthesis include lag screw fixation, maxillomandibular fixation, nonlocking mandibular border plate, and monocortical miniplate (Champy principle) fixation. |
|
|
|
What is the treatment for patients with a 1x1 cm area of exposed mandible 2/2 bisphosphonate induced necrosis, no pain, no fracture? |
Ruggiero et al. proposed a three-stage classification system and treatment algorithm for bisphosphonate-related osteonecrosis of the jaw Stage 1- exposed and necrotic bone that is otherwise asymptomatic, as in the patient described above. Antiseptic mouth rinse & observation. Stage 2 - exposed and necrotic bone with pain and clinical evidence of infection. Antiseptic mouth rinses, oral antibiotics, and superficial debridement are recommended for this stage. Stage 3 - the features of Stage 2 and one or more of the following: pathologic fracture, extraoral fistula, and osteolysis extending to the inferior mandibular border. Stage 3 patients require surgical debridement or resection in addition to antiseptic mouth rinses and oral antibiotics. Dental extraction of infected, unsalvageable teeth should be performed, but extractions may also result in further nonhealing wounds and bone exposure. |
|
|
|
62-year-old woman who underwent chemotherapy/radiation protocol for oropharyngeal cancer 10 years ago has onset of severe pain after a dental extraction. Subsequent CT scan shows a pathologic fracture of the mandibular angle. What is the most appropriate management? |
Free fibula. The most common cause of pathologic fracture after radiation therapy in the mandible is tooth extraction, usually the third molar, and a subsequent angle injury, as in this case. With a large, multi-decade experience in the use of osseous free flaps, especially the fibular flap, these cases are now routinely managed by resection of the affected bone and immediate reconstruction. |
|
|

A 25-year-old man is brought to the emergency department 2 hours after being punched in the left side of the face. Physical examination shows swelling on the left side of the face. The panoramic x-ray study (Panorex) shown was obtained. Which of the following is the most appropriate management? A) Extraction of all components of the third left mandibular molar and maxillomandibular fixation (MMF) for 2 weeks B) Extraction of all components of the third left mandibular molar and MMF for 6 weeks C) Extraction of all components of the third left mandibular molar, MMF, and open reduction and internal fixation (ORIF) D) Ligating the third left mandibular molar to the adjacent tooth for stability, MMF, and ORIF E) Preservation of the third molar, MMF, and ORIF |
C) Extraction of all components of the third left mandibular molar, MMF, and open reduction and internal fixation (ORIF) There's also a parasymphyseal fracture! |
|
|
|
How are teeth numbered? |
Standard numbering of the dentition of the maxillary dental arch from right to left is No. 1 to No. 16. The mandibular dental arch from left to right is No. 17 through No. 32. |
|
|

A 56-year-old woman with type 1 diabetes mellitus has a six-month history of a slowly enlarging, painless mass in the mandible. She is edentulous. Physical examination shows a 4-cm mass on both the buccal and lingual portions of the alveolus with intact mucosa. A panoramic radiograph (Panorex) is shown. Biopsy confirms ameloblastoma. Which of the following is the most definitive management?
A ) Conservative segmental resection of the mandible, followed by nonvascularized iliac crest cortical bone grafting B ) Curettage and cancellous bone grafting C ) Segmental resection of the mandible with wide margins and cervical lymph node dissection, followed by vascularized free fibular bone grafting D ) Segmental resection of the mandible with wide margins and cervical lymph node dissection, followed by vascularized free fibular bone grafting and adjuvant radiation therapy E ) Segmental resection of the mandible with wide margins, followed by vascularized free fibular bone grafting
|
The correct response is Option E. The history and radiographic findings in the patient described are most consistent with multicystic ameloblastoma. This odontogenic tumor commonly presents as a painless enlarging mass in the mandible or, less commonly, in the maxilla. The typical radiographic finding is a multilocular lucency with preservation of the cortex, though the cortex may be thinned. There are subcategories including peripheral (extraosseous) and central (intraosseous), which may be unicystic or multicystic, as in the radiograph shown. Extraosseous lesions may have no radiographic findings. This tumor goes beyond the boundaries seen on radiograph.
Wide resection is necessary for multicystic lesions to prevent recurrence. The sizeable defect resulting from wide resection in the patient described would be best treated with vascularized bone graft, especially in light of her diabetes. |
|
|

A 27-year-old man is admitted to the emergency department after being injured in an altercation. Physical examination shows objective malocclusion with a left-sided crossbite and right-sided open bite. A CT scan is shown. Which of the following muscles is most likely responsible for these radiographic and physical examination findings?
A) Genioglossus B) Lateral pterygoid C) Masseter D) Medial pterygoid E) Mylohyoid |
Lateral pterygoid. Medial pterygoid & masseter displace during angle and body fx |
|
|
|
Between which 2 planes is submandibular approach to mandible fractures performed? Landmark to make incision? |
The submandibular approach to facial fractures involves incising the skin 2 cm below the mandibular border, dividing the platysma and dissecting deep to the investing fascia, just above the submandibular gland. Once in this plane, the course of dissection is carried superiorly toward the mandibular border.
|
|
|
|
An isolated mandible fracture had a ___% relationship with a cervical spine injury. |
An isolated mandible fracture had a 5.1% relationship with a cervical spine injury. |
|
|
|
Which of the following provides the most significant blood supply to the mandibular condylar head?
A) Articular disk B) Capsule of the temporomandibular joint C) Deep branch of the superficial temporal artery D) Facial artery E) Medullary branch of the inferior alveolar artery |
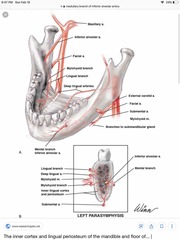
E) Medullary branch of the inferior alveolar artery |
|
|
|
With condylar & subcondylar fractures, which side has an open bite & which side has a cross bite? |
typical findings of condylar/subcondylar fractures: ipsilateral crossbite and contralateral open bite |
|
|
|
22-year-old man is evaluated because of a painless, firm, unilateral enlarging mass of the body of the mandible. He denies trauma to the area and he has excellent oral hygiene. His dentist performed fine needle biopsy that showed multinucleated giant cells. CT scan shows a radiolucent bone lesion with an expanded cortex. Which of the following is the most appropriate next step in management? What is the lesion? A) Incisional biopsy B) Partial mandibulectomy with free margins C) Radiation therapy D) Resection and curettage E) Sclerotherapy |
D) Resection and curettage This patient has an aneurysmal bone cyst (ABC). These lesions may be related to giant cell granulomas. These lesions are most common in the long bones with 1.9% of them being reported in the mandible.
The correct answer is resection and curettage. In a study of 120 ABC cases, resection and curettage was reported to have a 91.8% success rate (recurrence occurred in 11 out of 120 cases). Incomplete resection is hypothesized to be a cause of recurrence. Recurrence was not related to histopathologic parameters. |
|
|
|
Key treatment for ameloblastoma? |
Partial mandibulectomy with free margins is the preferred treatment for lesions like ameloblastomas. Given the efficacy of excision and curettage, mandibulectomy is not the recommended first line treatment for this diagnosis. It can be employed in recurrences (although as stated above, less aggressive interventions are typically employed first).
|
|
|
|
How long should MMF be employed for subcondylar fractures? What about comminuted bilateral intracapsular mandible fractures? |
Maxillomandibular fixation (MMF) for 4 to 6 weeks 2 weeks for intracapsular |
|